4049
MRI changes of pubic symphysis injuries in primiparous women1Peking University Third Hospital, Bei Jing, China
Synopsis
Objective: MRI changes of pubic symphysis injuries of primiparas and its relationship with pubic symphysis pain and mode of delivery. Methods: 20 primiparas with MRI, were divided into cesarean, normal vaginal delivery and high-risk vaginal delivery. MR changes were observed. Results : pubic symphysis fibroadenoma avulsion was significantly correlated with pubic symphysis pain. Width of pubic symphysis of the primiparas was wider. primiparas had pubic bone marrow edema, which was not associated with pubic symphysis pain. 1 case pubic fracture. MRI changes were not associated with mode of labor. Conclusion: The severy pubic symphysis pain may be related to the symphysis pubis fibrocartilage avulsion and was not related to the pubis bone marrow edema.
Objective: to observe and identify MRI changes of the pubic symphysis injuries of primiparous women, and to explore its relationship with pubic symphysis pain and mode of delivery.
Methods: prospectively collected 30 primiparas from the Peking University Third Hospital, and performed pelvic floor sagittal, coronal, axial T2WI and fsT2WI after 2-3 days postpartum. According to the mode of delivery, primiparas were divided into cesarean (5 cases), normal vaginal delivery (15 cases) and high-risk vaginal delivery(10 cases,high risk factors including prolonged 2nd stage labor, forceps, age≥33 years old, birth weight > 4000 grams1,2) and their occurrence of pubic symphysis pain and basic data (pre-pregnancy BMI, prenatal BMI, fetal weight and pelvic inclination) were recorded. MR follow-up was performed after 6-8 weeks postpartum. MR changes of pubic symphysis injuries after delivery were observed, including of pubic symphysis fibrocartilage avulsion, pubic symphysis width, pubic bone marrow edema, and pubic fracture. Ten nulliparous women were collected as a control group.
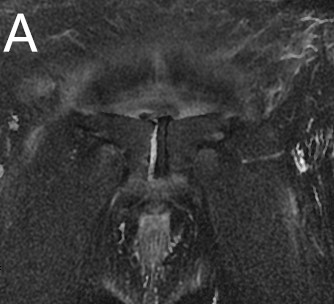
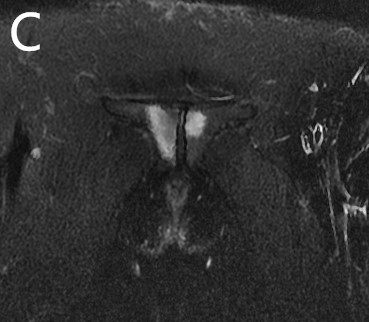
Results :(1) Among the 30 primiparous, 7 had the pubic symphysis fibroadenoma avulsion, which was significantly correlated with severe pubic symphysis pain (P=0.000), but not with the mode of delivery. (X2=2.42, P= 0.298). (2) the width of the pubic symphysis of the primiparous women was wider than that of nulliparous women(t=4.26,P=0.000), but there was no statistical difference between different modes of delivery (P =0.89). (3) 21 of the 30 primiparas had pubic bone marrow edema, which was not associated with severe pubic symphysis joint pain (P =0.071), and there was no statistical difference between different modes of delivery (X2=0.794, P =0.672). (4)pubic bone fracture: only 1 case of cesarean showed left pubic bone inferior fracture; (5) a total of 13 primiparous were followed up for 6-8 weeks after delivery: 3 primiparous who underwent the pubic symphysis fibrocartilage avulsion recovered after conservative treatment (rest in bed and tie the pelvic girdle); width of pubic symphysis returned to normal; pubic bone marrow edema was still present.
Discussion: In present study, postpartum MRI examination found that 7 cases of postpartum pubic symphysis fibrocartilage avulsion were correlated with clinical symptoms of severe symphysis pubic pain. Pubic symphysis fibrocartilage avulsion, accompanied by pubic bone marrow edema, was along the posterior and inferior parasymphyseal region where the levator ani muscle’s pubic portion inserts and undergoes the most stress during pregnancy and vaginal delivery3.The width of pubic symphysis after fibrocartilage avulsion was widened, but all of them did not reach 10mm, which were similar to those found in other literatures in 3 cases of postpartum pubic symphysis fibrocartilage avulsion, with the distance of pubic symphysis joint being 7mm4, 5 and 9mm6. The diagnosis of pubic symphysis injury by ultrasonography and plain view has some limitations. The width of pubic symphysis after 2-3 days postpartum was 3.98±1.13mm, which was wider than that of nulliparous women. this is because that the ovary corpus luteum secretes relaxin during pregnancy, relaxing pubic ligaments, thus increasing the width of pubic symphysis. 1-3mm of pubic symphysis width is postpartum normal physiological change. Susanne et al. measured the pubic symphysis distance of nulliparous women at 5.0mm and at 6.0mm 2 weeks after childbirth , which was somewhat different from our data, considering that it was caused by the different pelvic structures of Asian and European women. Pubic bone marrow edema, also known as contusion, indicates a nonspecific stress injury of the pubic bone. This study showed that pubic bone marrow edema, were common in the three kinds modes of delivery, including cesarean, meaning that not only direct mechanical force during fetal childbirth descent, but also sustained, long-term stress by the fetus during pregnancy and amniotic fluid would lead to pubic bone marrow edema. After 6-8 weeks postpartum, only 1 case edema disappeared, even 2 cases enlarged edema range. The pubic bone edema had not yet recovered. Most of the stress injuries were cured within 6-8 weeks, but recovery of the pubic symphysis injuries took 2-5 months 7.
Conclusion: there was no significant correlation between the severity of postpartum pubic symphysis injury and the mode of delivery. The severy pubic symphysis pain may be related to the symphysis pubis fibrocartilage avulsion and was not related to the pubis bone marrow edema. The width of pubic symphysis returned to normal at 6-8 weeks postpartum and the pubic bone marrow edema did not return.
Acknowledgements
No acknowledgement found.References
1. Kearney R, Miller J M, Ashton-Miller J A, et al. Obstetric factors associated with levator ani muscle injury after vaginal birth [J]. Obstet Gynecol, 2006, 107(1): 144-149.
2. Low L K, Zielinski R, Tao Y, et al. Predicting Birth-Related Levator Ani Tear Severity in Primiparous Women: Evaluating Maternal Recovery from Labor and Delivery [J]. Open J Obstet Gynecol, 2014, 4(6): 266-278.
3. Lien K-C, Mooney B, DeLancey JOL, Ashton-Miller JA. Levator ani muscle stretch induced bysimulated vaginal birth. Obstet Gynecol. 2004; 103:31–40.
4. Brandon C, Jacobson J A, Low L K, et al. Pubic bone injuries in primiparous women: magnetic resonance imaging in detection and differential diagnosis of structural injury [J]. Ultrasound Obstet Gynecol. 2012, 39(4): 444-451.
5. Wurdinger S, Humbsch K, Reichenbach J R, et al. MRI of the pelvic ring joints postpartum: normal and pathological findings [J]. J Magn Reson Imaging, 2002, 15(3): 324-329.
6. Kurzel R B, Au A H, Rooholamini S A, et al. Magnetic resonance imaging of peripartum rupture of the symphysis pubis [J]. Obstet Gynecol, 1996, 87(5 Pt 2): 826-829.
7. Datir AP, Saini A, Connell A, Saifuddin A. Stress-related bone injuries with emphasis on MRI. Clinical Radiology. 2007; 62:828–836
Figures