4057
The reduction of perfusion fraction in placenta increta --a pilot study of placental perfusion using IVIM MRI1Department of Radiology, the first Affiliated Hospital of Xi'an Jiaotong University, Xi'an, China, 2MR Research China, GE Healthcare, People’s Republic of China, Bei Jing, China
Synopsis
Placenta increta, a serious threat to maternal and fetal life, is difficult to distinguish by traditional MRI. In this study, IVIM imaging was used for the first time to detect the perfusion level of some placenta implanted, and it was found that the perfusion fraction was significantly lower than that of the normal placenta. That is help for establishing a new method for clinical diagnosis of placental implantation, especially placenta non-percreta.
Introduction
Placenta increta, which means placenta can't be separated from the uterus during labor, can cause a large amount of bleeding of mother1. Therefore, it is a serious threat to maternal and fetal life. Although the diagnosis of placenta implantation by MRI is more accurate than ultrasound, it is difficult to distinguish the boundary between the placenta and the myometrium due to the thinness of the lower uterus muscle layer in the third trimester of pregnancy. So it is very important to find a more effective method for helping diagnosing placenta increta. Our study found that IVIM MRI can distinguish implantable placenta from normal placenta. This will provide a new and effective method for diagnosing placenta increta.Materials and Methods
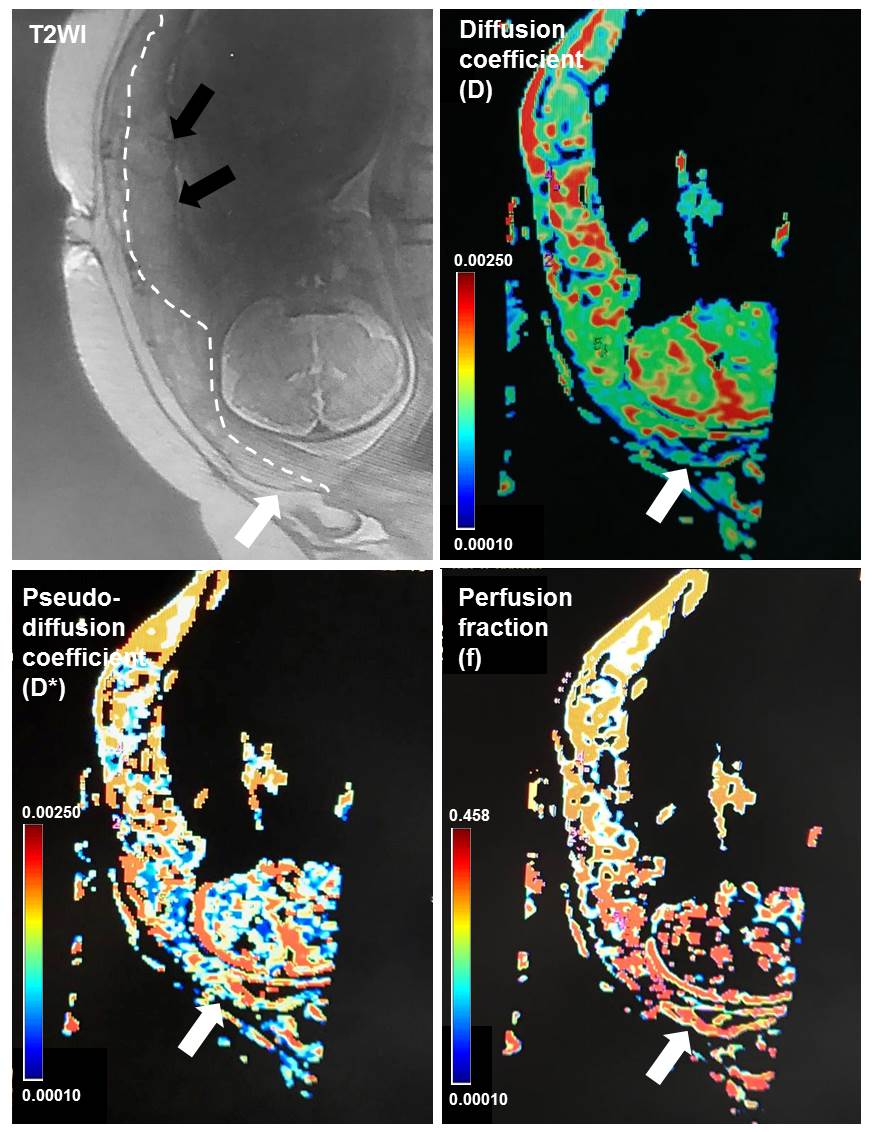
This study was approved by ethical committee of First Affiliated Hospital of Xi’an Jiaotong University. Written parental informed consent was obtained for all pregnant women. 15 pregnant women were recruited from January 2016 to March 2017 in First Affiliated Hospital of Xi’an Jiaotong University. No sedatives were used for MRI. The scanning was stopped immediately once the pregnant woman has chest discomfort or other discomfort. Placental MR examination for each gestational woman was performed on a 3T MRI system (GE Healthcare, Milwaukee, Wisconsin) with an 8-channel body flex coil. Single shot fast spin echo (SSFE) T2-weighted images were acquired using: TR minimum; TE 85 ms, matrix 228×256, FOV 36mm, section-thickness 4 mm without gap. Intra Voxel Incoherent Motion (IVIM) images were collected with each of the following b values: 0, 20, 50, 80, 100, 150, 200, 400, 600, 800sec/mm2. The scanning parameters were as follows: TR 2000ms; TE 63 ms, matrix 128×128, FOV 38mm, section-thickness 4mm with 1mm gap. A total examination time was less than 10 min. Regions of interest (ROI) were drawn under the direction of an experienced obstetrician (Figure1) and references2. For each placenta, 3 ROI of fetal compartment and 3 ROI of maternal compartment were drawn. Part of implantation placenta also drew ROI, and ROI of the corresponding position of the normal placenta as a control. Post-processing of IVIM images to obtain the diffusion coefficient (D), pseudo-diffusion coefficient (D*) and perfusion fraction (f) value of the ROIs.Results
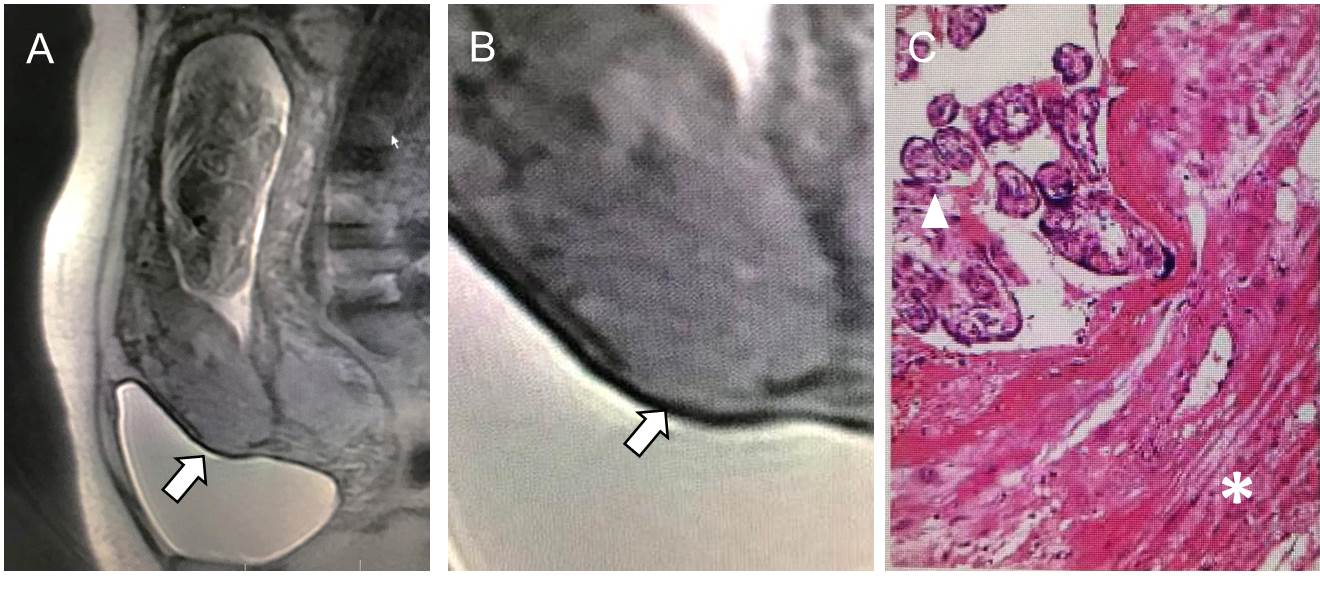
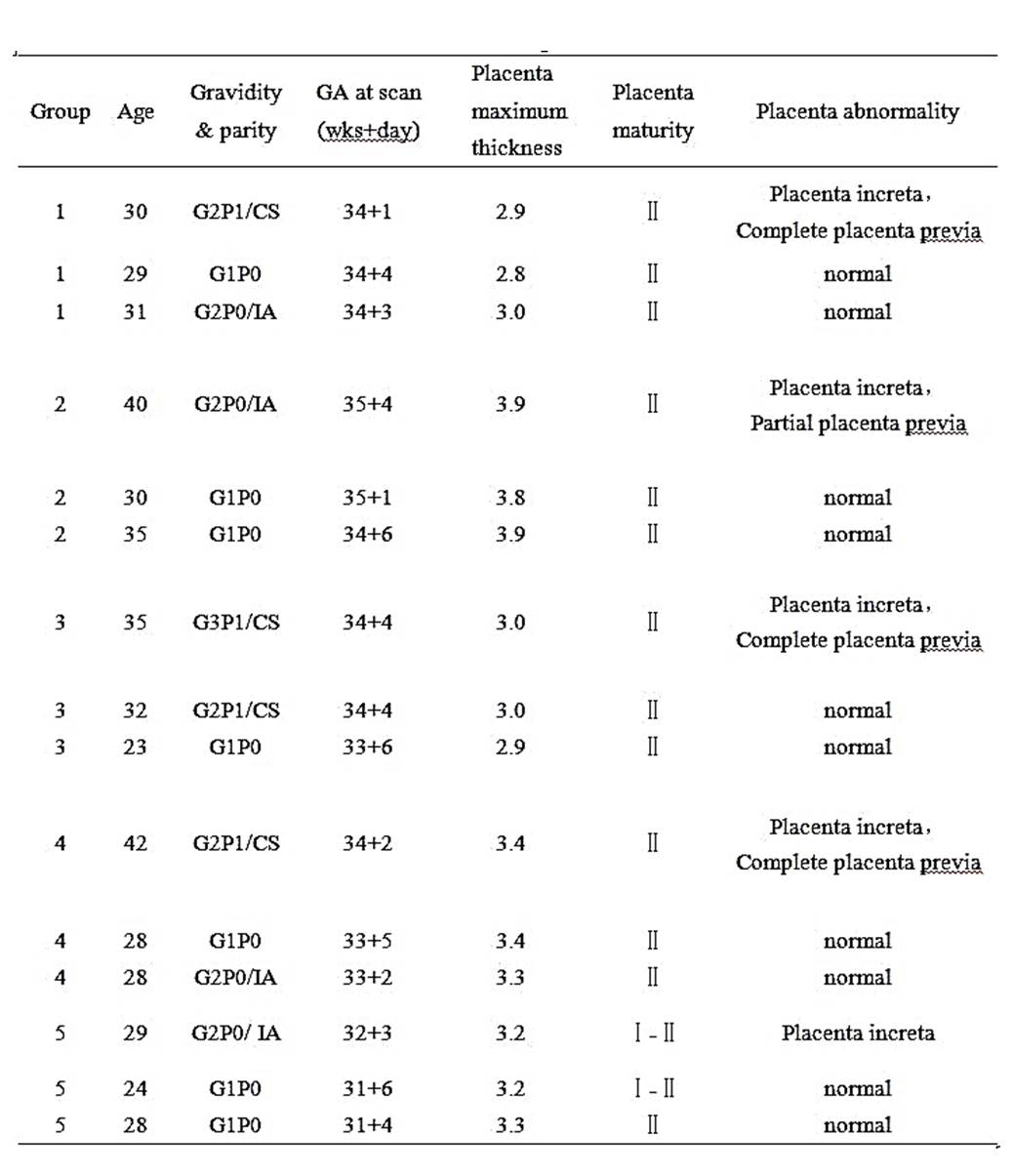
A total of 15 pregnant women were recruited for this research. Five of them were patients who diagnosed placenta increta surgically or pathologically. Figure 2 showed MRI and the pathological image. Each patient was matched two pregnant women with normal placenta as a group (Table1).
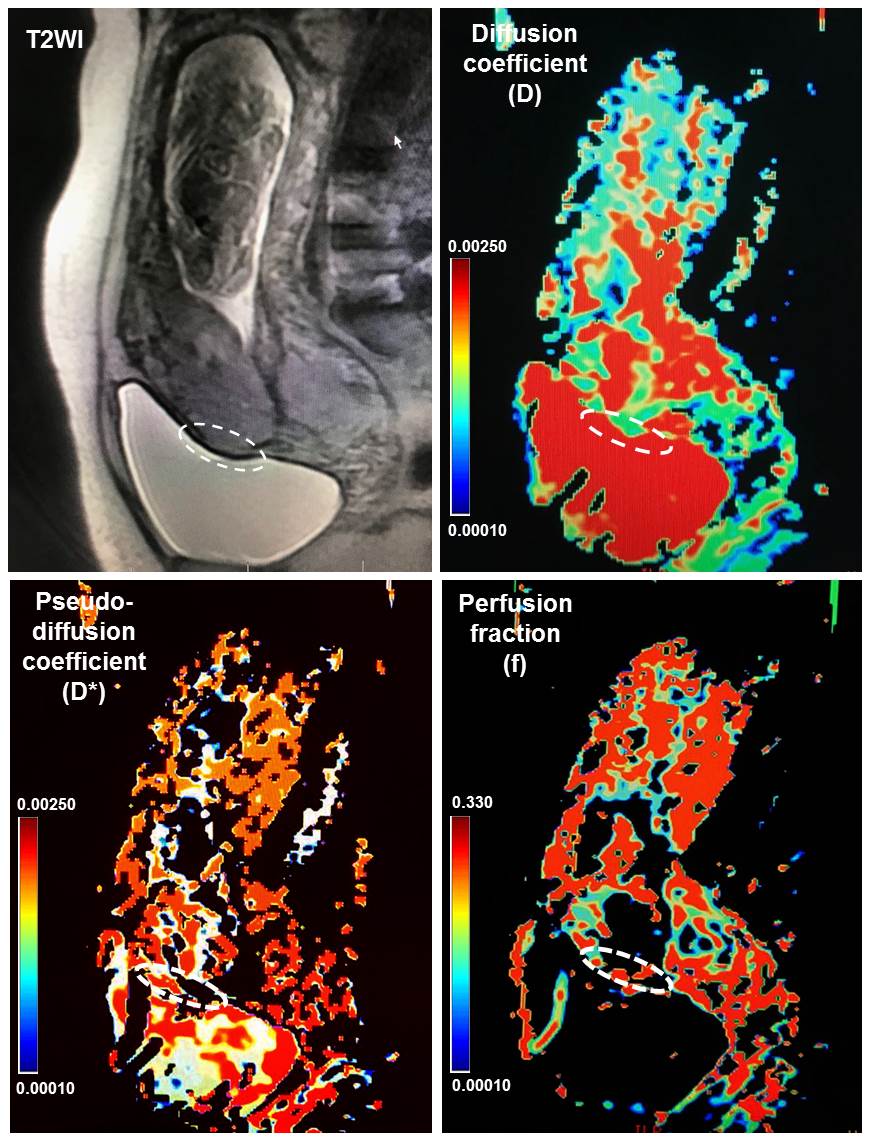
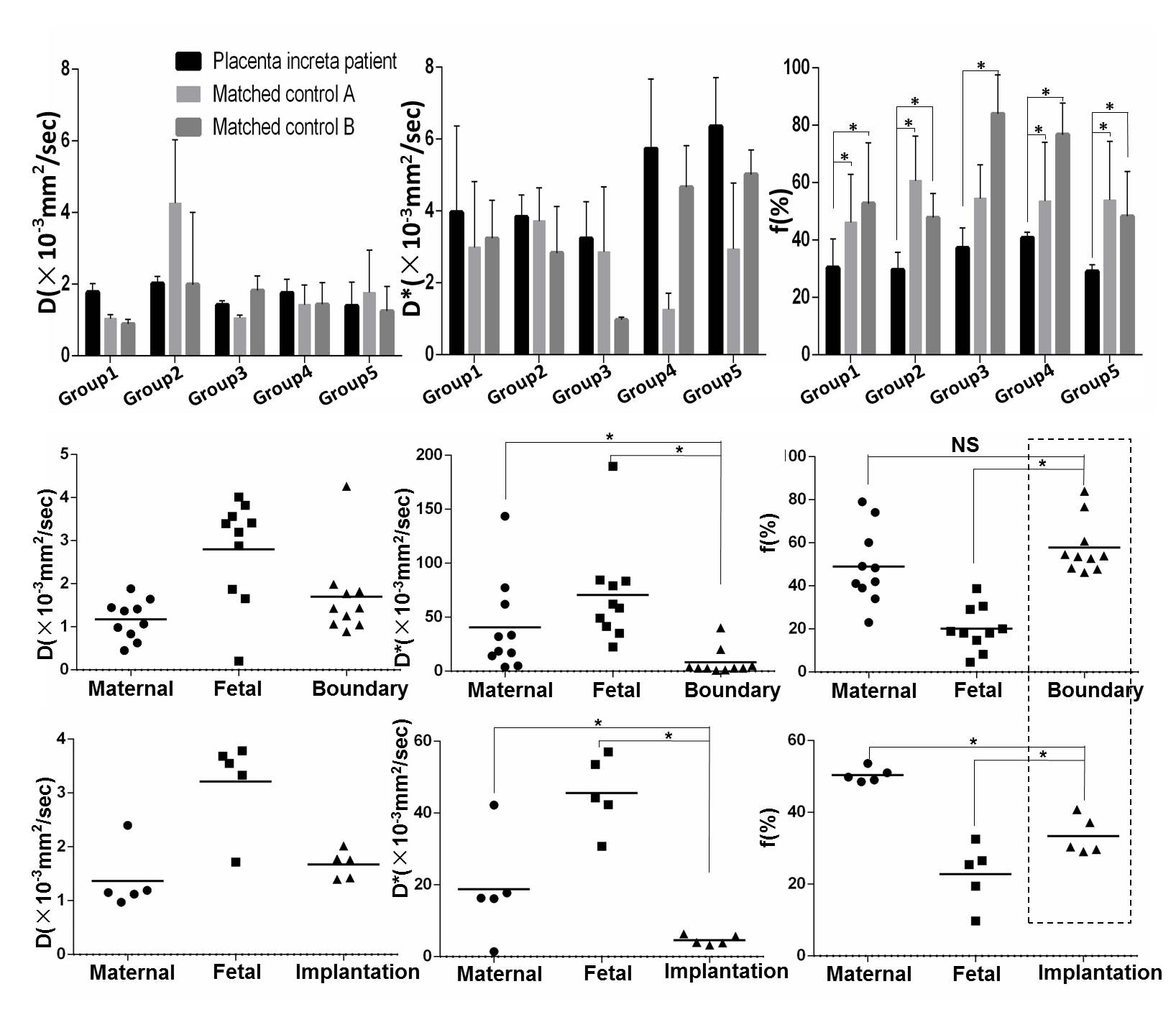
IVIM post-processing images, including D, D*, f maps, and T2WI for normal placenta and implantable placenta were shown in Figure 2 and 3. Figure 4 demonstrated that the perfusion fraction of the implanted partial placenta in each group is significantly reduced compared to the corresponding anatomical position of the normal placenta.
Through
the division of the fetal part and the maternal part of the placenta, we found
that the perfusion fraction of the maternal part of the placenta was
significantly higher than that of the fetal part (Figure 4). It is noteworthy that
the perfusion fraction of the part of the implantable placenta was between those
two parts. While the perfusion fraction at the edge of the normal placenta (the
portion corresponding to the anatomical location of the implant) is then at the
same level as the maternal portion of the placenta.
Discussion
The IVIM model has proven to be an ideal model for evaluating placental blood perfusion3,4. Through this model, we found that the maternal partial perfusion fraction of the placenta was higher than that of the fetal part, which is consistent with other studies5. This is most likely due to the fact that the blood volume of maternal part in placenta is more abundant than that in fetal side and transported to the fetal side. In normal pregnancy, the lateral margin of the placenta is the myometrium, and the blood volume of the myometrium is comparable to that of the mother's side placenta. So the perfusion fraction of boundary normal placenta is the same as the maternal side of the placenta. The implanted part of the placenta breaks the blood circulation of the normal placenta and myometrial attachment6, so the bleeding perfusion score is different from that of the normal placenta. This is the first report on the level of perfusion in implantable placental, which is likely to be used as a diagnosis for placental implantation. This can compensate for the defects of MRI plain image diagnosis.Conclusion
The perfusion fraction of implanted placenta is reduced compared to the normal placenta, which will help for diagnosis.Acknowledgements
This work was supported by the National Key Research and Development Program of China (2016YFC0100300), National Natural Science Foundation of China (No. 81471631, 81771810 and 51706178), the 2011 New Century Excellent Talent Support Plan of the Ministry of Education, China (NCET-11-0438) the Clinical Research Award of the First Affiliated Hospital of Xi’an Jiaotong University (No.XJTU1AF-CRF-2015-004), Research and Development Fund of the First Affiliated Hospital of Xi'an Jiaotong University (YK201509), Shaanxi Natural Science Basic Research Program Fund (2017JQ8034), Basic Research Fund of central Colleges (xjj2018jchz07).References
1. Kaufman C, Tadros A. Endovascular Interventions for the Morbidly Adherent Placenta. Journal of clinical medicine 2018; 7(5).
2. You W, Andescavage N, Zun Z, Limperopoulos C. Semi-automatic segmentation of the placenta into fetal and maternal compartments using intravoxel incoherent motion MRI. Proceedings of SPIE--the International Society for Optical Engineering 2017; 10137.
3. Slator PJ, Hutter J, McCabe L, et al. Placenta microstructure and microcirculation imaging with diffusion MRI. Magnetic resonance in medicine 2018; 80(2): 756-66.
4. Jakab A, Tuura RL, Kottke R, et al. Microvascular perfusion of the placenta, developing fetal liver, and lungs assessed with intravoxel incoherent motion imaging. Journal of magnetic resonance imaging : JMRI 2018; 48(1): 214-25.
5. Moore RJ, Strachan BK, Tyler DJ, et al. In utero perfusing fraction maps in normal and growth restricted pregnancy measured using IVIM echo-planar MRI. Placenta 2000; 21(7): 726-32.
6. Merz W, Van de Vondel P, Strunk H, Geipel A, Gembruch U. Diagnosis, treatment and application of color Doppler in conservative management of abnormally adherent placenta. Ultraschall in der Medizin 2009; 30(6): 571-6.
Figures