4059
Joint placental angiography with perfusion and apparent oxygenation mapping1Biomedical Engineering,School of Biomedical Engineering & Imaging Sciences, Kings College London, London, United Kingdom, 2Department of Women and Children’s Health, School of Life Course Sciences, Kings College London, London, United Kingdom, 3Centre for the Developing Brain, School of Biomedical Engineering & Imaging Sciences, Kings College London, London, United Kingdom
Synopsis
In this work we combine two novel methods for imaging the oxygen transfer system between maternal and fetal circulations, 1) a motion robust angiography acquisition and 2) a combined perfusion and oxygenation acquisition. This enables the matching of functional regions of placenta to the vessels that supply them in utero. This may provide further insight into the vascular origins of major obstetric diseases such as fetal growth restriction and pre-eclampsia.
Introduction
The effective exchange of oxygen between maternal and fetal circulations in the placenta is an essential component to fetal health.1,2 Defective trophoblast invasion and incomplete remodelling of the maternal vasculature leads to ineffective perfusion and placental oxidative stress. A subsequent cascade of events can lead to severe obstetric complications such as fetal growth restriction (FGR) and pre-eclampsia (PE).3,4
Placental T2* has become a key MRI biomarker for identifying placental deficiency with MRI.5,6 This originates from the BOLD contrast mechanism, in which the paramagnetic effect of deoxyhaemoglobin shortens the T2* relaxation of tissue. The hypothesis is that a shortened T2* indicates a relative excess of deoxygenated blood and possible dysfunction in placental oxygen exchange. However, T2* is insufficient to completely describe the complex haemodynamics of the placenta and is unable to further indicate the cause of dysfunction.
In this study we combine two novel methodologies we have separately developed for investigating the circulation in the placenta, 1) a motion-robust angiography sequence for vessel visualisation and 2) an interleaved perfusion/oxygenation sequence (PERFOX). The methods behind both of these techniques are described in detail in separate abstracts submitted to this conference. Here, we describe how the images produced by these methods can be combined to further explore placental circulation.
Methods
Imaging was performed on a Philips 3T Achieva system equipped with a 32-channel cardiac coil. Informed consent was obtained from 5 pregnant participants (gestational age (GA): 22-38w). Scanning was performed in the supine position with routine blood pressure and pulse oximetry monitoring. No sedation, gating or exogenous contrast methods were used.
Angiography was performed with a 2D snapshot RF-spoiled gradient echo acquisition modified for the ‘sweep’ method, where the imaging slice is moved continuously by shifting excitation frequency of each successive RF pulse.7 This produces dense spatiotemporal sampling that confers motion robustness. A retrospective motion correction model was applied, based on partitioning data into respiration states before recombination to a single motion free image.8
The PERFOX acquisition comprised of a velocity selective arterial spin labelling (VSASL) module preceding a multi-echo gradient echo EPI (MEGE-EPI) acquisition. The VSASL module labels maternal blood for imaging perfusion while the MEGE-EPI readout allows for interleaved T2* decay modelling.
Relevant acquisition parameters:
Sweep angiography scan: FOV=260x320x220mm; Resolution=1.2x1.2mm; slice thickness=3.5mm; TR/TE=10/5.4ms; flip=55⁰; SENSE=2; sweep shift/pulse=6.4µm; time/slice=580ms; Total acquisition time=5.33m.
PERFOX scan: FOV=260x320x32mm; resolution=4mm3, TR/TEs=3500/20-56-93ms, 25 label/control pairs, SENSE=2.5, Vc=1.55cm/s, PLD=1600ms, Total acquisition time=2.30m.
Results
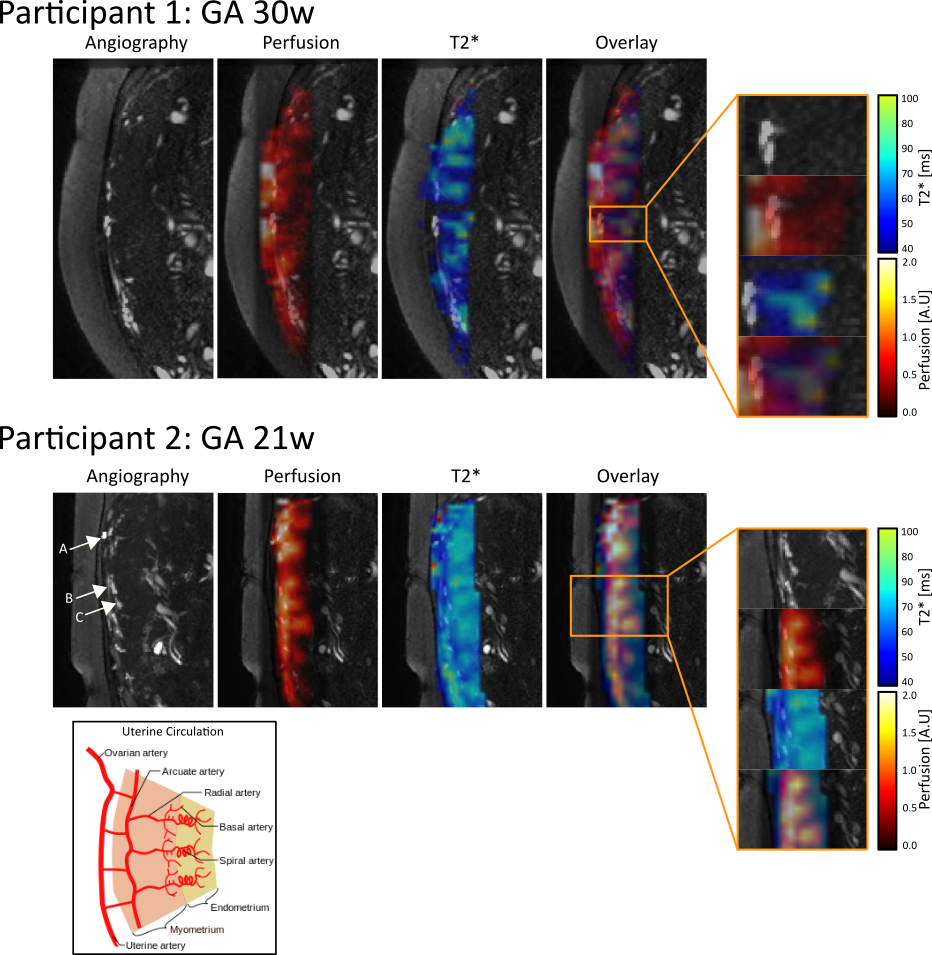
Figure 1 shows two coronal image stacks of angiography data with T2* and perfusion maps overlaid. The regions of high perfusion can be seen to match closely to the regions in which large blood vessels are present. Regions of high perfusion also propagate away from the visible vessels, these likely correspond to the location of spiral arteries in the endometrium that are too small to be visualised directly by the angiography but are the downstream outlets of the uterine vessels. The perfusion values drop towards the centre of the placenta as the tagged maternal blood is restricted by the fetal villi. In these regions, T2* of tissue remains high indicating that the oxygen has transferred to untagged fetal blood.
Two representative participants are shown in Figure 2. The uterine vascular system is complex, with a hierarchical network of vessels supplying blood to the functional cotyledons (see figure 2 inset). In participant 2 we can identify three levels of this network up to the radial arteries. The terminations of these vessels match closely with areas of high perfusion and T2*.
Discussion
In this study we have combined two new acquisitions that provide complementary information to investigate the flow of oxygen through the placenta. This provides the ability to identify regions with high exchange activity and identify the vessel that supplies this region. This may help diagnose and potentially link vascular remodelling defects linked to decreased oxygen transfer.
In its current form, the angiography acquisition is able to identify the major vessels present in the myometrium. Further clinical value may be provided by increasing the effective spatial resolution of these images such that spiral arteries in the endometrium can be visualised to provide a complete vascular map of the placental circulation. However, the presence of high perfusion in areas downstream from visible vessels demonstrates indirect detection of the terminal vessels.
Conclusion
This technique enables the pathways to be traced from the maternal circulation to the placental units where it exchanges with the fetal circulation. This has potential to provide a detailed view of how oxygen is transported through the placenta to the fetus and may give valuable insights into where and how this transfer is compromised in diseases such as FGR and PE.Acknowledgements
This work was supported by the NIH Human Placenta Project grant 1U01HD087202-01 (Placenta Imaging Project (PIP)), the Wellcome Trust (Sir Henry Wellcome Fellowship, 201374/Z/16/Z), and the EPSRC (grants N018702 and M020533) and by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.References
1. Pardi, G., Marconi, A. M. & Cetin, I. Placental-fetal interrelationship in IUGR fetuses - A review. Placenta 23, 136–141 (2002).
2. Kingdom, J. C. P. & Kaufmann, P. Oxygen and placental villous development: Origins of fetal hypoxia. Placenta 18, 613–621 (1997).
3. Sibai, B., Gus, D. & Michael, K. Pre-eclampsia. Lancet (London, England) 365, 785–99 (2005).
4. Baschat, A. A. & Hecher, K. Fetal Growth Restriction due to Placental Disease. Semin. Perinatol. 28, 67–80 (2004).
5. Hutter, J. et al. Multi-modal functional MRI to explore placental function over gestation. Magn. Reson. Med. 1–14 (2018). doi:10.1002/mrm.27447
6. Sørensen, A. et al. Changes in human fetal oxygenation during maternal hyperoxia as estimated by BOLD MRI. Prenat. Diagn. 33, 141–145 (2013).
7. Jackson, L. H. et al. Respiration resolved imaging using continuous steady state multiband excitation with linear frequency sweeps. Proc. ISMRM18 Paris (2018).
8. Schnabel, J. A. et al. A generic framework for non-rigid registration based on non-uniform multi-level free-form deformations. in Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics) (2001). doi:10.1007/3-540-45468-3_69
Figures