4042
Imaging characteristics of ovarian sclerosing stromal tumor1Department of Radiology, Shenzhen Mental Health Center, Shenzhen Kangning Hospital, Shenzhen, China
Synopsis
Sclerosing stromal tumor (SST) is an extremely rare benign sex cord-stromal tumor of the ovary. Due to its clinical presentation and imaging findings are similar to those of borderline or malignant epithelial tumors and other sex cordstromal tumors, accurate preoperative clinical diagnosis can be very difficult. This study evaluated magnetic resonance imaging and computed tomography features and pathological findings of SST of ovary and the correlation between them. The results demonstrated that MRI examination with dynamic and delayed enhancement could play a critical role in making appropriate diagnosis preoperatively when combined with clinical information.
Introduction
Sclerosing stromal tumor (SST) is a very rare benign sex cord-stromal tumor (SCST) of the ovary. More than 80% of SST were observed in young women in the 2nd and 3rd decades of life1,2. Because its clinical presentation and imaging findings are similar to those of borderline or malignant epithelial tumors and other sex cordstromal tumors, accurate preoperative clinical diagnosis can be difficult. The definite diagnosis of SST is made based on post-operative pathological examination after oophorectomy, and laparoscopic surgery is seldom performed in SST cases. Therefore, accurate preoperative imaging diagnosis can be helpful to perform minimally invasive surgery and reduce unnecessary salpingo-oophoretomy for SST. The aim of this study was to evaluate magnetic resonance imaging (MRI) and computed tomography (CT) features and pathological findings of SST of ovary and the correlation between them.Methods
The MRI (n=8), CT (n=3) findings and clinical pathological data of SST proven by pathology were studied, and imaging features and pathological expression were analyzed.Results
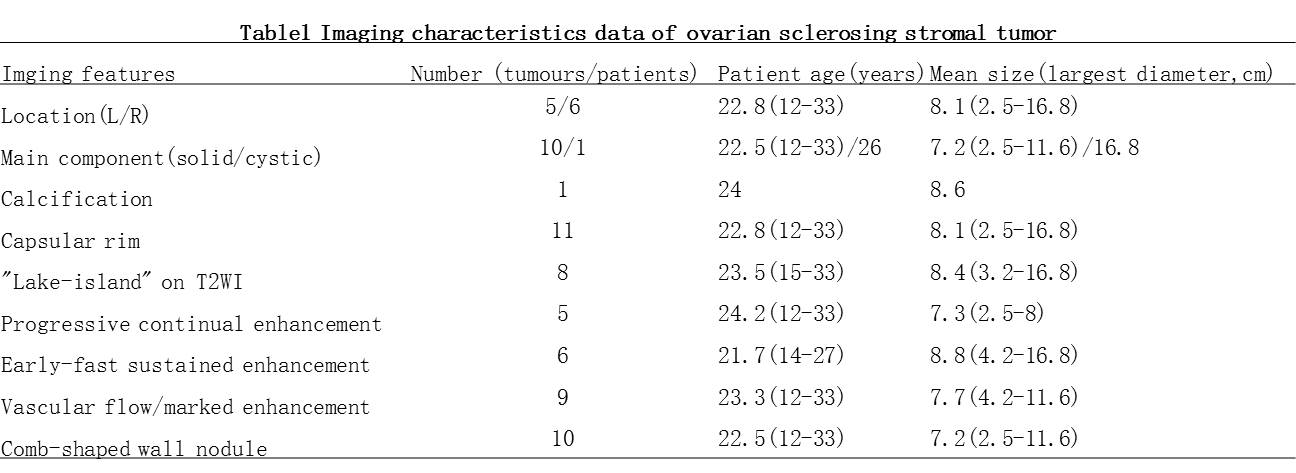
Table 1 shows the imaging characteristics of
these SSTs. Among the 11 cases with SST of ovary, 5 of them located in the left
ovary and 6 cases right. The tumors size varied from 2.5~16.8 cm
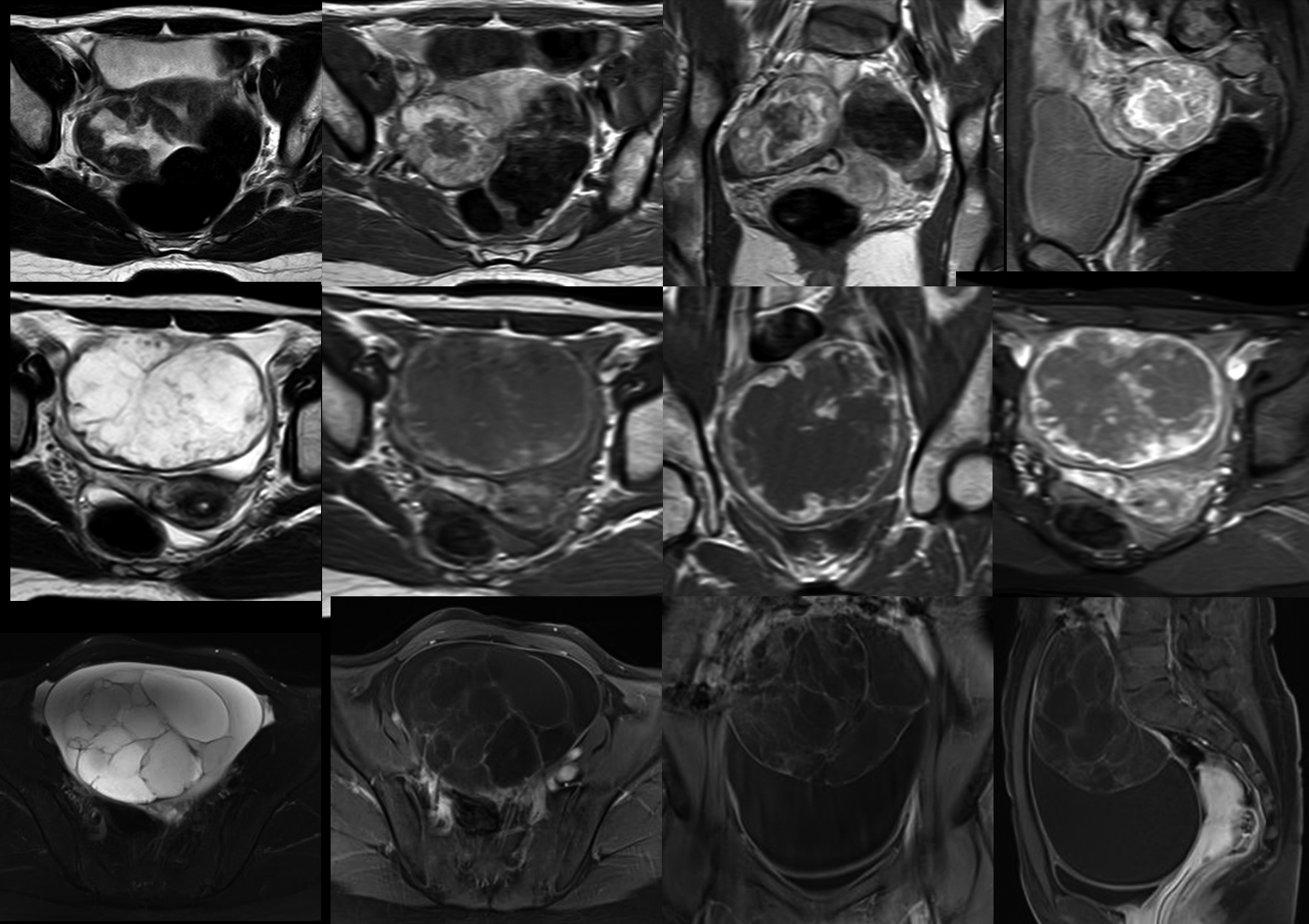
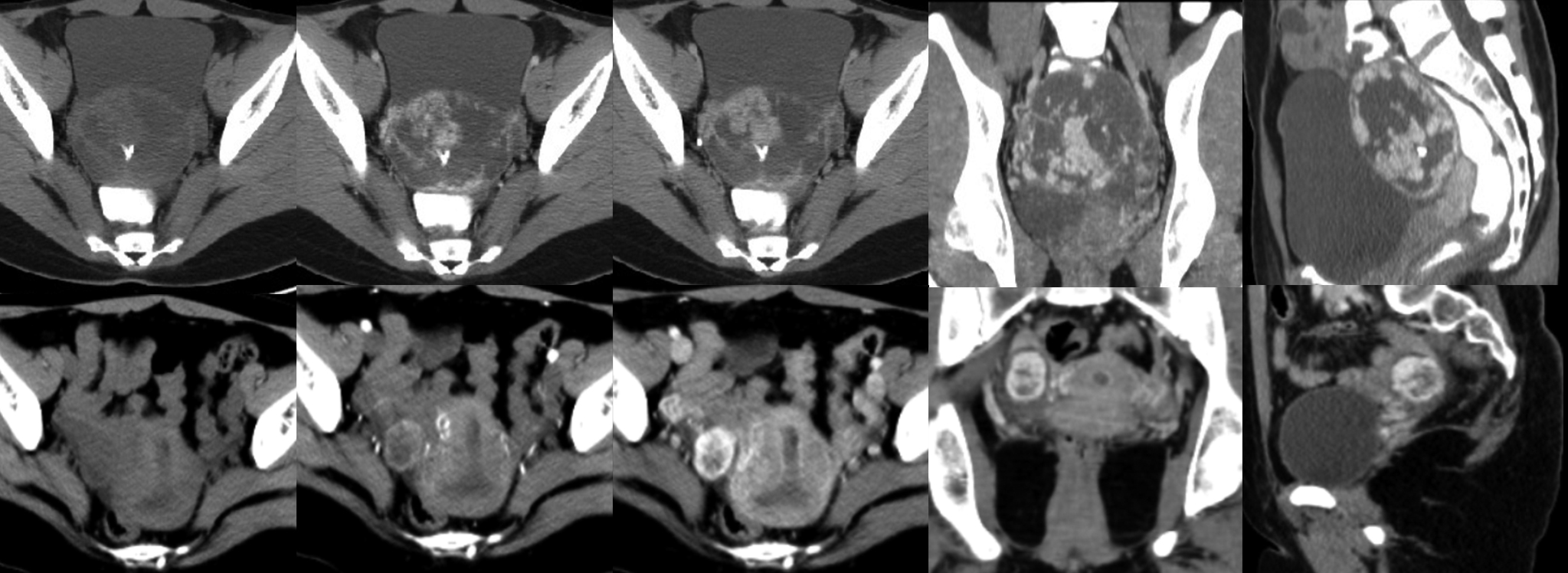
in the largest diameter. Unenhanced CT scans showed mixed and low density, and MRI T1-weighted imaging (T1WI) showed
hypointensity, while mixed and hyperintensity in T2-weighted imaging (T2WI). The masses were showed with cystic and solid density, 10
cases (90.9%) were predominantly solid tumors, and 1 case (9.1%) predominantly cystic tumor. Only one of the 3
CT cases found a flaky calcification (Figure 1-2). In all cases, the outer surface of the
tumor contained a capsular and complete smooth rim and comb-shaped wall nodule
in internal surface. Ten cases of CT/MRI images showed a little ascites around
the mass (90.9%). Only one case showed no ascites, but a small amount of light
ascites was seen during surgery. Eight tumors (72.7%) showed “lake-island” sign
on T2WI (Figure 1).
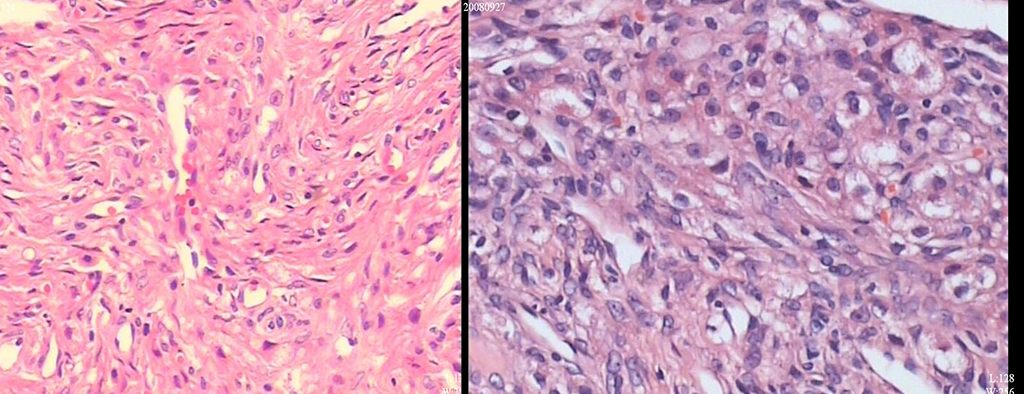
According to the mode of enhancement: ①Progressive centripetal continual enhancement: In 5 cases (45.5%) the curve of enhancement of the solid components appeared as straight line shape, but the cystic components has no enhancement in the whole course (Figure 1-2).②Early -fast sustained enhancement: the curve of enhancement of the solid components in 6 cases (54.5%) appeared as peak-shape, but the cystic components has no enhancement in the whole course. One case (9.1%) showed a multiloculated cystic mass with irregularly thickened septae and tumor wall (Figure 1-2). The solid components in the 10 predominantly solid mass are comb-like and wheel-like enhanced. Vascular flow signals or/and marked enhancement of blood vessels in 9 lesions (2 CT and 7 MRI cases). Pathologic examination all the cases demonstrated pseudolobule patterns, spindle cells, collagenous areas, edematous hypocellular areas and prominent vasculatures (Figure 3).
Discussion
The SSTs were the only subtype of benign SCSTs which were enhanced distinctly3. We found that most SSTs were the tumors with“lake-island” sign on T2WI and progressive centripetal/early-fast continual and comb- or wheel-like enhancement. The explanation may be that the tumor has a characteristic microscopic pattern in which the pseudo-separation of the cell-rich region is separated by the hypocellular region of the loose collagen and edematous connective tissue. Pathologically prominent vascular components also explain the continual obviously enhancement of the image.Conclusion
Most of MRI, CT manifestation and pathological findings of SST had characteristic features. Generally, MRI examination with dynamic and delayed enhancement could make appropriate diagnosis preoperatively when combined with clinical information.Acknowledgements
No acknowledgement found.References
1. A. Chalvardjian, and R. E. Scully, 'Sclerosing Stromal Tumors of the Ovary', Cancer, 31 (1973), 664-70.
2. E. I. Kaygusuz, S. Cesur, H. Cetiner, et al., 'Sclerosing Stromal Tumour in Young Women: Clinicopathologic and Immunohistochemical Spectrum', J Clin Diagn Res, 7 (2013), 1932-5.
3. M.
Horta, and T. M. Cunha, 'Sex Cord-Stromal Tumors of the Ovary: A Comprehensive
Review and Update for Radiologists', Diagn
Interv Radiol, 21 (2015), 277-86.
Figures