4067
Classification and prognosis of fetal hepatic hemangioendothelioma using MRI1MRI, Shandong Medical Imaging Research Institute, Shandong University, Jinan, China, 2Ultrasound, Shandong Medical Imaging Research Institute, Shandong University, Jinan, China, 3MR Collaboration AP, Siemens Healthcare, MR Collaboration AP, Beijing, China, 4Obstetrics, Jinan Maternity and Child Care Hospital, Jinan, China
Synopsis
The aim of this study was to investigate the MRI features and classification of 23 fetal hepatic hemangioendothelioma (HAE) and to compare the prognosis of HAE-I and HAE-II. The results showed that fetal HAE-I tends to be more vascular in the lesion, and the larger the focus, the more prone to complications. Once complications occur, the prognosis is poor; however, in HAE-II, the lesions are always smaller, there is a lack of vascularity, they are homogeneous, and the prognosis is good. Our study demonstrated that the MRI features and classification of HAE can effectively predict and guide prognosis.
Introduction
Congenital tumors represent only 1.5 – 2% of all pediatric tumors, with a prevalence of 1 in 12,500 – 27,500 live births [1, 2]. Hepatic tumors comprise about 5% of all congenital neoplasms, of which the most common (60%) is the hemangioendothelioma (HAE). Although benign by pathology, the clinical expression of HAE is extremely variable and ranges from asymptomatic to life-threatening complications in utero [3, 4]. Nowadays, magnetic resonance imaging (MRI) is a useful complementary tool to assess anomalies in fetuses. Our study aims to explore the MRI features and classification, and to compare the prognosis of different types of fetal HAE.Materials and methods
From January 2015 through October 2018, a total of 48 pregnant women with suspected fetal HAE (screened by ultrasound) underwent prenatal liver MRI examinations at our institute. In all cases, the prenatal diagnosis was confirmed by postnatal examination findings, including MRI / computed tomography (CT) and serial US examinations, or pathology. Exclusion criteria: poor image quality, incomplete clinical data, insufficient follow-up, and additional structural abnormalities not caused by HAE.
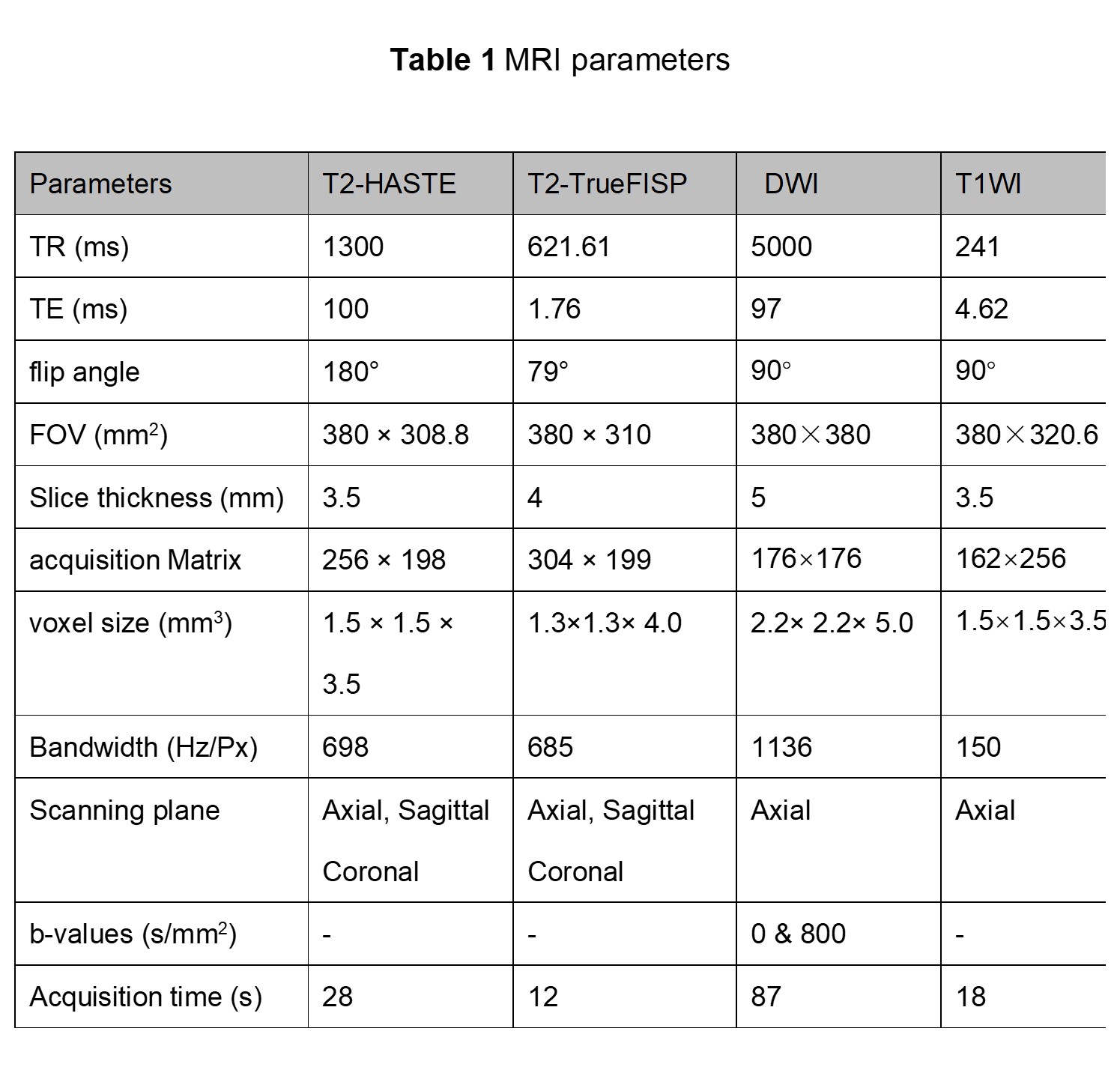
The MRI examinations were performed on a 1.5 T MAGNETOM Amira (Siemens Shenzhen Magnetic Resonance, Ltd., Shenzhen, China) using a 13-channel body coil in combination with a spine coil. The MRI protocols included T2-weighted half-Fourier acquisition single-shot turbo spin-echo (T2-HASTE), T2-weighted true fast imaging with steady-state precession (T2-TrueFISP), diffusion-weighted imaging (DWI), and T1WI with and without fat saturation (FS). The protocol parameters are listed in Table 1.
The MRI features considered indicative of HAE-I included the following: lesion hypervascularity, uneven signals, and oversized lesion, whereas those for HAE-II were the opposite. Two experienced radiologists independently evaluated the MRI features of all the cases.
The intraclass correlation coefficient (ICC) was used to assess interobserver variability. Fisher’s two-sided exact test was performed to compare the difference in MRI features between the two types of HAE. The sensitivity and specificity of each MRI feature of HAE-I were calculated. The prognoses of HAE-I and HAE-II were compared using the Kaplan-Meier log-rank test. SPSS 22.0 (IBM Corp., Armonk/NY, USA) was used to perform the statistical analysis. A P-value < 0.05 was considered statistically significant.
Results
All the cases were divided into two groups, HAE-I and HAE-II, based on the MRI features. Ultimately, sixteen cases with HAE-I and seven with HAE-II were recruited.
In the 16 HAE-I cases, the features of lesion hypervascularity, uneven signals, and oversized lesions were seen in 16, 16, and 15 cases (radiologist 1), and 16, 16, and 16 cases (radiologist 2). In the 7 HAE-I cases, the features were 0, 0, and 0 cases (radiologist 1), and 0, 0, and 0 cases (radiologist 2). Interobserver agreements between the two radiologists were consistent (all ICC > 0.75). Significant differences were found in the three MRI features between HAE-I and HAE-II. The sensitivity of the three MRI signs (lesion blood supply, signal, and size) in the diagnosis of HAE-I was as follows: 100% (16/16), 100% (16/16), and 93.7% (15/16), and the specificity was 100% (7/7), 100% (7/7), and 85.7% (6/7), respectively.
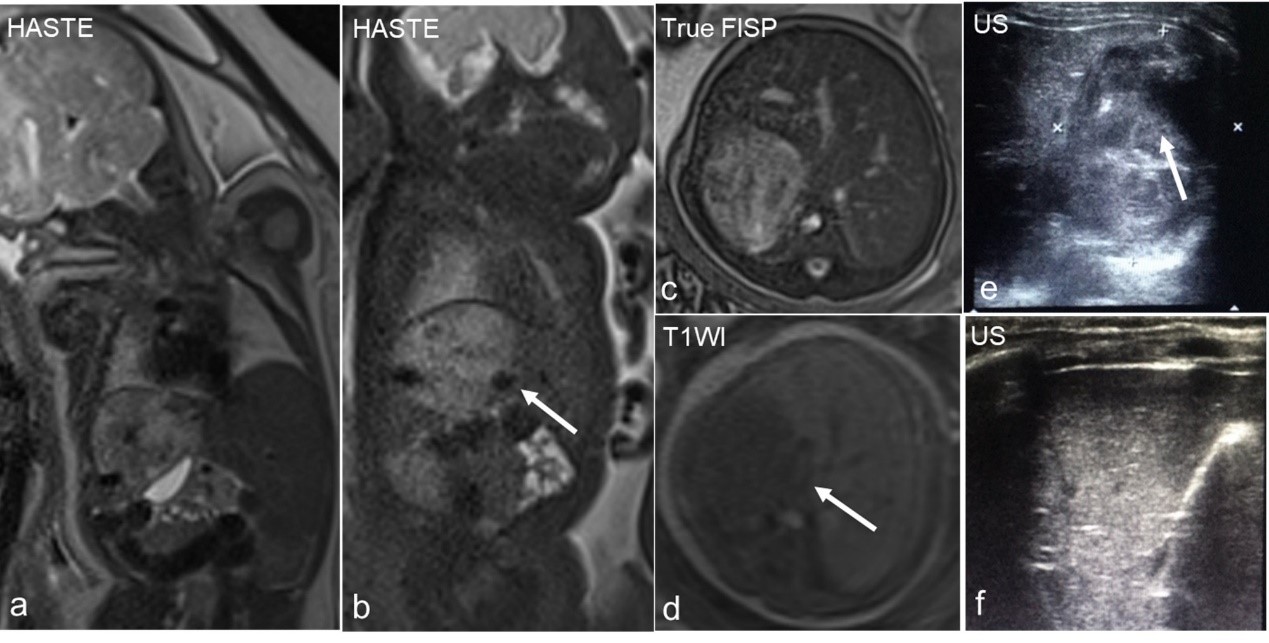
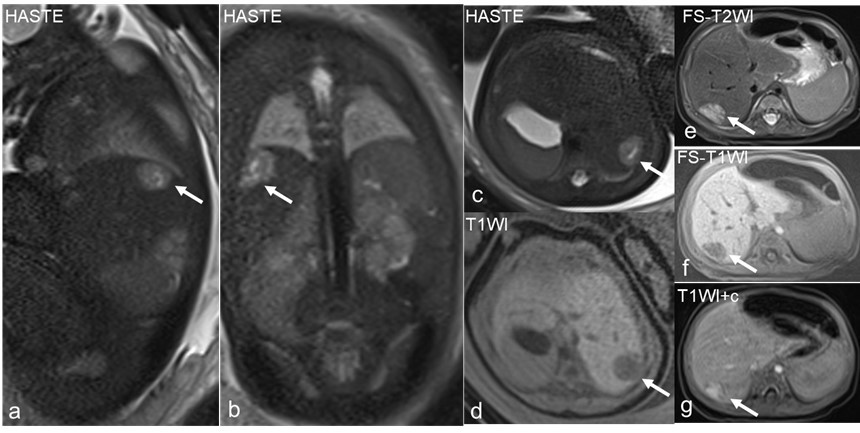
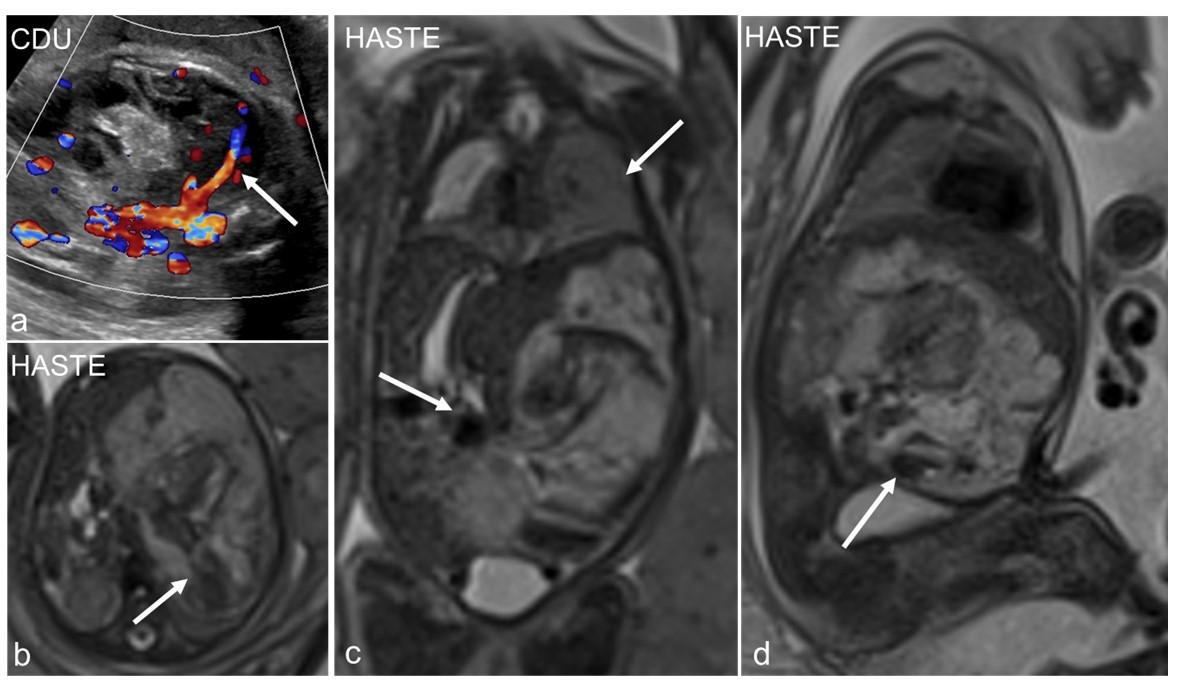
Changes in the size of the lesions were as follows: of the 16 cases in the HAE-I group, 9 (56.2%) became smaller (Fig. 1), 5 (31.2%) disappeared (Fig. 2), and 2 (12.5%) showed no apparent changes. Of the 7 cases in the HAE-II group, 3 (42.9%) became smaller (Fig. 3), 3 (42.9%) disappeared, and 1 (14.3%) showed no apparent changes.
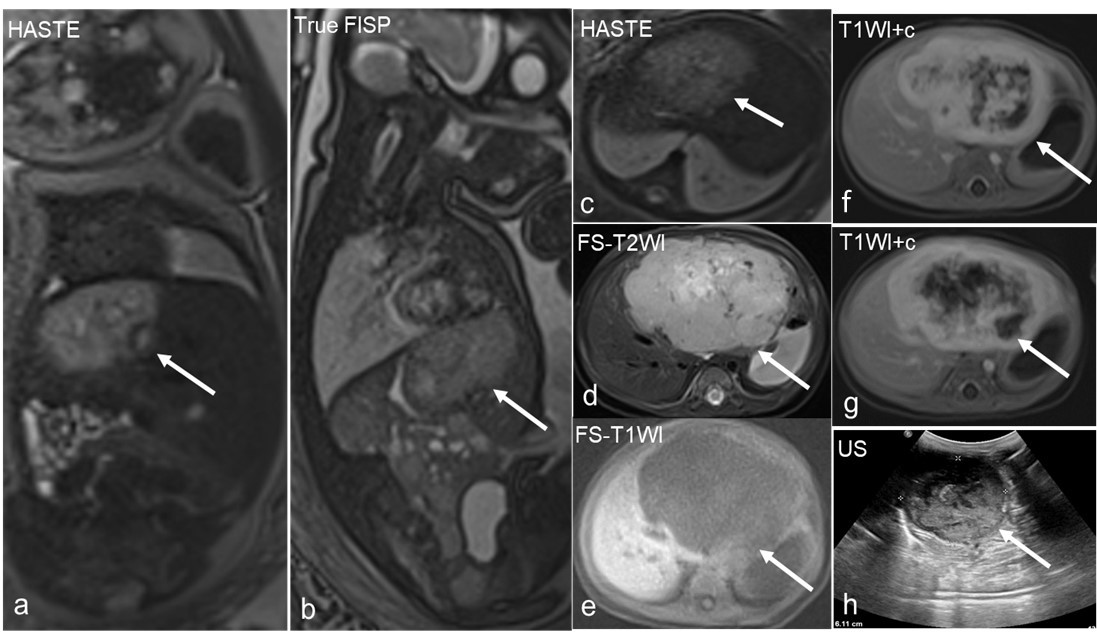
Regarding the prognosis, in the HAE-I group, 2 cases associated with severe complications died after birth (Fig. 4), 2 cases had a relatively poor prognosis, and 12 other cases had no apparent complications and all had a good prognosis. In the HAE-II group, none of the cases had any complications, and all had a good prognosis. There were no significant differences in the size changes (P>0.05) ,but significant differences in the prognosis (P <0.05) between HAE-I and HAE-II.
Discussion and Conclusion
Lesion hypervascularity, uneven signals, and oversized lesions are useful MRI features for differentiating HAE-I from HAE-II. The prognosis of fetal HAE-I is correlated with the vascular distribution, lesion size, and the signal. The more blood vessels, the larger the focus; the more heterogeneous the signal, the more prone to complications, and once complications occur, the prognosis is poor. If there are no complications, the prognosis is good. However, fetal HAE-II usually become smaller or disappears and has a benign presentation at birth.Acknowledgements
No acknowledgement found.References
[1] Alamo L, Beck-Popovic M, Gudinchet F, et al. Congenital tumors: imaging when life just begins[J]. Insights into Imaging,2011,2(3):297-308.
[2] von Schweinitz D. Neonatal liver tumours[J]. Seminars in Neonatology,2003,8(5):403-410.
[3] Isaacs H. Fetal and neonatal hepatic tumors[J]. Journal of Pediatric Surgery,2007,42(11):1797-1803.
[4] Franchi-Abella S, Gorincour G, Avni F, et al. Hepatic haemangioma—prenatal imaging findings, complications and perinatal outcome in a case series[J]. Pediatric Radiology,2012,42(3):298-307.
Figures