4074
Why MRI? Evaluating Acute Abdominal and Pelvic Pain During Pregnancy.1Medical College of Georgia at Augusta University, Augusta, GA, United States, 2Feinberg School of Medicine, Chicago, IL, United States, 3Radiology and Imaging Sciences, Emory University School of Medicine, Atlanta, GA, United States, 4Radiology and Imaging, Medical College of Georgia at Augusta University, Augusta, GA, United States
Synopsis
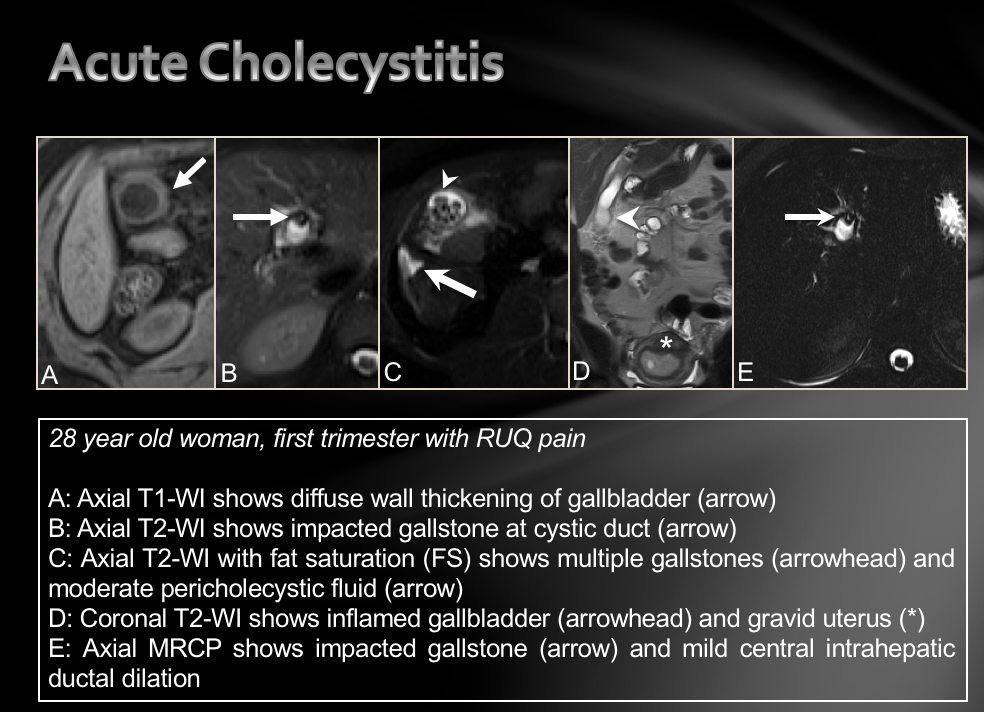
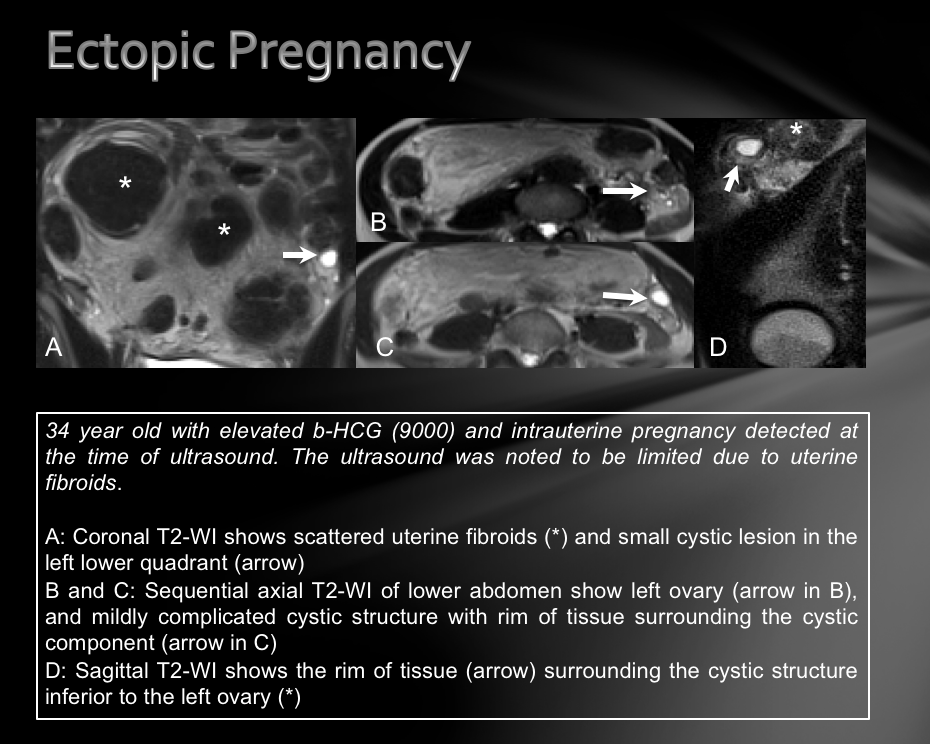
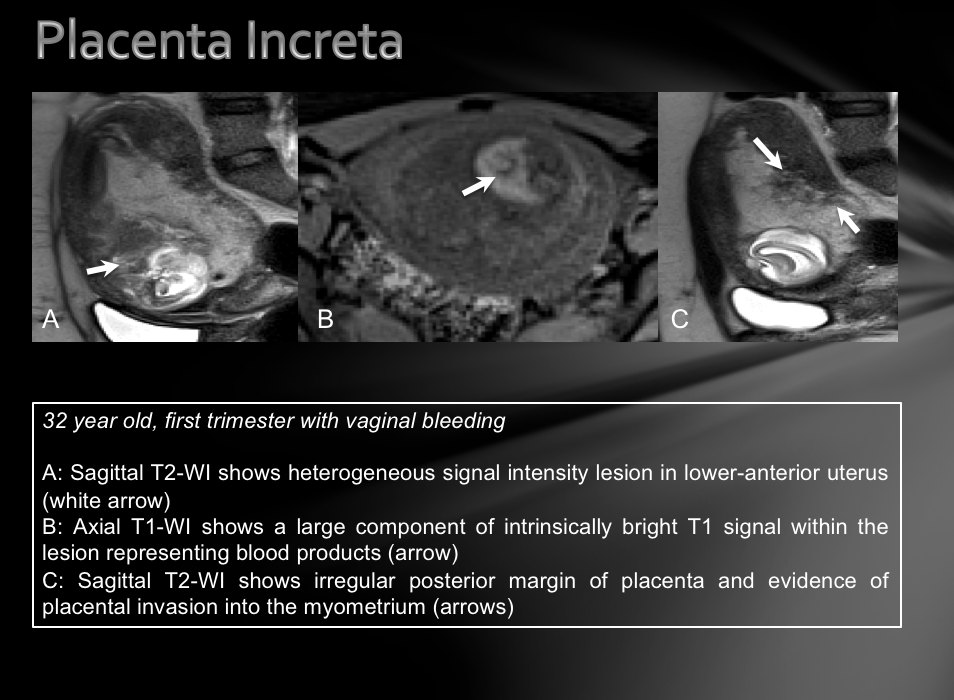
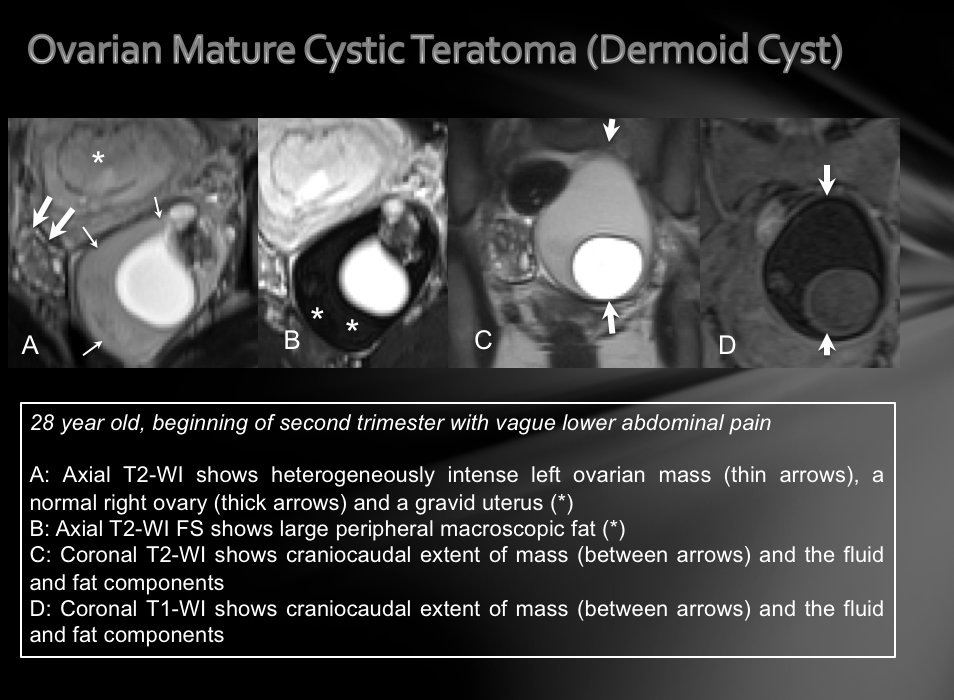
A variety of pathological processes can be the cause of abdominopelvic pain during pregnancy, such as acute appendicitis, acute cholecystitis, hepatic adenoma, spontaneous adrenal hemorrhage, ovarian mature cystic teratoma, ectopic pregnancy, cystic degeneration of an intramural fibroid, and the placenta accreta spectrum. Standard MRI protocols without gadolinium contrast are discussed, as well as protocols for fluid sensitive sequences with and without fat suppression, T1-weighted sequences, and thin slice sequences. These MR imaging techniques are valuable in determining an accurate diagnosis and subsequent management plan for the mother and fetus.
Learning Goals
1. To determine the various causes of abdominopelvic pain during pregnancy and their magnetic resonance imaging characteristics.
2. The role of MRI as a safe imaging modality during pregnancy due to its excellent soft tissue contrast and multiplanar capabilities, as opposed to computed tomography and ultra sound imaging.
3. Demonstrate important elements in the assessment and management of abdominopelvic pain during pregnancy.
Background Information and Content
This exhibit reviews evaluating acute abdominal and pelvic pain during pregnancy with magnetic resonance imaging. The magnetic resonance imaging obtained in the cases presented were important diagnostic tools used in the investigation of these various pathological processes. Managing acute abdominopelvic pain in pregnancy is challenging due to the variety of differential diagnoses (ranging from obstetrical and gynecological to abdominal pathologies), limited value of laboratory tests, and the anatomical and physical alterations that occur during pregnancy1. Ultra sound imaging can be limited in advanced pregnancies due to overlying bowel gas, the gravid uterus, and pregnancy related obesity1. Computed tomography is not desirable for imaging pregnant women because of the potential of fetal harm from radiation2. Thus, magnetic resonance imaging has become increasingly useful in evaluating abdominal pain in pregnancy. The American College of Radiologists concluded that MRI at 1.5 T is safe in pregnancy, irrespective of fetal gestational age. The multiplanar technique and wide field view of MR make it possible to image the anatomical changes that make the ultra sound imaging modality limited2. Accurate detection and diagnosis of pregnant women presenting with acute abdominal pain is extremely important because treatment delay worsens the outcome for both the mother and the fetus2.Key Anatomic, Pathophysiologic Issues, Imaging findings, and Imaging Technique
Most causes of abdominal and pelvic pain during pregnancy are benign and require no specific treatment or supportive measures only. The purpose of this project is to investigate cases where MR imaging was utilized in diagnosing abdominopelvic pain during pregnancy and discuss the MR imaging protocol used. The MRI protocols and their advantages over other modalities are discussed in the cases presented, which include the most common indications for emergent surgery during pregnancy - acute appendicitis being the most common (occurring in 1 in every 1400-6600 pregnancies) and acute cholecystitis being the second most common3. Hepatic adenoma, spontaneous adrenal hemorrhage, ovarian mature cystic teratoma, ectopic pregnancy, cystic degeneration of an intramural fibroid, and the placenta accreta spectrum (the most common cause of emergent postpartum hysterectomy) are also discussed. The MR imaging characteristics presented are protocols that maximize the yield for diagnosing inflammatory causes of abdominopelvic pain (fluid sensitive sequences with and without fat suppression), T1-weighted sequences beneficial in detecting blood products and other proteinaceous fluids, and thin slice sequences used in cases requiring fine anatomic detail.Conclusions
1. When ultrasound examination is limited or non-diagnostic, non-contrast magnetic resonance imaging is safe and effective for diagnosing and directing subsequent management in many cases of abdominal and pelvic pain during pregnancy and the peripartum period.
2. MRI has superior soft tissue contrast and multiplanar capabilities when compared to computed tomography and ultra sound, and MRI does not expose the patient, nor the fetus, to ionizing radiation, as opposed to CT.
3. Radiologists should be familiar with protocoling and interpreting abdominal and pelvic MRIs in pregnant patients in order to guide management of both the mother and the fetus by providing diagnoses for abdominopelvic pain.
Acknowledgements
No acknowledgement found.References
- Amitai MM, et al. Role of Emergency Magnetic Resonance Imaging in the Workup of Suspected Appendicitis in Pregnant Women. Israel Medical Association Journal. 2016;18(10): 600-604.
- Casciani E, et al. Errors in Imaging the Pregnant Patient with Acute Abdomen. Abdominal Imaging. 2015;40(7):2112-2126.
- Beddy P, et al. Magnetic Resonance Imaging for the Evaluation of Acute Abdominal Pain in Pregnancy. Seminars in Ultrasound, CT and MRI. 2010;31(5):433–441.
Figures