4062
Model-Driven Registration for 3D Placental Diffusion-Weighted MRI1School of Biomedical Engineering & Imaging Sciences, King's College London, London, United Kingdom, 2Department of Medical Physics & Biomedical Engineering, University College London, University College London, London, United Kingdom, 3Institute for Women’s Health, University College London, London, United Kingdom, 4Medical Physics, University College London Hospital, London, United Kingdom, 5Centre for Medical Imaging, University College London, London, United Kingdom, 6University Hospital KU Leuven, Leuven, Belgium, 7NIHR University College London Hospitals Biomedical Research Centre, London, United Kingdom
Synopsis
The placenta is essential for successful pregnancy outcome. Placental imaging is however challenging due to maternal breathing motion and fetal movements, making motion correction important for subsequent analysis. This study introduces an iterative model-based registration technique which incorporates a joint placenta-specific signal model for diffusion and relaxation data into the motion correction process. We compared our method to a pre-existing method used for contrast-enhanced data making use of principal component analysis. Our results suggest that the proposed method significantly improves alignment of free-breathing placenta relaxation and DW-MRI data and evidence that the precision of markers of function obtained in placenta can be improved.
INTRODUCTION
The placenta is essential for successful pregnancy outcome1. Inadequate placenta development leads to poor placental perfusion and placental insufficiency which can lead to long-term health consequences. MRI can be used to measure the whole placenta in vivo and provide detail about function and the effect of novel therapeutics. Placental imaging can be compromised by maternal breathing motion and fetal movements, making motion correction important for subsequent analysis. Advanced imaging such as relaxometry or diffusion-weighted imaging2,3 is more susceptible to motion due to long scan times and is made even more challenging by the use of variable image contrast.
In this study we propose a novel model-driven registration (MDR) method which incorporates a joint placenta-specific signal model for diffusion and relaxation data (DECIDE)3 into the motion correction process. We compare this technique to a pre-existing method used for contrast-enhanced data making use of principal component analysis (PCA) named progressive principal component registration4 (PPCR).
METHODS
Subjects
The study involved a cohort of eleven normal pregnant subjects with no known placental complications with gestational age between 24-34 weeks. The study was approved by the local research ethics committee and all subjects gave written informed consent.
Image Acquisition
MRI was performed under free-breathing on 1.5T Siemens Avanto, at seven b-values (0,50,100,150,200,400,600s.mm-2) and eight echo times (TE) (81,96,120,180,210,240,270,300ms). All TE were acquired at b-value=0s.mm-2 to allow T2 fitting and all b-values at TE=96ms. Other settings were as follows: TR=3900ms, FOV=402x479x437mm3, reconstructed matrix 156x192x26, temporal resolution 4.1s. The scan time was approximately 20 minutes. The placenta were manually segmented (ITK-SNAP Version 3.6.0,2017) from the unregistered baseline image (lowest TE, no diffusion weighting).
Image Registration
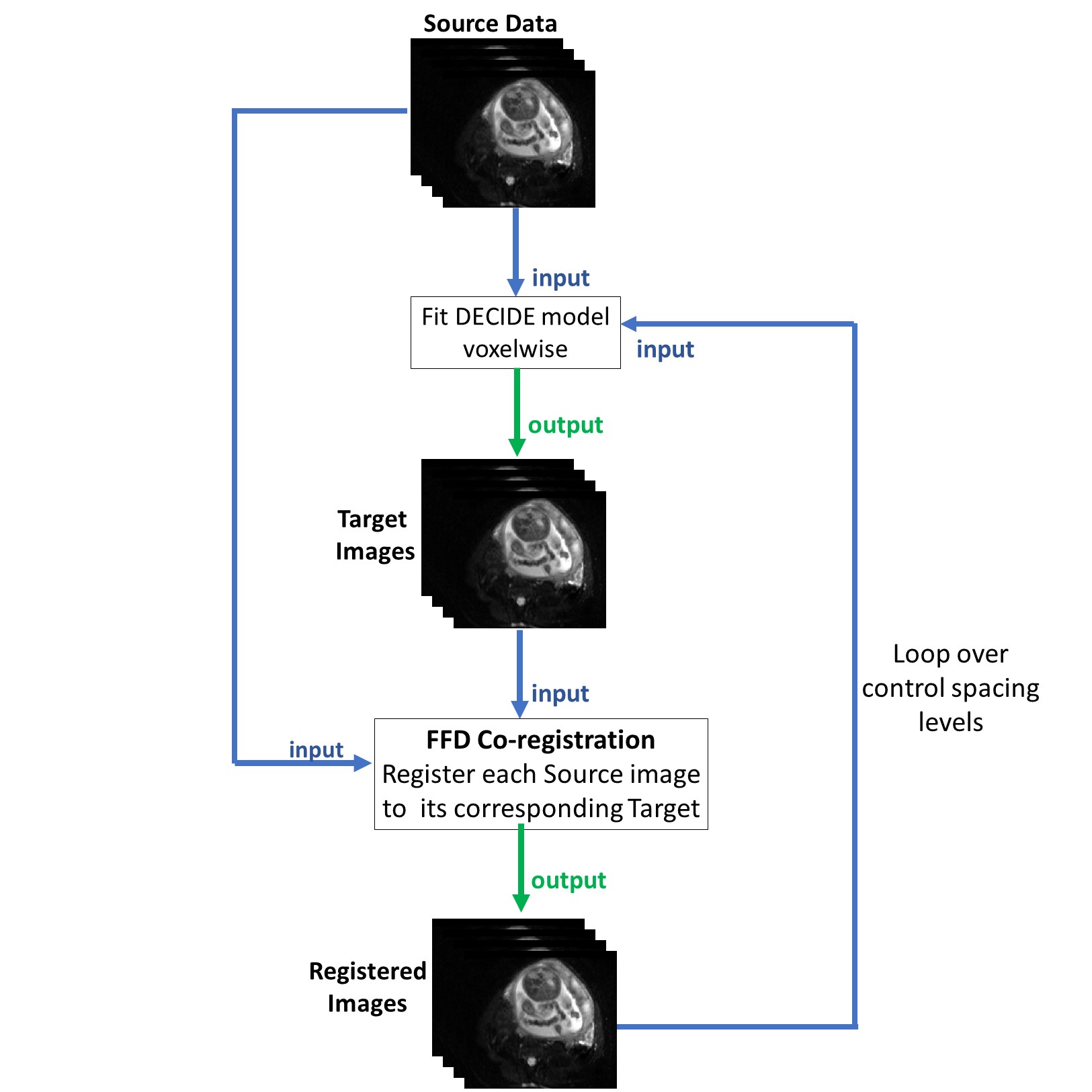
The core architecture of the MDR algorithm is as follows (Fig.1): the DECIDE model3 is fitted voxelwise to the source 3D data using a fast linear fit5 (non-linear fitting is slow and therefore impractical for voxel-based parameter estimation) and the model fit results are used as target images for registration; then a highly optimised C++ implementation6 of free-form deformation (FFD) registration was used to register each source to its corresponding target image.The model-fitting and registration steps are alternated three times with decreasing FFD control spacing (10x10x10, 5x5x5, 2.5x2.5x2.5 pixels). We compare our results to a previously published algorithm which replaces the model-fitting step with results from three-iterations of PCA analysis (this algorithm incorporates the same baseline free-form registration algorithm4). Image registration was performed on a standard laptop computer (3.1GHz,16GB).
Evaluation
After registration, the DECIDE model was fitted non-linearly using an in-house software developed in MATLAB (The MathWorks Inc,Natick,MA).The results were evaluated by visual comparison of registered and unregistered images and by computing the root mean square error (RMSE) between the data and the fit of each method.
RESULTS
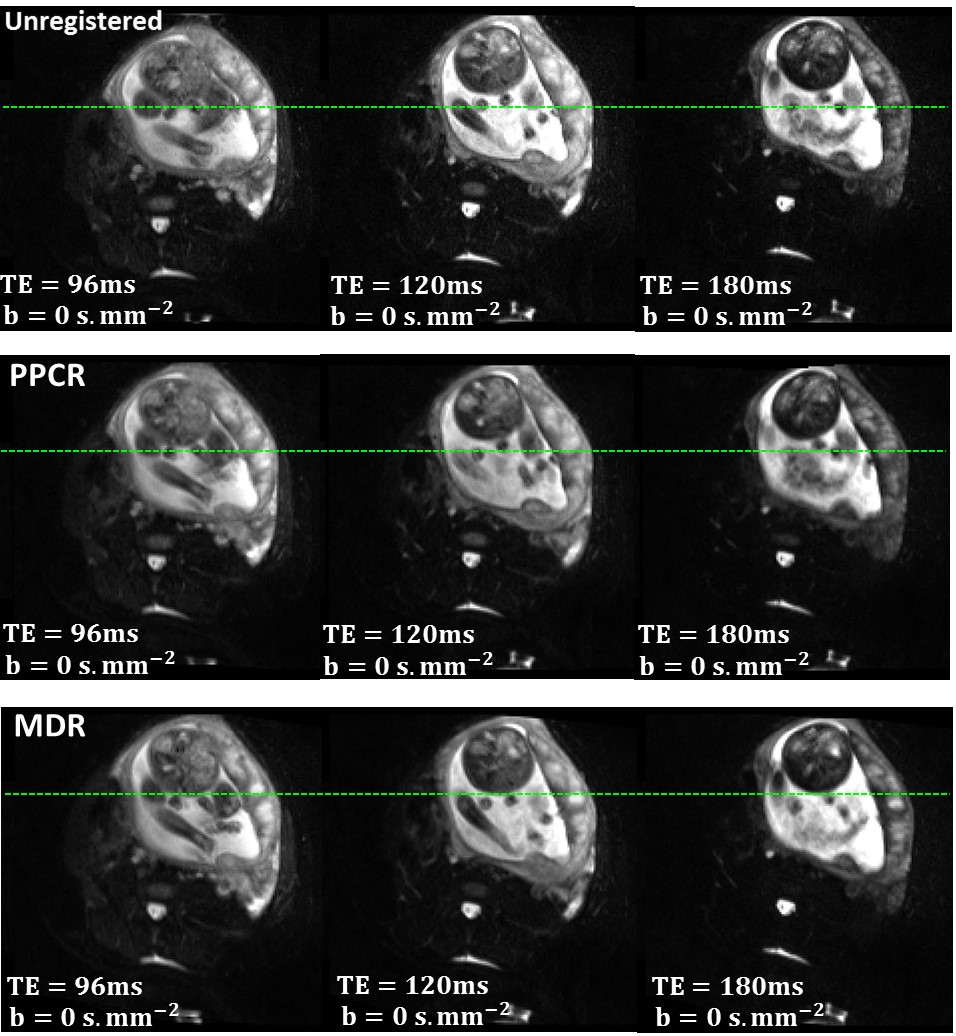
The MDR algorithm notably removes the motion without affecting signal intensities (Fig.2).
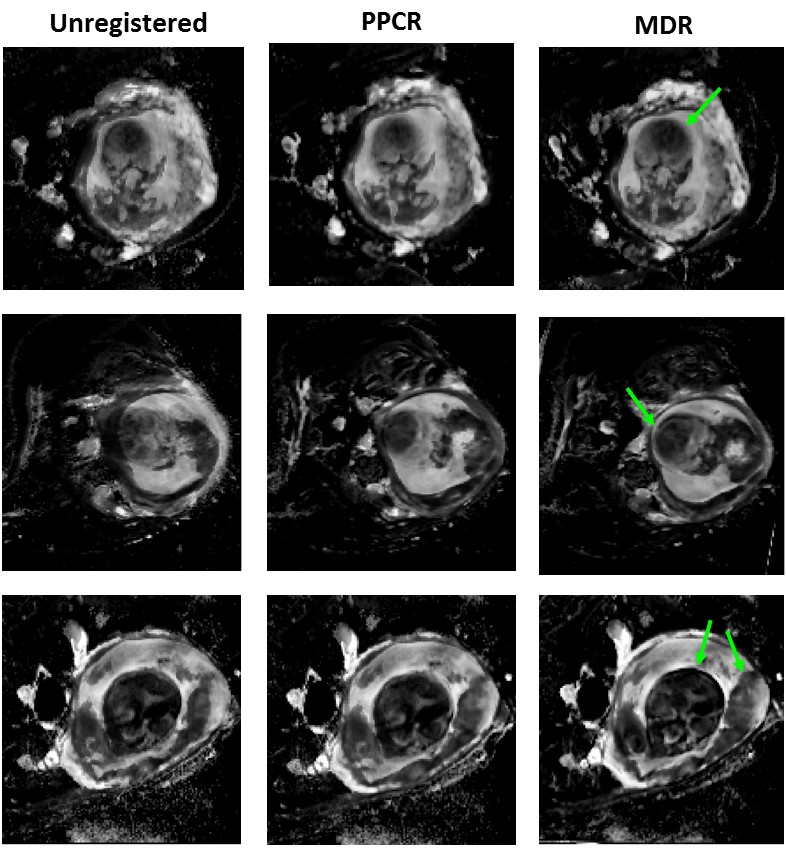
The unregistered fetal blood volume fraction maps show strong blurring and artefacts which are mostly removed after MDR leading to much clearer organ boundaries (Fig.3).
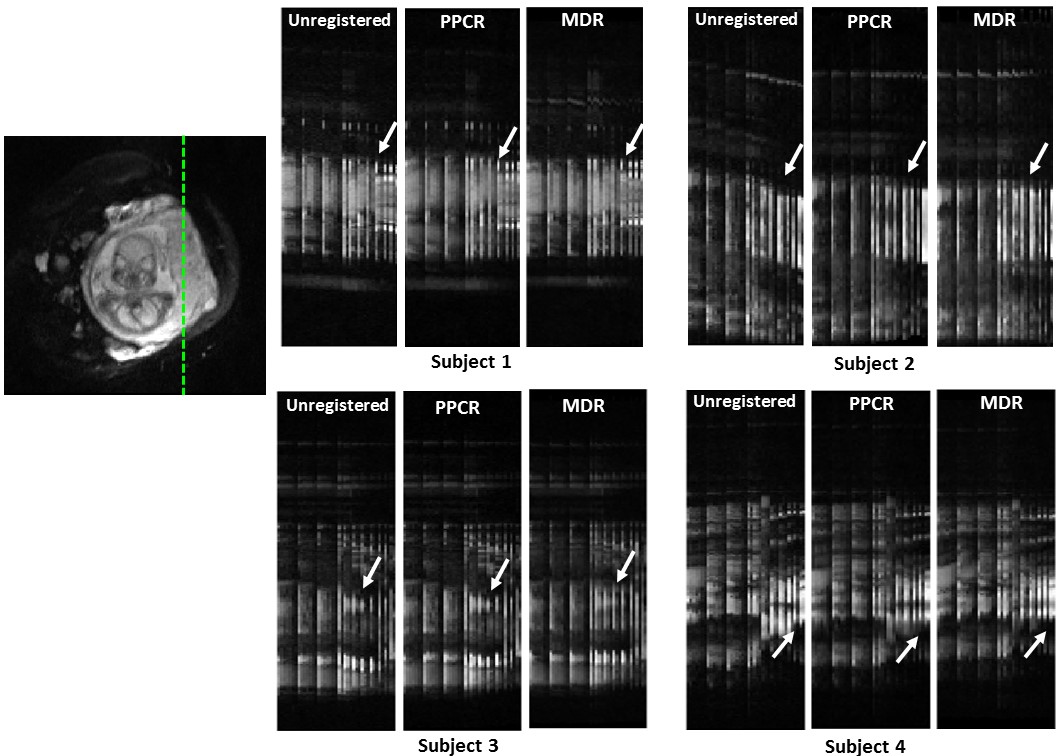
Time-cut images of the unregistered and registered data demonstrate that misalignments were further reduced after MDR in all cases (Fig.4).
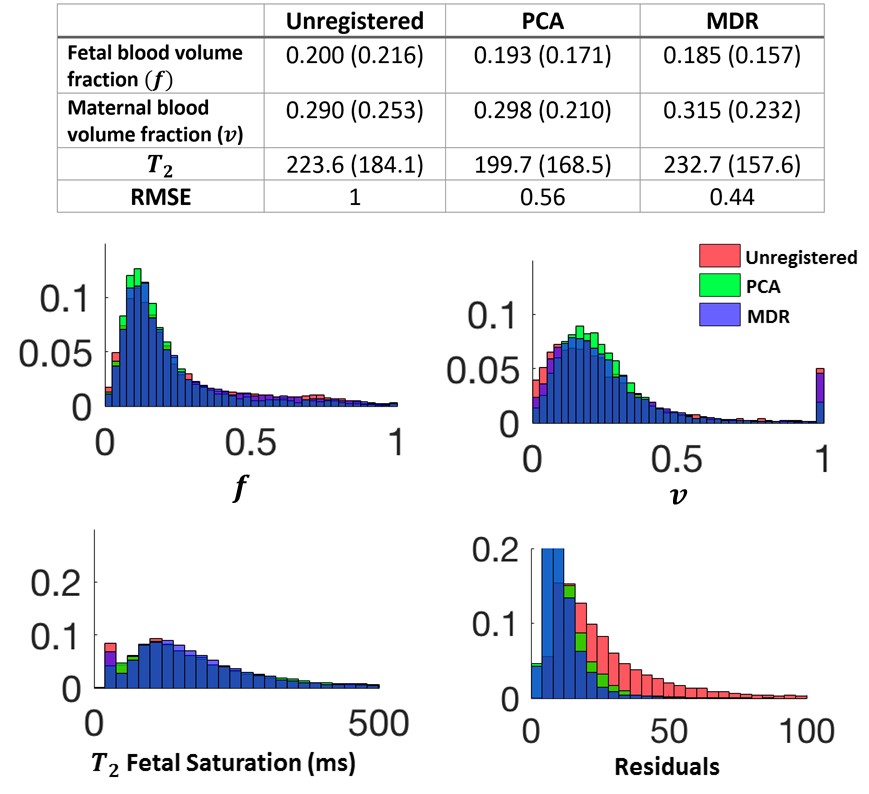
The registered and unregistered histograms in Fig.5 show similar distributions for all parameters. Analysis showed a further decrease of the residual error with the MDR method (0.44) compared to PPCR (0.56).
Regarding calculation times the MDR method took 12-15 minutes.
DISCUSSION
An iterative model-based registration method has been proposed. We compared the performance of MDR to PPCR by keeping the control point spacing and transformation model the same for both methods. However, the methods use different approaches to create target images. Results show that MDR method allows improved motion correction compared to PPCR. This is also demonstrated by the further reduction of the residual bias between the data and the fit.
Although a placenta model is used (DECIDE), the method is essentially tissue independent and it is therefore applicable to other organs. Results show very good alignment of structures outside of the placenta, including the fetal brain. Further work will explore how our method can be used to improve the alignment of these structures and if useful information can be obtained.
CONCLUSION
MDR with a placenta-specific tissue model provides accurate registration of free-breathing placenta relaxation and DW-MRI data and strong evidence that the precision of the parameters we are attempting to measure can be improved. Non-rigid registration of the placenta has a vital role in improving the precision of markers of function obtained in the placenta; this information is crucial to help predict both if and when the placenta may fail; and will help the assessment of novel treatments for placenta dysfunction.Acknowledgements
This work is supported by the Wellcome Trust grants 210182/Z/18/Z and 101957/Z/13/Z, the EPSRC NS/A000027/1 and the Radiological Research Trust. We would like to thank all the families who agreed to take part in this research.References
- Spencer RN, Carr DJ and David AL. Treatment of poor placentation and the prevention of associated adverse outcomes – what does the future hold?. 2014. Prenat Diagn, 34: 677-684.
- Slator PJ, Hutter J , McCabe L, et al. Placenta microstructure and microcirculation imaging with diffusion MRI. Magn Reson Med. 2018; 80: 756–766.
- Melbourne A, Aughwane R, Sokolska M, et al. Separating fetal and maternal placenta circulations using multiparametric MRI. Magn Reson Med. 2018;00:1–12.
- Melbourne A, Atkinson D, White MJ, Collins D, Leach M, Hawkes D. Registration of dynamic contrast‐enhanced MRI using a progressive principal component registration (PPCR). Phys Med Biol. 2007;52:5147–5156.
- Flouri D, Lesnic D and Sourbron SP. Fitting the two‐compartment model in DCE‐MRI by linear inversion. Magn Reson Med. 2018; 76: 998–1006.
- Modat M, Ridgway G, Taylor Z, et al. Fast free‐form deformation using graphics processing units. Comput Methods Programs Biomed. 2010;98:278–284.
Figures