4070
Comparison of fetal lung diffusivity in cases of pulmonary hypoplasia to normative MRI dataClemente Velasco‐Annis1, Ali Gholipour1, Judy A. Estroff1, Richard B. Parad2, Terry L. Buchmiller1, Carol E. Barnewolt1, Sila Kurugol1, Simon K. Warfield1, and Onur Afacan1
1Boston Children's Hospital and Harvard Medical School, Boston, MA, United States, 2Brigham and Women's Hospital and Harvard Medical School, Boston, MA, United States
Synopsis
Typically the fetal lungs are measured using structural magnetic resonance (MRI) or ultrasound images, but improvements in fetal MR imaging have made diffusion weighted imaging (DWI) feasible for even fetal patients. Previously it was shown that lung diffusion could be reliably measured for fetuses with normal lung development and that diffusivity increased with gestational age (GA). In this study we applied the same techniques to measure lung diffusivity in patients indicated for congenital diaphragmatic hernias. We then compared diffusivity measurements for both the herniated-side, left lung and right lung to normative lung diffusivity data.
Introduction
Characterizing the development of the fetal lungs is critical for the medical care of fetal lung abnormalities such as pulmonary hypoplasia (PH), the incomplete development of the lungs, such as in cases of congenital diaphragmatic hernia (CDH). Non-invasive, in-utero imaging and analysis informs parents and healthcare providers information on the severity of the abnormality, its survivalbility, whether early intervention is needed, as well as planning for the birth and post-birth care of the fetus. Typically the fetal lungs are measured using structural magnetic resonance (MRI) or ultrasound images, but improvements in fetal MR imaging have made diffusion weighted imaging (DWI) feasible for even fetal patients. Previously it was shown that lung diffusion could be reliably measured for fetuses with normal lung development and that diffusivity increased with gestational age (GA)1, theoretically due to decreased interstitial tissue and increased capillary growth throught gestation . In this study we applied the same techniques to measure lung diffusivity in patients indicated for congenital diaphragmatic hernias. We then compared diffusivity measurements for both the herniated-side, left lung and right lung to normative lung diffusivity data.Methods
46 subjects were imaged on Siemens 3T Skyra scanners, including 37 control subjects and 9 patients who were indicated for a left-sided congenital diaphragmatic hernia (mean GA =28.28±5.71 weeks). Diffusion weighted scans were acquired using multi-slice single shot Echo Planar Imaging (EPI) sequences with 6 b-values (0, 50, 100 200, 400, 600 (sec/mm2). The imaging paramters were as follows: In-plane resolution, ranging between 2-2.66mm x 2-2.66mm; Repitition Time TR)=4400-6700ms; and Echo Time (TE)=60-75ms. During the clinical CDH exams, 19 lung diffusion scans were acquired in total. Two acquisitions with severe fetal motion were eliminated from further processing leaving 17 DWI scans which could be measured for analysis. The region of interest (ROI) was selected for each lung manually (figure 1). The extent of PH in the clinical cases varied, ranging from “favorable” assessments to having almost no distinguishable lung tissue present, particularily for the left lung. In cases where the left lung could not be confidently differentiated from the hernia, the lung was located using landmarks visible in structural imaging acquired during the same exam (figure 2). An apparent diffusion coefficient (ADC) value was calculated, excluding the B=0 image, using a robust maximum likelihood based curve fitting procedure.Results
Statistical analysis was performed using multiple linear regression, where median ADC measurements of each lung for each subject were used as outcome and GA and the presence of CDH were used as independent variables. Both left lung ADC (LADC) and right lung ADC (RADC) for left-sided CDH cases correlated with GA significantly (p≤.005). LADC significantly differed versus control subject ADC (p≤.05), whereas RADC did not. In Figure 3, LADC and RADC has been plotted against the normative ADC values from control cases.Discussion and Conclusions
These results suggest that the decreased diffusivity of under-developed fetal lungs in cases of CDH-induced PH, as compared to that of control subjects, can be detected using diffusion-weighted MRI. The ability to characterize the functionality of in-utero fetal lungs may improve the medical care of PH patients, which currently relies on volumetric measurements.Acknowledgements
This research was supported in part by the following grants: NIH-R01EB019483, NIH-R01NS079788, NIH-R01EB018988 and a grant from Fetal Health Foundation.References
Afacan, O., Gholipour, A., Mulkern, R.V., Barnewolt, C.E., Estroff, J.A., Connolly, S.A., Parad, R.B., Bairdain, S. and Warfield, S.K., 2016. Fetal lung apparent diffusion coefficient measurement using diffusion‐weighted MRI at 3 Tesla: Correlation with gestational age. Journal of Magnetic Resonance Imaging, 44(6), pp.1650-1655.Figures
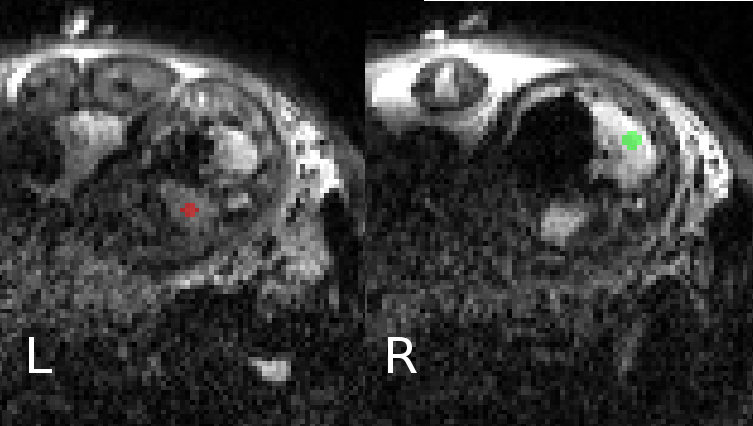
Figure 1. This figure shows ROI placement on the diffusion weighted images. Each lung for CDH cases was separately labelled. The expert segmented the images using B0 images as well as higher B value images and also checked for motion between images.
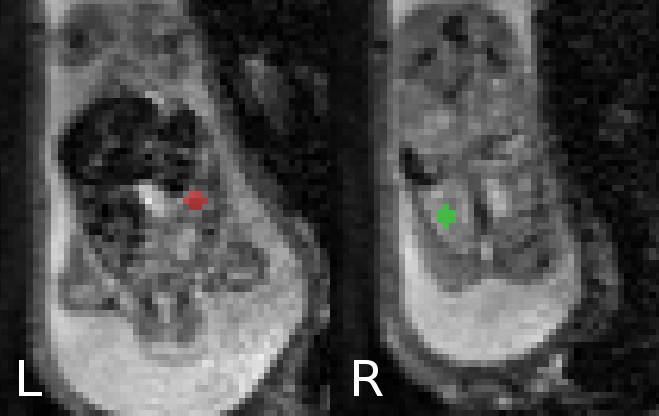
Figure 2. Another example where CDH lung was segmented using diffusion weighted images as well structural HASTE and TRUEFISP images to improve segmentation in cases where lung volume was small.
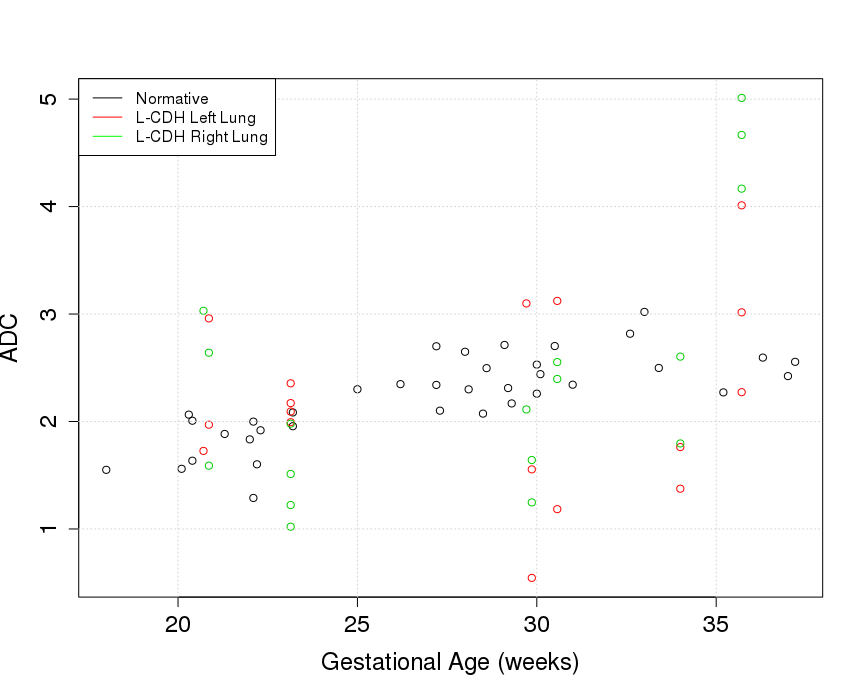
Figure 3. Apparent diffusion coefficient results plotted against gestational age. Black dots represent cases with normal lung development. All patients used in this plot were left sided CDH cases. Red dots show left lung ADC values and green dots show right lung ADC values.