4055
Fetal cardiac 4D phase-contrast MRI using Doppler ultrasound gating to visualize fetal hemodynamics in utero: preliminary resultsFabian Kording1, Björn Schönnagel1, Christian Ruprecht1, Manuela Tavares de Sousa2, Jin Yamamura1, and Daniel Giese3
1University Medical Center Hamburg-Eppendorf, Hamburg, Germany, 2Department of Obstetrics and Fetal Medicine, Germany, University Medical Center Hamburg-Eppendorf, Hamburg, Germany, 3Department of Radiology, University Hospital Cologne, Cologne, Germany
Synopsis
In this study 2D and 4D phase contrast MRI angiography was performed in six foetuses (gestational week 30-35) with direct cardiac gating using Doppler ultrasound at 1.5T. The fetal vasculature and hemodynamics could be visualised in detail including the ductus arteriosus. Blood flow was similar between 2D and 4D PCA. This method may provide an important additional tool for prenatal diagnosis of CHD such as coartation of the aorta.
Introduction
Fetal CMR provides a valuable adjunct to fetal echocardiography in the evaluation of congenital cardiovascular pathologies (1). The use of 4D flow cardiovascular magnetic resonance (CMR) may provide valuable additional information over conventional Doppler methods for the assessment of fetal hemodynamics, especially for prenatal diagnosis of fetal coarctation that is still challenging today (2). As 4D flow CMR requires cardiac gating the application to the fetus was limited in the past. With the recent development of a gating device based on Doppler ultrasound similar to an ECG (3) standard sequences such as 4D flow requiring gating can also be applied. Hence, the aim of this preliminary study was to evaluate the feasibility of 4-dimensional phase contrast magnetic resonance imaging to visualize fetal cardiac hemodynamics with the focus on the fetal aorta. In addition the blood flow was quantitatively compared between standard 2D and 4D acquisitions.Methods
The feasibility to acquire a 4D dataset of the aortic arch and to visualize fetal cardiac hemodynamics was evaluated in six fetuses (Gestation week 30 - 35) at 1.5T (Philips, Archieva). Cardiac gating was performed using a recently developed MRI compatible Doppler Ultrasound (DUS) device (northh medical GmbH, Hamburg, Germany). The device records the fetal heart rate and processes the signal into a gating signal that is fed into the physiologic unit of the MRI, similar to ECG gating. The 4D phase contrast sequence (pixel spacing = 1.04 x 1.04 x 2.50 mm, slice thickness = 5 mm, TR/TE: 3.0/2 msec, FA: 6.5°, SENSE = 2, FoV = 300 x 300 x 50 mm, Phases= 10) was limited to only 10 heart phases to minimize imaging time, resulting in a temporal resolution of ca. 40 ms and scan time of 2.30min. Morphologic images of the aorta and fetal heart for planning and orientation were acquired using a retrospectively gated cine balanced steady-state free precession sequences (pixel spacing = 1.0 x 1.0 mm2, slice thickness = 5 mm, TR/TE: 5.0/1.6 msec, FA: 60°, SENSE = 2, matrix = 288 x 288, Phases= 20). Visualizations and analysis was performed using Gyro Tools. Flow values in the aorta descendent (AoD) were calculated from each 4D dataset and compared to a gated 2D cine phase contrast angiography sequence (pixel spacing = 1.2 x 1.2 mm2, TR/TE: 4.2/2.6 msec, FA: 10°, slice thickness: 8 mm, VENC: 160 cm/s, phases: 25) that was acquired perpendicular to the descending aorta.Results
Dynamic PC and 4D datasets were successfully in performed in five fetus with heart rates ranging from 129 – 155 bpm. Cardiac gating was reliably performed in all cases. One fetus was excluded due to aliasing. In the remaining cases the aortic arch, descending aorta as well as ascending aorta could be clearly visualized (Figure1). The cross-sectional aortic lumen could be identified in all cases with a mean vessel diameter of the AoD of 7.8 ± 1.2 mm. ROI’s could be reliably defined in the vessel lumen. The aortic flow as well as flow in supra-aortic vessels could be observed (Figure 2). Moreover the blood flow from the pulmonary artery into the aorta via the ductus arteriosus could be visualized. It is important to note that a high flow (> 90 cm/s) can be observed in the ductus arteriosus as the vessel diameter decreases at this part. In all cases a high vortex inside the descending aorta after the ductus arteriosus was observed as shown in Figure 3. The assessed time-velocity curves revealed characteristic biphasic arterial flow waveform patterns with a strong early systolic peak and continuously positive low diastolic blood flow (Figure 4) The average net flow in the descending aorta measured from 2D and 4D acquisitions was similar (22±5 ml/s and 24±4 ml/s).Discussion
The direct fetal gating allowed dynamic functional imaging of the fetal vasculature. The blood flow hemodynamics could be visualized successfully for the first time for the human fetal heart. Quantitative measurements were similar between 4D and 2D phase contrast acquisitions in all cases. The acquisition of 4D data instead of single slice 2D acquisitions may provide a substantial advantage for the evaluation of congenital cardiovascular pathologies as the hemodynamics of the fetal vasculature can be evaluated retrospectively. However, fetal movement is a challenge due to long acquisition times and needs to be addressed in future studies.Conclusion
This preliminary study showed the possibility of visualization and quantitative measurements of blood flow in-utero within the great fetal vessels using 4D phase contrast imaging and direct fetal cardiac gating using Doppler ultrasound. The technique may be beneficial for visualization and quantification of blood flow for complex congenital cardiovascular malformations.Acknowledgements
No acknowledgement found.References
- Wielandner A, Mlczoch E, Prayer D, Berger-Kulemann V. Potential of magnetic resonance for imaging the fetal heart. Semin Fetal Neonatal Med 2013;18:286–97.
- Evers PD, Ranade D, Lewin M, Arya B. Diagnostic Approach in Fetal Coarctation of the Aorta : A Cost-Utility Analysis. J Am Soc Echocardiogr 2017;30:589–94.
- Kording F, Yamamura J, Tavares De Sousa M, Ruprecht C, Hedström
E, Aletras AH, et al. Dynamic fetal cardiovascular magnetic resonance imaging
using Doppler ultrasound gating. J Cardiovasc Magn Reson 2018;20:1–10.
Figures
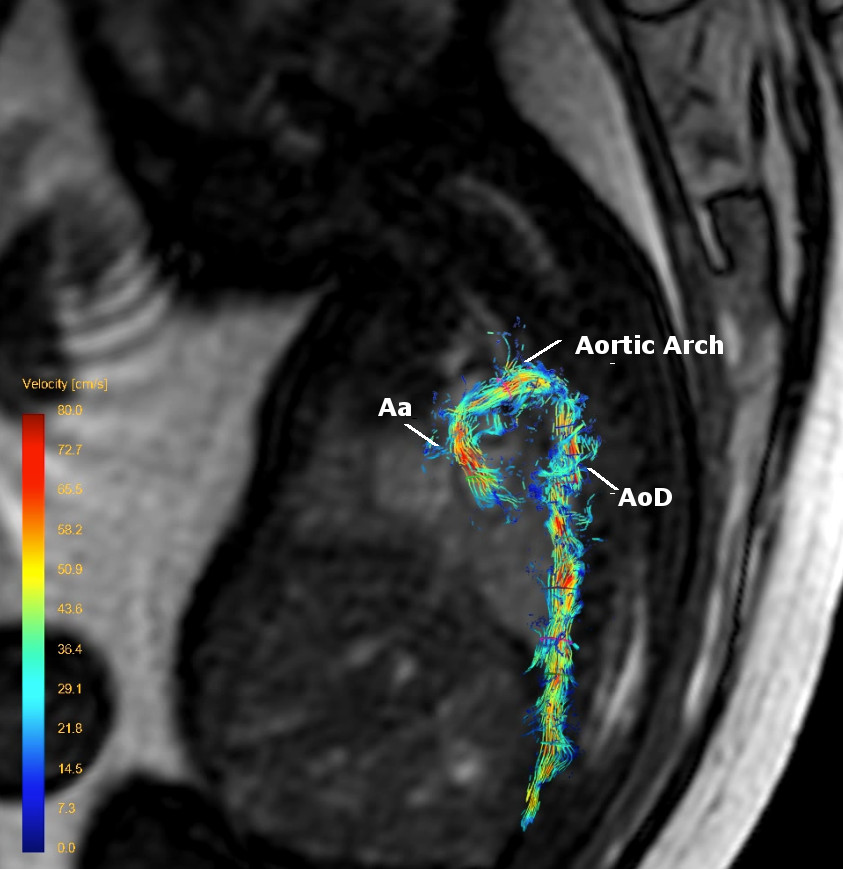
4D PC flow of the aorta of a fetus (gestational age 34 weeks) including ascending aorta (Aa), aortic arch (AA) and descending aorta AoD.
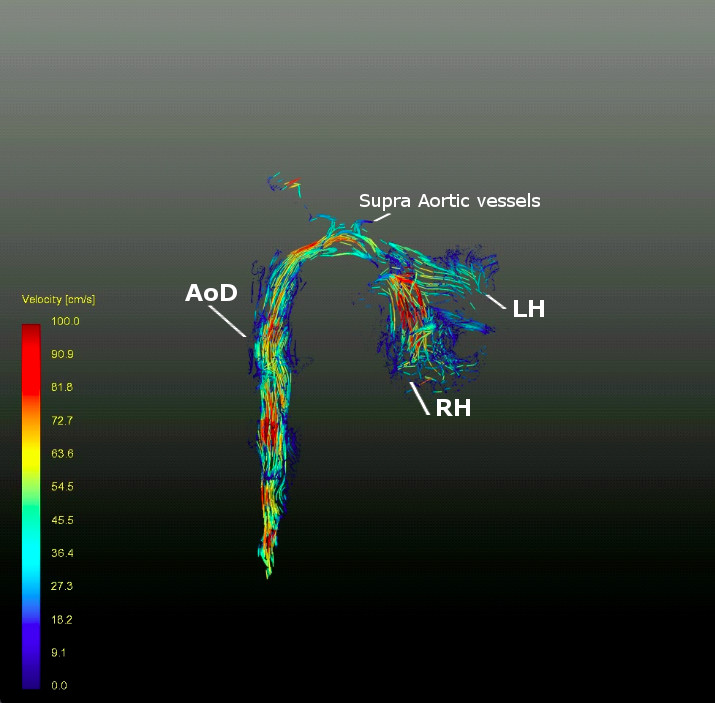
4D PC flow of the aorta of a fetus (gestational age 35 weeks) beginning in the left heart (LH) with clearly visualised supra-aortic vessels and descending aorta (AoD). The beginning of the pulmonary artery in the right heart (RH) can also be seen.
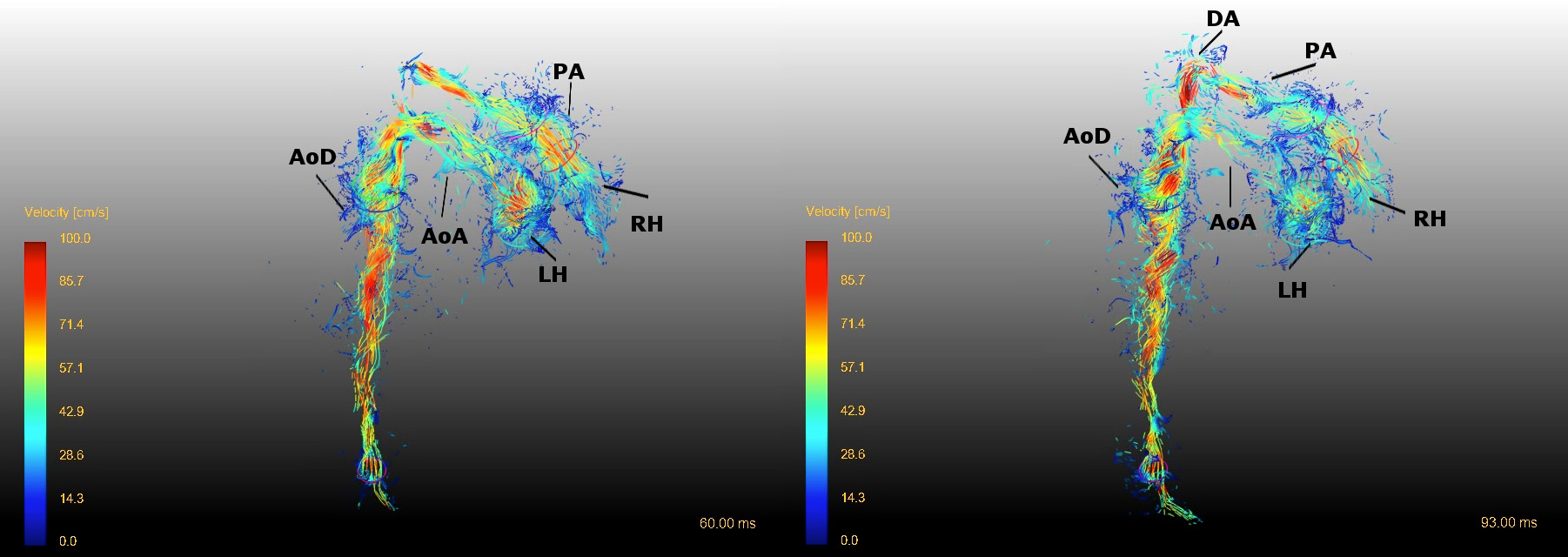
Two different time points in the cardiac cycle Left: Blood flow in the pulmonary artery (PA) does not yet reach the ductus arteriosus. Right: Blood flow of PA reaches the aorta via the DA leading to high flow velocities and vortex inside the aorta.
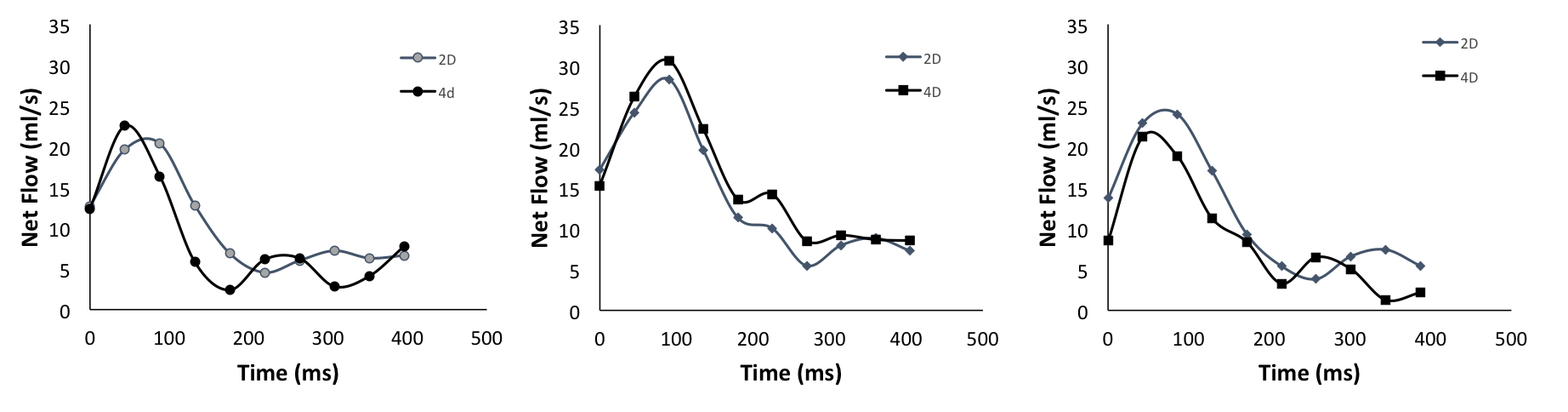
Exemplary comparison of flow curves of 2D and 4D PC acquisition from three different fetus (Gestational week 33, 30 and 35) at the same area of the descending aorta showing typical early systolic peak and continuous positive diastolic flow.