4068
Assessment of placental microcirculation by joint analysis of flow compensated and non-flow compensated intravoxel incoherent motion data1Fetal-Neonatal Neuroimaging & Developmental Science Center, Boston Children's Hospital, Boston, MA, United States, 2Department of Electrical Engineering and Computer Science, Massachusetts Institute of Technology, Cambridge, MA, United States, 3Computer Science and Artificial Intelligence Laboratory (CSAIL), Massachusetts Institute of Technology, Cambridge, MA, United States, 4Department of Pathology, Massachusetts General Hospital, Boston, MA, United States, 5Athinoula A. Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Charlestown, MA, United States, 6Department of Radiology, Harvard Medical School, Boston, MA, United States, 7Harvard-MIT Division of Health Sciences and Technology, Massachusetts Institute of Technology, Cambridge, MA, United States, 8Institute for Medical Engineering and Science, Massachusetts Institute of Technology, Cambridge, MA, United States, 9Maternal-Fetal Medicine, Obstetrics and Gynecology, Massachusetts General Hospital, Boston, MA, United States, 10Psychiatry Neuroimaging Laboratory, Brigham and Women’s Hospital and Harvard Medical School, Boston, MA, United States
Synopsis
Using diffusion weighted imaging and the intravoxel incoherent motion model (IVIM) of blood flow in capillaries, we can measure placental properties relating to maternal and fetal blood flow and perfusion. In this study, we focused on improving the accuracy and precision of the estimated parameters in IVIM imaging by using joint analysis of flow compensated and non-flow compensated diffusion data. With flow compensation, we observed strong re-phasing, approximately cancelling the blood flow effect and allowing more accurate and consistent estimation of diffusion and perfusion measures.
Introduction
The placenta is dually perfused by the maternal and fetal circulations. It has a heterogeneous tissue microstructure with a broad variety of villous structures and perfusion functions. Diffusion weighted imaging and the intravoxel incoherent motion model (IVIM) of blood flow in capillaries can be used to determine placental morphological and physiological characteristics. Previous studies using the IVIM model have shown differences in placental perfusion fraction maps between normal and growth-restricted pregnancies.1-4 In this study we proposed to use a joint analysis of flow compensated (FC) and non-flow compensated (NFC) IVIM data in the placenta to improve the accuracy and precision of the estimated IVIM parameters. This approach has been previously used and validated on in vivo liver, pancreas and brain data,5,6 and here we apply it to the placenta.Methods
In this IRB approved study, four subjects with gestational ages of 25w+1d, 29w+2d, 32w+6d and 33w were scanned. Scans were performed on a 3T Skyra scanner (Siemens Healthineers, Erlangen, Germany) using the following protocol: EPI readout, TR = 7900ms, TE = 76ms, BW= 1830Hz/pixel, 2.6×2.6×2mm3 voxel size, ~70 slices covering whole uterus, two diffusion encoding directions, b = 0, 15, 30, 60, 90, 110, 150, 225, and 300s/mm2, total scan time = 5:32min (two 2:46min acquisitions with and without flow compensation). We corrected signal non-uniformity and motion using our previously demonstrated computational pipeline.7 For inter-volume motion correction, all volumes with b>0 were aligned to the b=0s/mm2 volume acquired with non-flow compensated diffusion encoding. Data analysis was performed in Matlab. For conventional IVIM analysis a bi-exponential model (S(t)=S0((1-f)e-bD+fe-bD*) was used for nonlinear data fitting, with S0 (MRI signal without diffusion encoding), f (intravoxel fraction of flowing water in perfused capillaries), D (diffusion coefficient) and D* (pseudo diffusion coefficient) as free parameters. In joint analysis, the tissue diffusion coefficient D was estimated by mono-exponential signal fitting using the FC data with b ≥ 90s/mm2, then the other parameters in the IVIM model, f and D*, were estimated using NFC data. Voxel-wise IVIM parameters were computed using the averaged signal intensity values over a 3×3×3 neighborhood to achieve a better signal-to-noise ratio (SNR).Results
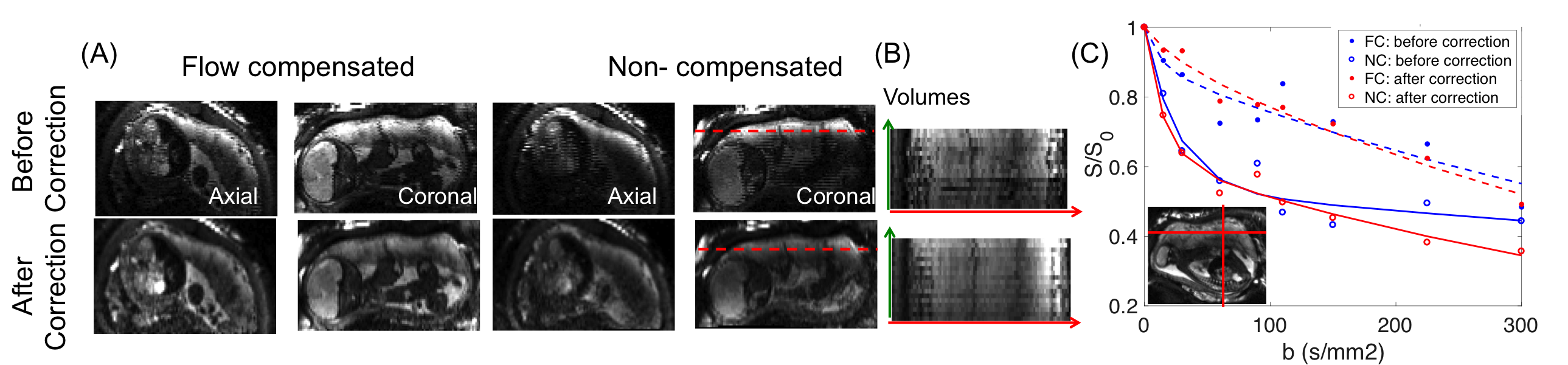
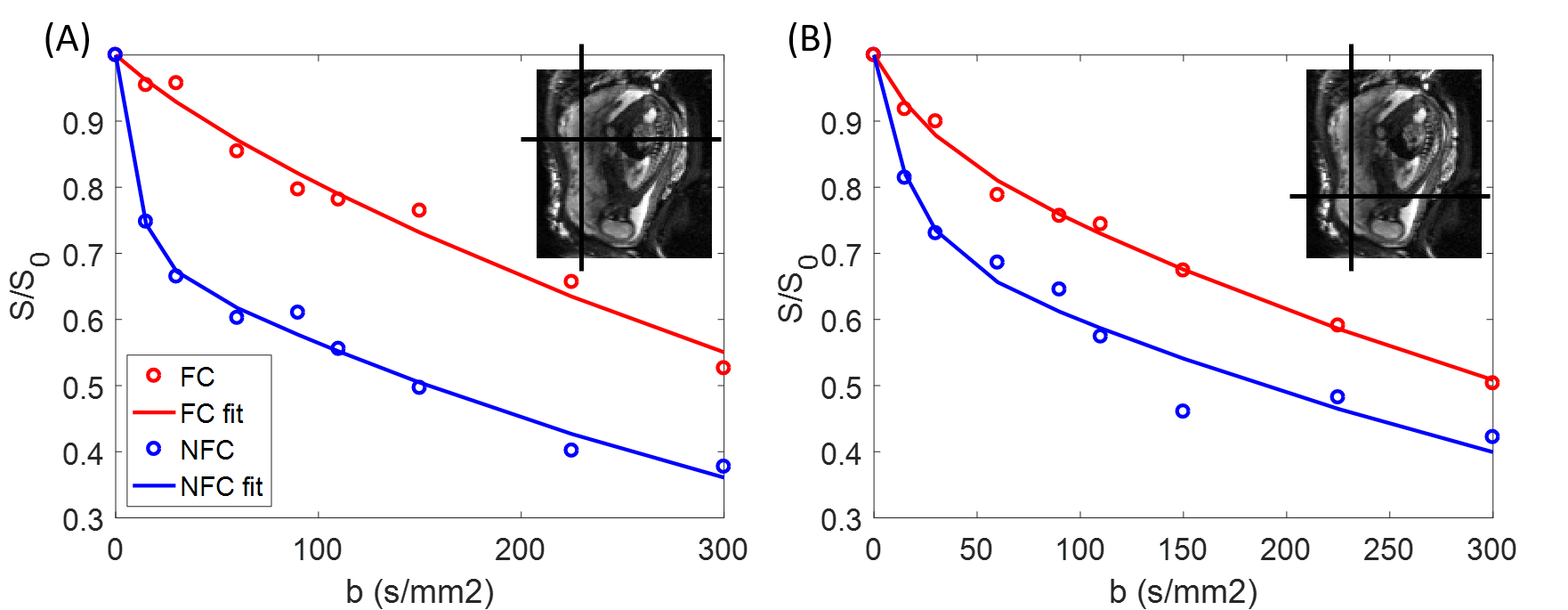
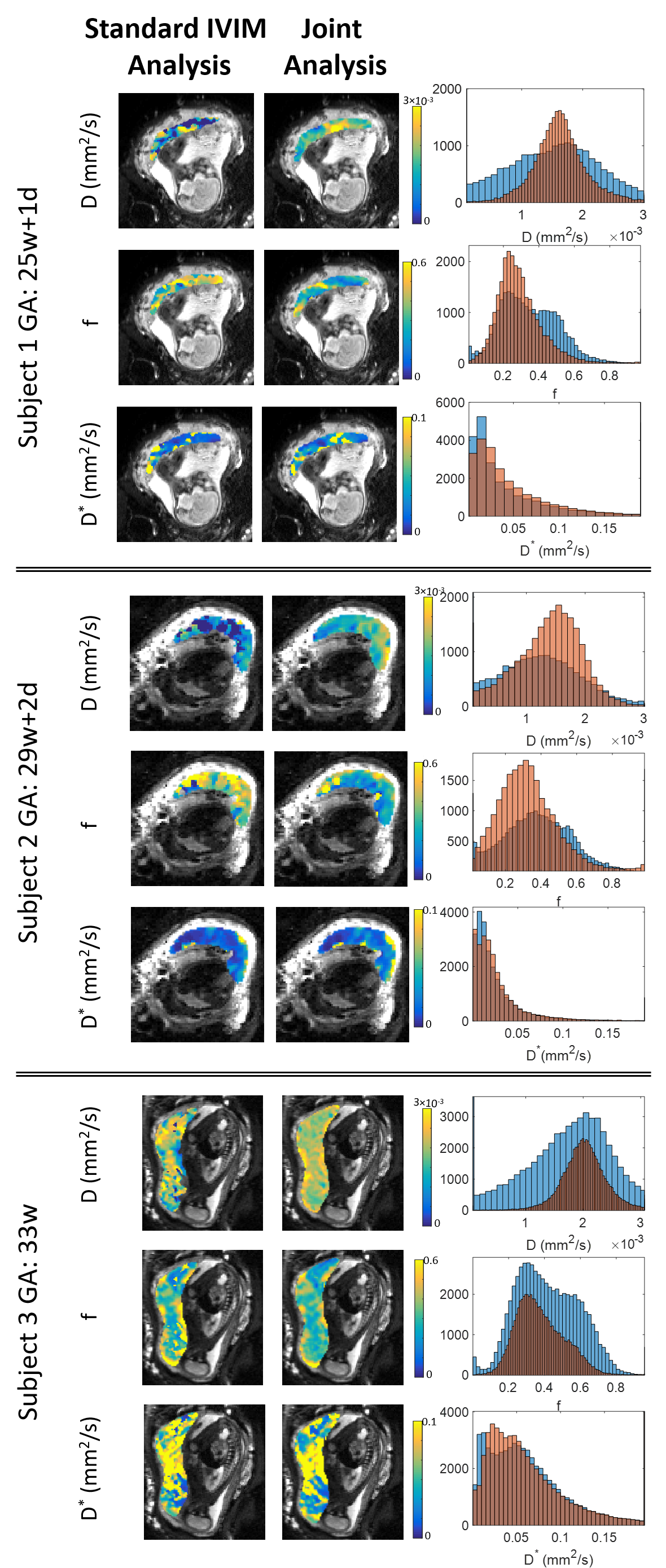
One subject was excluded due to a contraction during FC data acquisition. For the other three subjects both standard IVIM analysis and FC-NFC joint IVIM analysis was performed. Figure 1A shows orthogonal views of b=0 s/mm2 image before and after signal non-uniformity and motion correction. The signal intensity at the dotted line in (1A) over volumes shows less fluctuation after motion correction (Figure 1B). Figure 1C shows the improvement in voxel-wise model fitting after correction. Figure 2 shows bi-exponential model fittings with NFC and FC data at two different placental locations, separately. Similar to the previous study performed in the liver,5 the signal attenuation in NFC data was larger than the signal attenuation in FC data at the same b-values in the placenta. More obvious separation between FC and NFC attenuation curves in Figure 2A than 2B is reflected by a larger f in this region (i.e. 0.39 vs. 0.24). In Figure 2B, the higher signal attenuation observed in FC data compared to Figure 2A might be due to the incoherent blood motion in a capillary network with high velocity that cannot be fully compensated. Figure 3 shows parameter maps obtained by voxel-wise fitting of the standard IVIM model and FC-NFC joint IVIM model for each subject, along with histogram plots generated for whole placenta for each parameter. While we observed two peaks in the perfusion fraction histogram plots using standard IVIM model, after joint analysis the distribution was more homogenous.Discussion
We sought to improve the accuracy and precision of the estimated parameters in IVIM imaging using joint analysis of flow compensated and non-flow compensated diffusion data. With flow compensation, we observed strong re-phasing, i.e. decrease of the IVIM effect, which provides more accurate diffusion measures and thus, physiologically more accurate and spatially consistent perfusion fraction maps. This feasibility study provides preliminary evidence for using the proposed method for reliable estimation of blood perfusion measures in the placenta. However, parameter estimates need to be validated using other independent techniques. Fetal pulsatile flow closer to the chorionic plate and heterogeneous vascular structure might affect FC interpretation, which needs to be taken into account in future studies. As a next step, we will test joint analysis with a multi-compartment model to account for rapid and slow motion in fetal capillaries and maternal lakes, separately.Acknowledgements
This project is supported by NIH R01 EB017337, NIH U01 HD087211.References
1. Moore, R. J., Strachan, B. K., Tyler, D. J., Duncan, K. R., Baker, P. N., Worthington, B. S., Johnson, I. R. & Gowland, P. A. In utero perfusing fraction maps in normal and growth restricted pregnancy measured using IVIM echo-planar MRI. Placenta 21, 726–732 (2000).
2. Derwig, I., Lythgoe, D. J., Barker, G. J., Poon, L., Gowland, P. A., Yeung, R., Zelaya, F. & Nicolaides, K. Association of placental perfusion, as assessed by magnetic resonance imaging and uterine artery Doppler ultrasound, and its relationship to pregnancy outcome. Placenta 34, 885–891 (2013).
3. Sohlberg, S., Mulic-Lutvica, A., Lindgren, P., Ortiz-Nieto, F., Wikström, A. K. & Wikström, J. Placental perfusion in normal pregnancy and early and late preeclampsia: A magnetic resonance imaging study. Placenta 35, 202–206 (2014).
4. Sohlberg, S., Mulic-Lutvica, A., Olovsson, M., Weis, J., Axelsson, O., Wikström, J. & Wikström, A. K. Magnetic resonance imaging-estimated placental perfusion in fetal growth assessment. Ultrasound Obstet. Gynecol. 46, 700–705 (2015).
5. Wetscherek, Andreas, Bram Stieltjes, and Frederik Bernd Laun. Flow compensated intravoxel incoherent motion diffusion imaging. Magnetic resonance in medicine 74.2 (2015): 410-419.
6. Ahlgren, André, et al., Quantification of microcirculatory parameters by joint analysis of flow-compensated and non-flow-compensated intravoxel incoherent motion (IVIM) data. NMR in Biomedicine 29.5 (2016): 640-649.
7. Abaci Turk, Esra, et al., Spatiotemporal alignment of in utero BOLD‐MRI series. Journal of Magnetic Resonance Imaging 46.2 (2017): 403-412.
Figures