4054
Pelvic endometriosis: The added value of the R2*MFGRE sequence in magnetic resonance imaging1QiLu hospital of Shandong University, Shandong Jinan, China
Synopsis
Purpose: The diagnostic accuracy of endometriosis by conventional magnetic resonance imaging (MRI) sequences is not satisfactory. Minimum endometriosis is particularly challenging to diagnose, which may lead to recurrence or incomplete relief of symptoms after surgery. The R2* multi-fast gradient echo (R2*MFGRE) sequence with the highest sensitivity of hemorrhage in endometriosis may help to address this problem.
Methods: We selected 54 adenomyosis or endometriosis patients and referred them to MRI including the R2*MFGRE sequence and analyzed the results.
Conclusion: The analysis revealed that the R2*MFGRE sequence may provide useful information to help diagnosing endometriosis.
Introduction
Endometriosis is a chronic disease affecting the life of women(1), but the presurgical diagnosis via imaging is challenging. Magnetic resonance imaging (MRI) is wide consensus on a better imaging method. Endometriosis causes bleeding with periodic changes of estrogen and progesterone levels (2,3). Only subacute hemorrhage with methemoglobin is detectable via a high-intensity signal on fat-suppressed T1WI sequences(4-7). However, as non-subacute hemorrhage lesions are not frequently visible via conventional MRI sequences, the detection rate via MRI is not satisfactory. The R2*MFGRE sequence has the highest sensitivity in detecting iron(8) and has an amplification effect; therefore, it is capable in detecting traces of hemosiderin deposition in hemorrhagic lesions. The application of R2*MFGRE sequences may improve the diagnostic accuracy of endometriosis.Methods
Fifty-four patients with clinically suspected adenomyosis or endometriosis were referred to MRI (axial T1WI, IDEAL-T2W, and sagittal FS-T2WI)(GE Signa ExciteⅡ) and the R2*MFGRE sequence. We compared the number of lesions detected by conventional MRI sequences with the number of lesions detected by conventional MRI sequence combined with the R2*MFGRE sequence. All lesions were confirmed by pathological analysis or MRI follow-up after 3–6 months. A Paired t-tests were used for statistical analysis with SPSS software version 20.0.Results
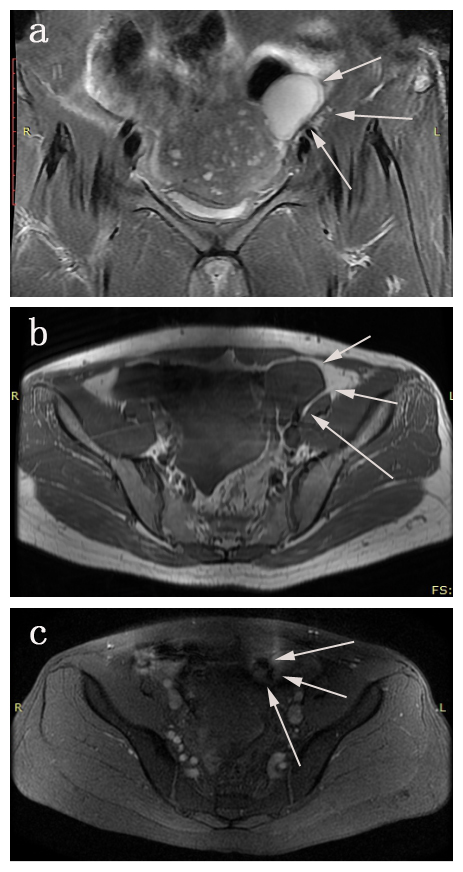
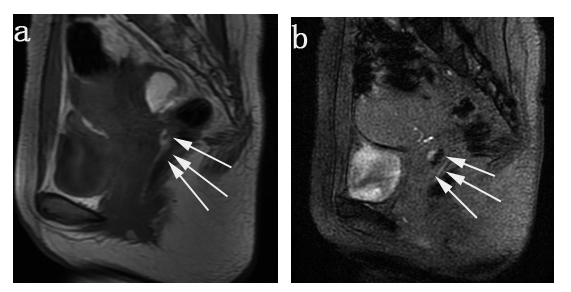
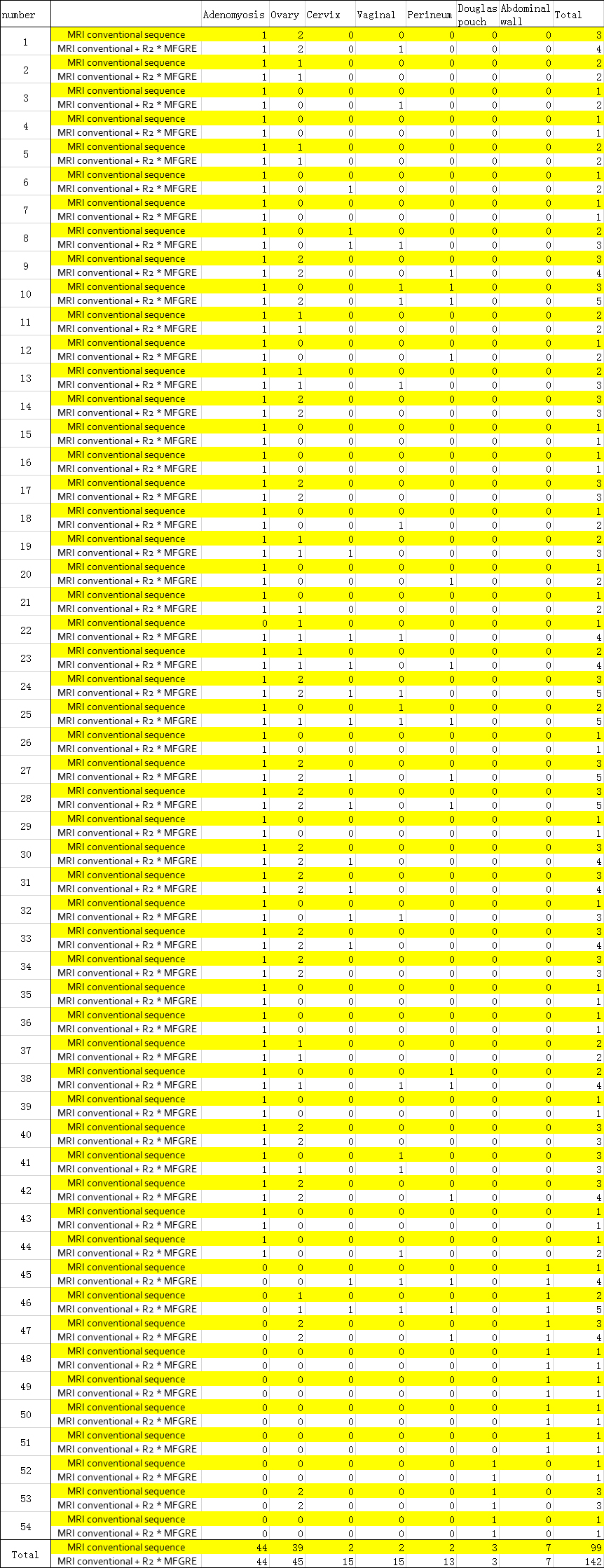
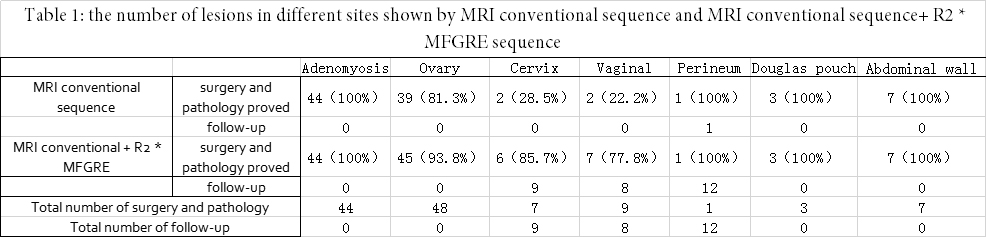
In 54 patients with endometriosis and/or adenomyosis, 99 lesions were found by conventional MRI sequenced, including 44 in adenomyosis, 39 in the ovaries, 2 in the cervix, 2 in the vagina, 2 in the perineum, 3 in the Douglas pouch, and 7 in the abdominal wall. In contrast, 142 lesions were found by conventional MRI sequences combined with the R2*MFGRE sequence,including 44 in adenomyosis, 45 in the ovaries, 15 in the cervix, 15 in the vagina, 13 in perineum, three in the Douglas pouch, and seven in the abdominal wall (Table 1 for details).
In all patients, 99 lesions were detected by conventional sequence, and 43 new lesions were found by adding the R2*MFGRE sequence (Table 2 for details). A paired t-test was used to compare the number of lesions detected in the conventional sequence with the number of lesions detected by the conventional sequence adding R2*MFGRE sequence. The analysis reveals that the conventional sequence combined with the R2*MFGRE sequence may be more advantageous than the conventional sequence for the detection of lesions(P < 0.01).
Discuss
The results showed that the conventional sequence combined with R2*MFGRE sequence could find more lesions in the ovarian, the cervical, the vaginal, and the perineal areas. The R2*MFGRE sequence revealed a maximum lesion diameter of 2.3 cm and an average size of 1.2 cm.
The R2*MFGRE sequence has the highest sensitivity on detecting iron (8) and an amplification effect, so it could detect traces of hemosiderin deposition in hemorrhagic lesions. Addition of the R2*MFGRE sequence for the detecting hemorrhage in minimal lesions of endometriosis is more sensitive than the conventional MRI sequence.
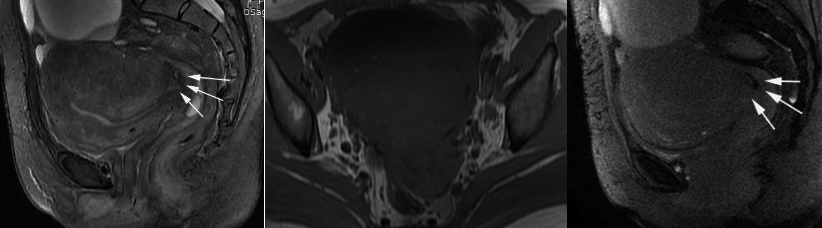
Ovarian endometriosis can be accurately diagnosed via FS-T1WI, but it is easily misdiagnosed as simple ovarian cysts without methemoglobin detected as a high-intensity signal on T1WI, while the hemorrhagic products in the lesion could be sensitively detected by the R2*MFGRE sequence. The lesions in the cervical, vaginal, and perineum areas were too small to be detected via conventional MRI sequences but could be detected using the R2*MFGRE sequence with the amplification effect. Therefore, the R2*MFGRE sequence could reduce the misdiagnosis of ovarian endometriosis and improve the detection rate of small lesions in the cervix, the vagina, and the perineum, which may change the treatment plan.
Adenomyosis can be accurately diagnosed by many characteristics including a point-like high-intensity signal on T2WI and Maximal Junctional Zone thickness > 12 mm(9). Abdominal wall endometriosis is often superficial, which can be clearly detected via conventional sequence for an accurate diagnosis. Although those lesions can be also detected via the R2*MFGRE sequence, the additional value is not significant. Because of influences of the rectal gas, endometriosis in the Douglas pouch could be not clearly visualized via the R2* sequence. Therefore, the added value on detection of the lesions on adenomyosis, the Douglas pouch, and the abdominal wall is not significant.
The R2*MFGRE sequence provides better detection of small endometriotic lesions or ovarian endometriosis compared to conventional MRI sequence but has a lower spatial resolution(10). It cannot be used to diagnose endometriosis independently and need to be combined with conventional sequences.
Conclusion
In term of diagnosing endometriosis, the R2*MFGRE sequence is valuable for the detection of endometriosis in the ovaries, the cervix, the vagina, and the perineum compared to conventional sequences but does not support detecting lesions in adenomyosis, in the Douglas pouch, and in abdominal wall endometriosis.Acknowledgements
First of all, I would like to extend my sincere gratitude to my supervisor, Qing Wang professor, for her instructive advice and useful suggestions on my thesis. I am deeply grateful of her help in the completion of this thesis.
Special thanks should go to my friends who have put considerable time and effort into their comments on the draft.
References
1.Parker JD, Leondires M, Sinaii N, Premkumar A, Nieman LK, Stratton P. Persistence of dysmenorrhea and nonmenstrual pain after optimal endometriosis surgery may indicate adenomyosis. Fertil Steril 2006;86:711–715.
2. Lane BF, Wong-You-Cheong JJ. Imaging of endometrial pathology. Topics inMagnetic Resonance Imaging 2010;21(4):237–45.
3. Garry R, Hart R, Karthigasu KA, Burke C. A re-appraisal of the morphologi-cal changes within the endometrium during menstruation: a hysteroscopic,histological and scanning electron microscopic study. Human Reproduction2009;24(6):1393–401.
4. Bazot M, Darai E, Hourani R, et al. (2004) Deep pelvic endometriosis: MR imaging for diagnosis and prediction of extension of disease. Radiology 232:379–389
5. Siegelman ES, Outwater E, Wang T, Mitchell DG (1994) Solid pelvic masses caused by endometriosis: MR imaging features. Am J Roentgenol 163:357–361
6. Busard MP, Mijatovic V, van Kuijk C, Hompes PG, van Waesberghe JH (2010) Appearance of abdominal wall endometriosis on MR imaging. Eur Radiol 20:1267–1276
7. Busard MP, Mijatovic V, Lu¨ chinger AB, et al. (2012) MR imaging of bladder endometriosis and its relationship with the anterior uterine wall: experience in a tertiary referral centre. Eur J Radiol 81:2106–2111
8. Siegelman ES, Outwater EK (1999) Tissue characterization in the female pelvis by means of MR imaging. Radiology 212:5–18
9. Baker PM,clement PB,Bell DA,et al.Superficial endometriosis of uterine cervix:A report of 20 cases of a process that May be confused with endocervical glandular dysplasia or adenocarcinoma in situ[J]. Int J Gynecol Pathol,1999,18:199-205.
10. Schieda N, Avruch L, Shabana WM, et al. Multi-echo gradient recalled echo imaging of the pelvis for improved depiction of brachytherapy seeds and fiducial markers facilitating radiotherapy planning and treatment of prostatic carcinoma. J Magn Reson Imaging 2015; 41:715–720.
Figures