4053
Cervix heterogeneity: recommendations for scanning the non-pregnant cervix1Centre for Medical Image Computing, University College London, London, United Kingdom, 2Centre for the Developing Brain, King’s College London, London, United Kingdom, 3Division of Women’s Health, King’s College London, London, United Kingdom
Synopsis
Imaging the non-pregnant cervix requires some unique considerations. The cervix has numerous functions including ensuring the fetus is maintained within the uterine cavity until the onset of labour. Alterations in the integrity of cervical tissue are purported to be one of the mechanisms which may contribute to preterm delivery. Quantitative MRI techniques can be used to characterise tissue microstructure however this has not been applied to date to the non-pregnant cervix in the absence of malignancy. This works aims to highlight some limitations and aspects to consider prior to scanning a non-pregnant cervix.
INTRODUCTION
Our long-term objective is to investigate cervical ‘incompetence’ before and between pregnancies to increase the prediction rate for preterm birth (PTB) in the event of a subsequent pregnancy. Thus, an acquisition protocol that is robust to inter and intra subject variability is needed. In this work, we aim to highlight some limitations and aspects to consider prior to scanning a non-pregnant cervix.
PTB is a major healthcare challenge, as they account for most adverse perinatal outcomes, which contributes to over 70% of perinatal mortality in developed countries1. It is the single most important determinant of adverse infant outcome with regards to survival and quality of life1,2. PTB has important financial implications; a one week increase in gestational age among PTB would save the NHS >£120 millions/year3,4. However, for approximately 25% of cases the cause remains unknown and the best predictor for a PTB is a previous PTB5.
The cervix’s primary function is to mechanically maintain the fetus safe within the uterus until the onset of labour6,7. Alterations to the cervix tissue, such scarring from surgery for pre-cancerous treatment or a full-dilatation C-section (in 15% of cases the incision is thought to be in the cervix), increase the risk of PTB8,9. This agrees with previous studies showing a correlation between the biochemical and mechanical properties of the cervical tissue with the obstetric history10,11.
During pregnancy, there are normal progressive alterations in the cellular composition of cervical tissue to prepare for delivery12. Work has been undertaken to quantify and evaluate the cervix during pregnancy to detect cervical ‘incompetence’. Most of the studies are ultrasound based12–14, although there is some research using Magnetic Resonance Images (MRI)15–17. No studies have assessed the non-pregnant cervix utilising MRI outside an oncology setting18,19.
METHODS
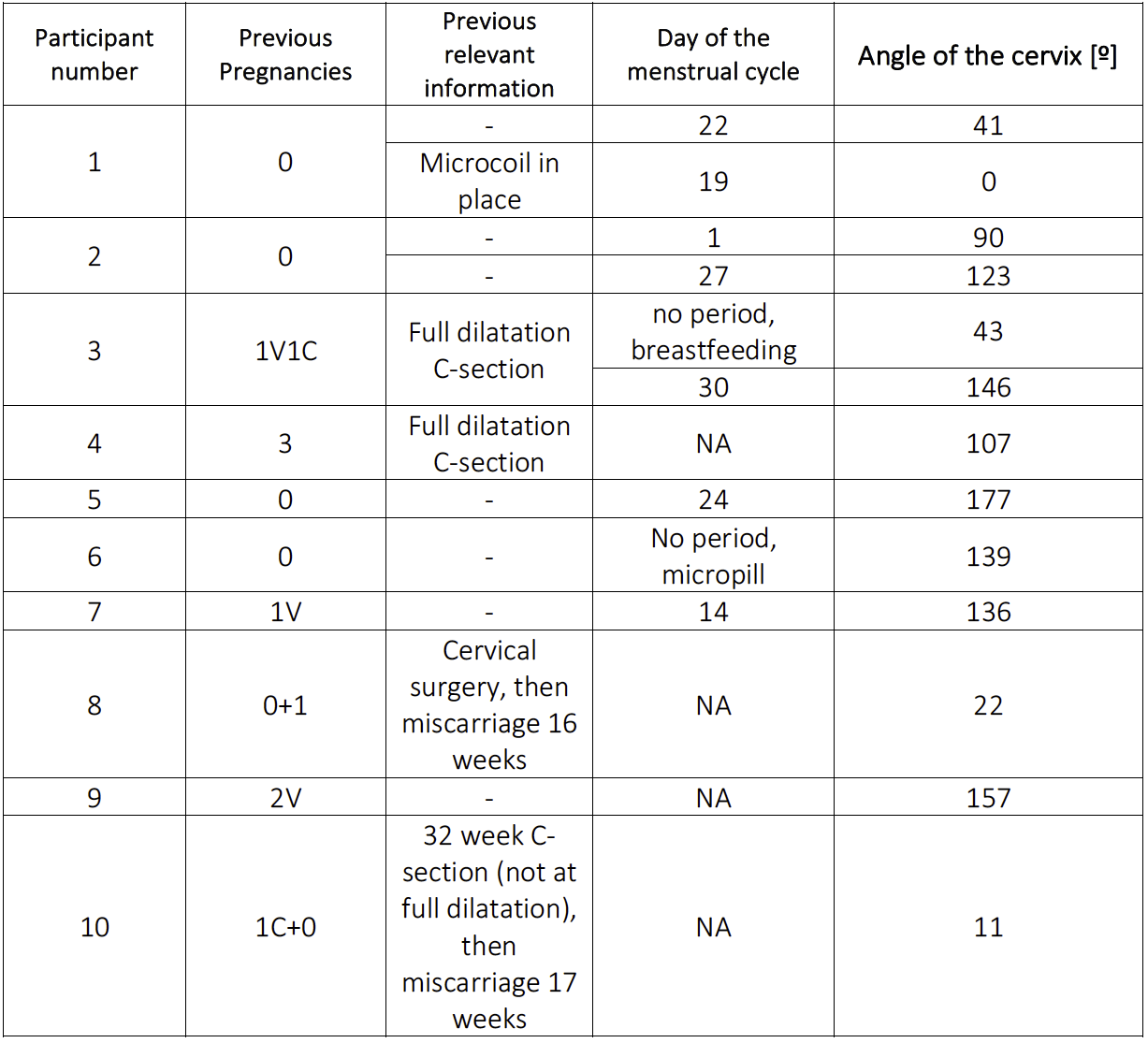
We used various MRI scanning protocols and different planes to scan non-pregnant cervixes from 10 women, from those 3 were scanned twice. We used the anatomical T2 images to measure the cervix orientation (angle of the cervix to the main axis). We measured the cervical width (the diameter in the widest cervical part, perpendicular to the canal) for those participants with multiple scans. We qualitatively assessed the acquisitions in terms of quality and the difficulties encountered during the scan.RESULTS and DISCUSSION
Detailed description of the participants in Table 1. Cervical mean size is in line with previous results20. However, the cervix size, shape and orientation is not static within the individual women.
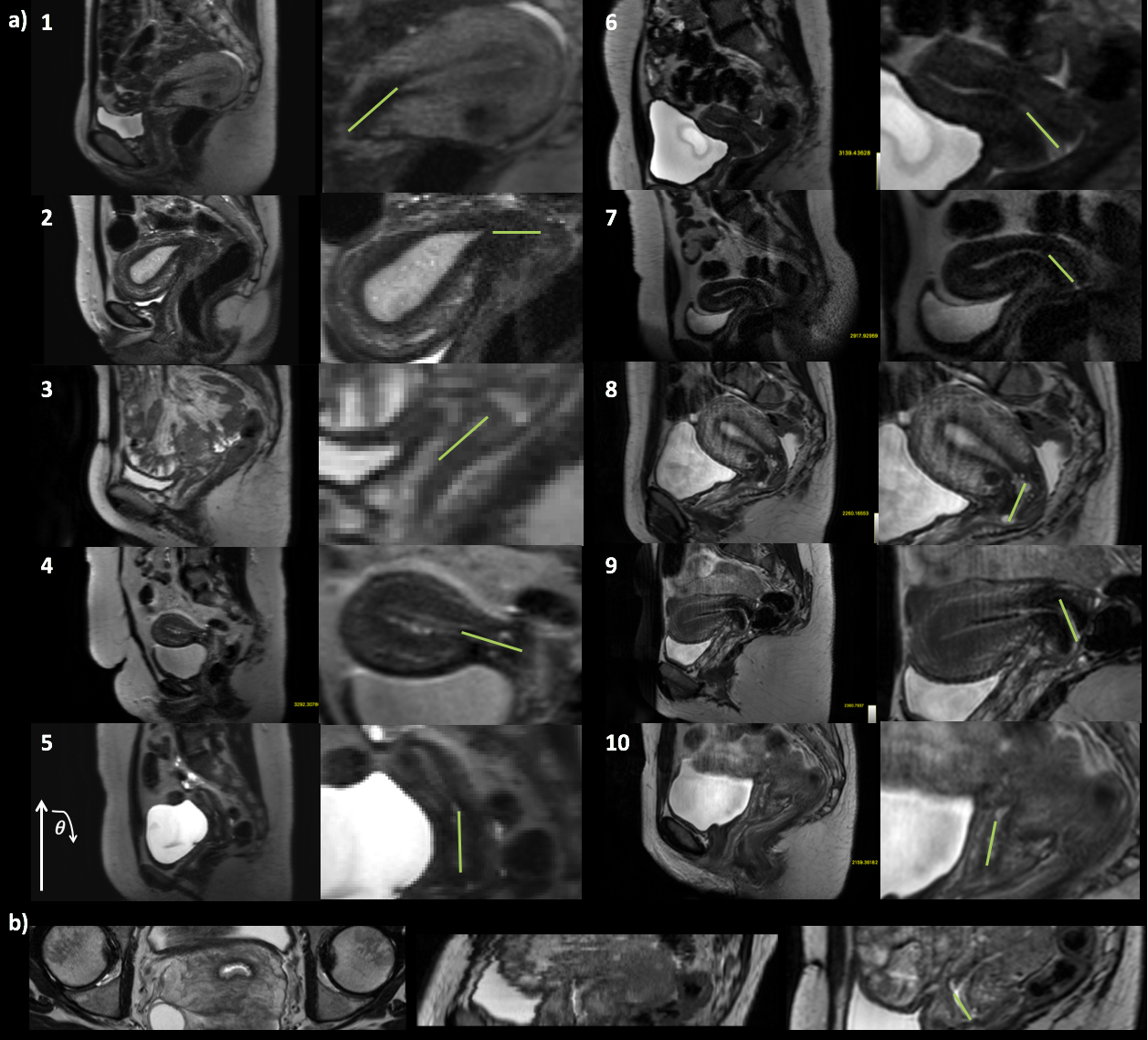
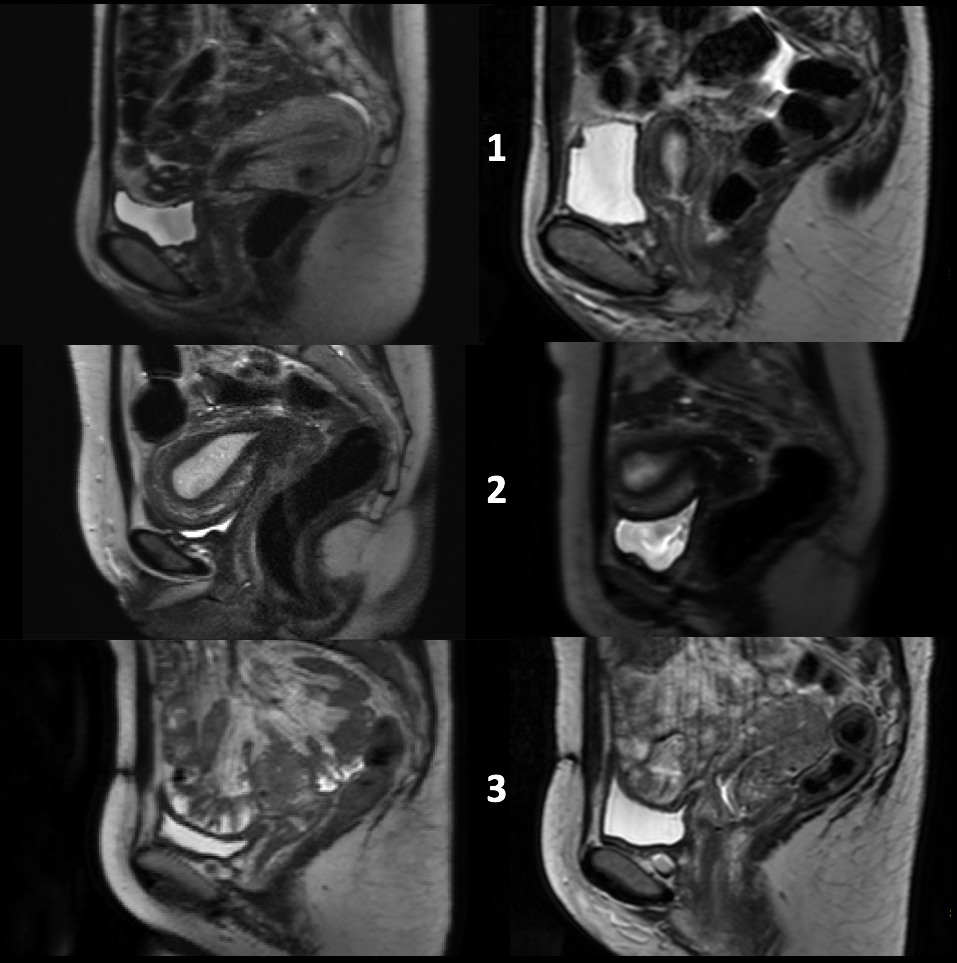
Figure 1 shows the anatomical T2 images for all the participants. As expected21, we have found a wide range of uterus in terms of orientation, from anteverted (the common one) to retroverted. These uterine differences also affect the cervix orientation and position. We want to study the cervical structure regardless of its orientation, instead of acquiring a real axial plane we modified the acquisition to obtain an “oblique-axial” plane (Figure 1b). This new plane, perpendicular to the cervical canal, can potentially be useful to assess the fibre architecture of the cervix17. Figure 2 shows the cervix variability regarding the T2 properties.
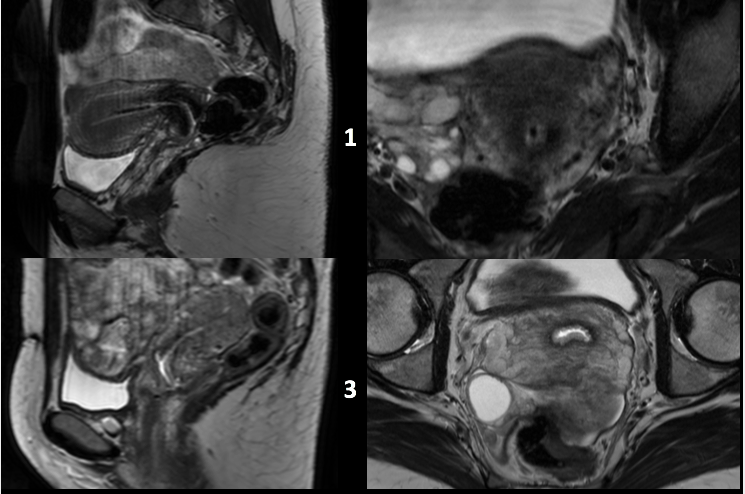
Another variable is the point in the menstrual cycle at which imaging occurs which may change the position, length, aperture and texture of the cervix (Figure 1a and Figure 3). During menstruation is when the cervix is longer. However, menstruation can also alter the image due to the presence of blood in the canal. In a similar manner, in the canal there is usually mucus, which changes consistency during the cycle, changing the image contrast. Additionally, mucus discharge may occur during the scan. Further work to study whether the tissue ‘incompetence’ can be detected in a specific moment of the cycle or as a ratio of two different moments would be valuable.
Finally, standard considerations need to be taken before the imaging. All movement should be avoided, including Keggle exercises. The bladder state (full or empty) might change slightly the cervix position. Gas and bowel movement from the rectum can create image artefacts. Local shimming or image based shimming is thus of key importance. There are some medications available to reduce this (e.g. Buscopan). However, avoiding these facilitates scanning in participants currently breastfeeding.
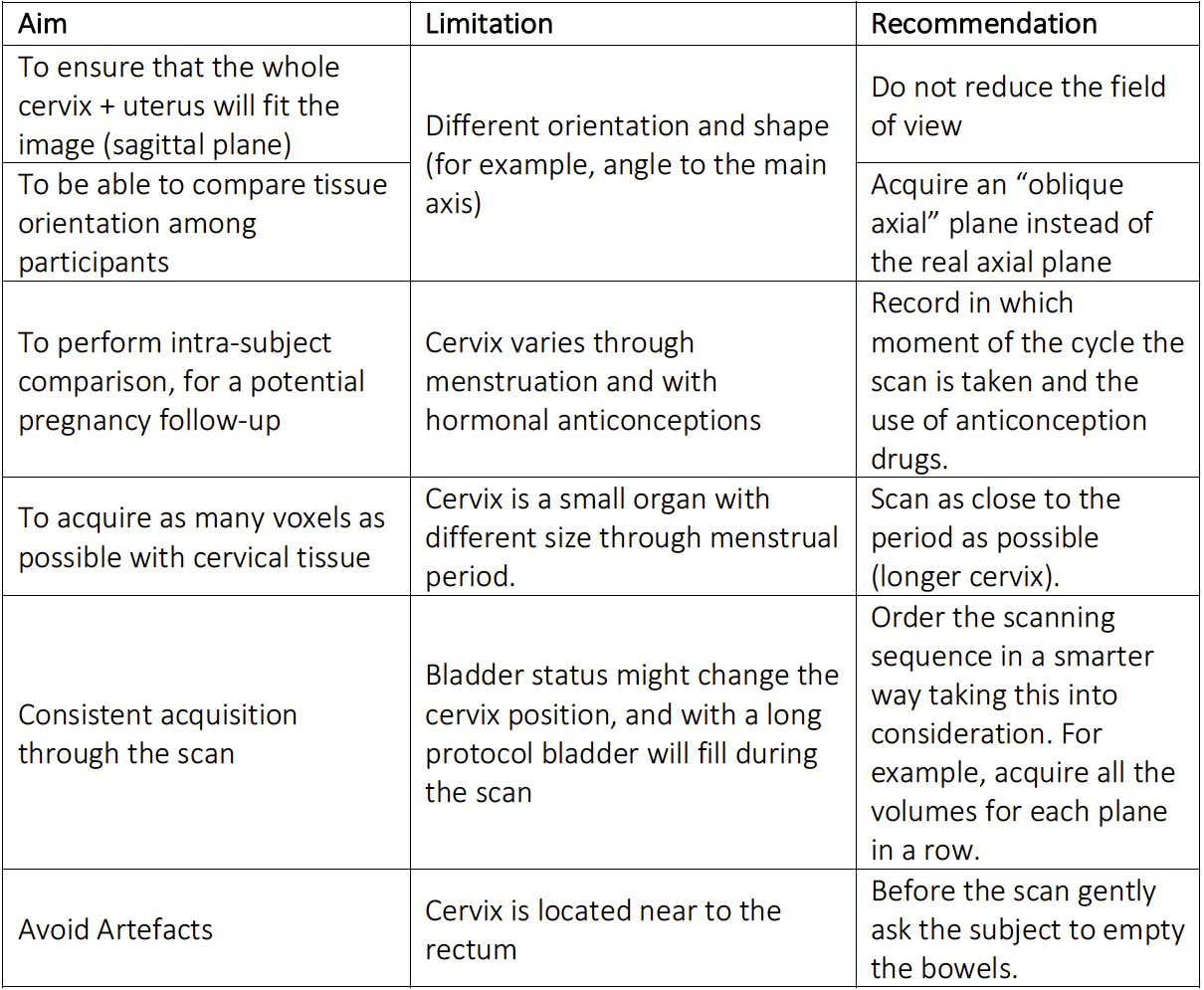
Table 2 presents a summary of the variables to consider before scanning the cervix.
CONCLUSION
In this work, we use our experience after scanning 10 participants to provide some recommendations for imaging the non-pregnant non-cancerous cervix using MRI which may enhance image quality. Similar considerations can be used for to image pregnant and cancerous cervix. Further work will focus on applying these techniques.Acknowledgements
We thank the midwives, obstetricians and radiographers who played a key role in obtaining the data sets. We would also like to thank all participants. EBC was supported by the Engineering and Physical Sciences Research Council (EPSRC ref.: EP/M020533/1). EP is supported by the EPSRC (EP/N021967/1), and EP/M020533/1 and EP/N018702/1 support DCA. JH and this work received funding from the Wellcome Trust (Sir Henry Wellcome Fellowship, [201374/Z/16/z]. This work was also supported by the Wellcome/EPSRC Centre for Medical Engineering [WT 203148/>/16/<].References
1. Saigal S, Doyle LW. An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet. 2008;371(9608):261-269. doi:10.1016/S0140- 6736(08)60136-1.
2. Gardosi JO. Prematurity and fetal growth restriction. Early Hum Dev. 2005;81(1):43-49. doi:10.1016/J.EARLHUMDEV.2004.10.015.
3. Khan KA, Petrou S, Dritsaki M, et al. Economic costs associated with moderate and late preterm birth: A prospective population-based study. BJOG An Int J Obstet Gynaecol. 2015. doi:10.1111/1471-0528.13515.
4. Mangham LJ, Petrou S, Doyle LW, Draper ES, Marlow N. The Cost of Preterm Birth Throughout Childhood in England and Wales. Pediatrics. 2009. doi:10.1542/peds.2008- 1827.
5. Mercer BM, Goldenberg RL, Das A, et al. The preterm prediction study: A clinical risk assessment system. In: American Journal of Obstetrics and Gynecology. Vol 174. ; 1996:1885-1895. doi:10.1016/S0002-9378(96)70225-9.
6. Valentin L, Bergelin I. Intra- and interobserver reproducibility of ultrasound measurements of cervical length and width in the second and third trimesters of pregnancy. Ultrasound Obstet Gynecol. 2002;20(3):256-262. doi:10.1046/j.1469- 0705.2002.00765.x.
7. Martyn F, McAuliffe FM, Wingfield M. The role of the cervix in fertility: is it time for a reappraisal? Hum Reprod. 2014;29(10):2092-2098. doi:10.1093/humrep/deu195.
8. Bruinsma F, Quinn M. The risk of preterm birth following treatment for precancerous changes in the cervix: a systematic review and meta-analysis. BJOG An Int J Obstet Gynaecol. 2011;118(9):1031-1041. doi:10.1111/j.1471-0528.2011.02944.x.
9. Watson HA, Carter J, David AL, Seed PT, Shennan AH. Full dilation cesarean section: a risk factor for recurrent second-trimester loss and preterm birth. Acta Obstet Gynecol Scand. 2017;96(9):1100-1105. doi:10.1111/aogs.13160.
10. Myers KM, Paskaleva AP, House M, Socrate S. Mechanical and biochemical properties of human cervical tissue. Acta Biomater. 2008;4(1):104-116. doi:10.1016/J.ACTBIO.2007.04.009.
11. Myers KM, Feltovich H, Mazza E, et al. The mechanical role of the cervix in pregnancy. J Biomech. 2015;48(9):1511-1523. doi:10.1016/j.jbiomech.2015.02.065.
12. Baños N, Perez-Moreno A, Migliorelli F, et al. Quantitative Analysis of the Cervical Texture by Ultrasound and Correlation with Gestational Age. Fetal Diagn Ther. 2017;41(4):265-272. doi:10.1159/000448475.
13. Baños N, Perez-Moreno A, Julià C, et al. Quantitative analysis of the cervical texture by ultrasound in the mid-pregnancy is associated with spontaneous preterm birth. Ultrasound Obstet Gynecol. 2017. doi:10.1002/uog.17525.
14. Pachtman SL, Ghorayeb SR, Blitz M, et al. Ultrasonic assessment of cervical heterogeneity for prediction of spontaneous preterm birth. Am J Obstet Gynecol. 2017;216(1):S13. doi:10.1016/j.ajog.2016.11.909.
15. de Tejada BM, Faltin DL, Kinkel K, Guittier M-J, Boulvain M, Irion O. Magnetic resonance imaging of the cervix in women at high risk for preterm delivery. J Matern Fetal Neonatal Med. 2011;24(11):1392-1397. doi:10.3109/14767058.2011.552654.
16. Masselli G, Perrone G, Kinkel K, et al. Are Second Trimester Apparent Diffusion Coefficient Values of the Short Uterine Cervix Associated with Impending Preterm Delivery? Radiology. 2016;280(3):897-904. doi:10.1148/radiol.2016150670.
17. Fiocchi F, Nocetti L, Siopis E, et al. In vivo 3 T MR diffusion tensor imaging for detection of the fibre architecture of the human uterus: a feasibility and quantitative study. Br J Radiol. 2012;85(1019):e1009-e1017. doi:10.1259/bjr/76693739.
18. McVeigh PZ, Syed AM, Milosevic M, Fyles A, Haider MA. Diffusion-weighted MRI in cervical cancer. Eur Radiol. 2008;18(5):1058-1064. doi:10.1007/s00330-007-0843-3.
19. Balleyguier C, Sala E, Da Cunha T, et al. Staging of uterine cervical cancer with MRI: guidelines of the European Society of Urogenital Radiology. Eur Radiol. 2011;21(5):1102-1110. doi:10.1007/s00330-010-1998-x.
20. Pardo J, Yogev Y, Ben-Haroush A, Peled Y, Kaplan B, Hod M. Cervical length evaluation by transvaginal sonography in nongravid women with a history of preterm delivery. Ultrasound Obstet Gynecol. 2003;21(5):464-466. doi:10.1002/uog.116.
21. Seppenwoolde Y, Stock M, Buschmann M, et al. Impact of organ shape variations on margin concepts for cervix cancer ART. Radiother Oncol. 2016;120(3):526-531. doi:10.1016/J.RADONC.2016.08.004.
Figures