4040
Clinical utility of susceptibility-weighted MR sequences for the evaluation of adnexal torsion1Department of Radiology, Tokushima University, Tokushima, Japan, 2Department of Radiological Technology, Tokushima Bunri University, Kagawa, Japan
Synopsis
Because venous thrombus within the twisted vascular pedicle is a specific pathological finding for adnexal torsion, to reveal the thrombus by MRI may be diagnostic. Surgically proven five benign ovarian masses with torsion were retrospectively evaluated. High intensity venous thrombus within the twisted vascular pedicle on fat-saturated T1WI were detected in four lesions (80%) but not in one acute torsion, whereas signal voids on susceptibility-weighted MR sequences (SWS) were detected in all five lesions (100%). SWS also revealed hemorrhagic infarction of all five ovarian masses with torsion, whereas fat-saturated T1WI could demonstrate high intensity hemorrhagic infarction in four lesions.
Introduction
Adnexal torsion is an uncommon gynecologic emergency caused by twisting of an adnexal mass, which is usually an ovarian tumor or cyst, and rarely normal ovary, along the vascular pedicle 1, 2. Typical adnexal torsion may cause acute abdomen, however, some patients may complain mild, intermittent pain, or may be almost asymptomatic. In such subclinical cases following subacute to chronic courses, the twisted benign ovarian mass may mimic malignancy. Complete torsion requires immediate surgical treatment because if it is left untreated, hemorrhagic necrosis and infection can lead to severe complications. Because venous thrombus within the twisted vascular pedicle is a specific pathological finding for adnexal torsion, to reveal the thrombus by MRI may be diagnostic. Fujii et al. reported that venous thrombus might contribute to the high intensity on DWI, however, malignant tumors may also show high intensity on DWI 3. Fat-saturated T1WI (fsT1WI) may be useful in detecting thrombus in the vascular pedicle but Rha et al. reported this finding in only 16% of cases, possibly T1WI can reveal only subacute hemorrhage with methemoglobin as high intensity 4. Susceptibility-weighted MR sequences (SWS) such as SWI and SWAN are MR techniques which maximize sensitivity to susceptibility effects, and have exquisite sensitivity to blood products such as deoxyhemoglobin and hemosiderin resulting from acute and chronic hemorrhage, respectively 5, 6. Takeuchi et al. reported a case of adnexal torsion exhibiting prominent signal voids due to venous thrombus in the twisted vascular pedicle on SWI 7. The purpose of this study is to evaluate the feasibility of SWS for the diagnosis of adnexal torsion.Methods
Five women (mean age 50 years) with pathologically proven adnexal torsion including two fibroma/fibrothecomas, two serous cystadenomas, and one corpus luteum cyst who had undergone MRI examinations including SWS before surgery were retrospectively evaluated. Fast spin-echo T2WI, gradient-echo T1WI with fat-saturation, DWI (b=0, 800 s/mm2) and SWS (SWI or SWAN) were obtained for four patients with 3-T superconducting MRI systems (Discovery MR750 or Signa HDx, GE), and for one patient with pregnancy with 1.5-T unit (Signa Excite HDx, GE). Two radiologists qualitatively evaluated the images for the presence of signal voids within masses and twisted vascular pedicles on SWS, and of high intensity on fsT1WI and DWI. The reviewers examined all images of the cases independently and then resolved discrepancies by consensus. The mean ADC values in the masses (solid portion, or wall of the cystic masses) and twisted vascular pedicles were measured respectively in a circular ROI in one representative region from ADC maps on the workstation (AW4.2).Results and Discussions
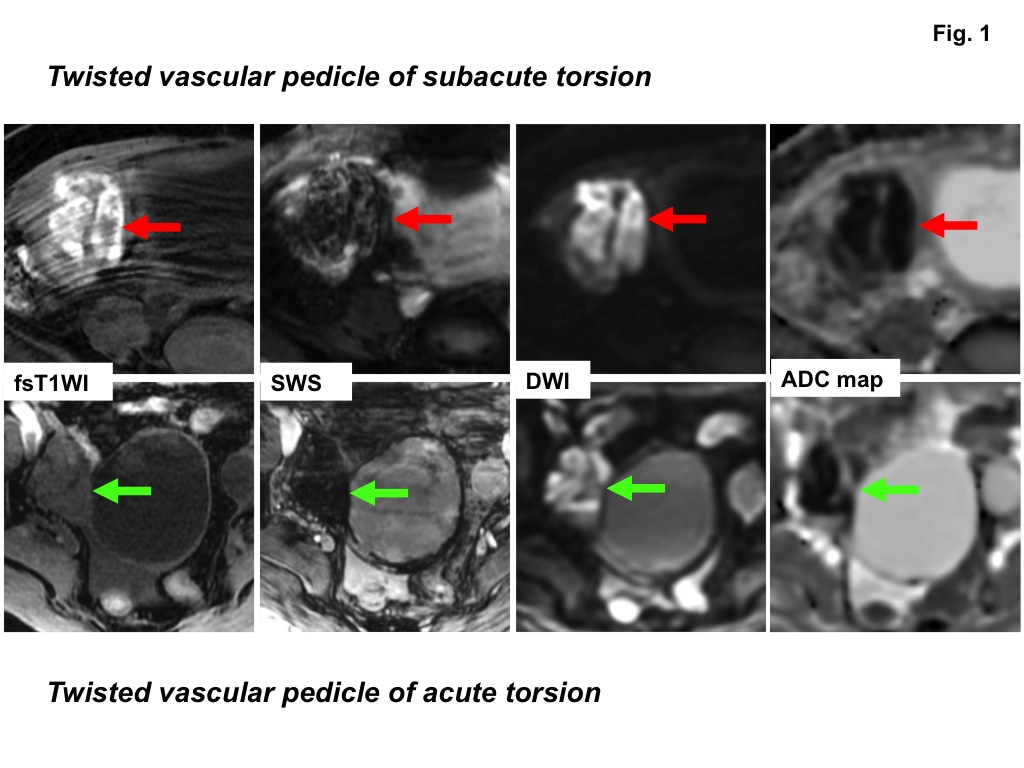
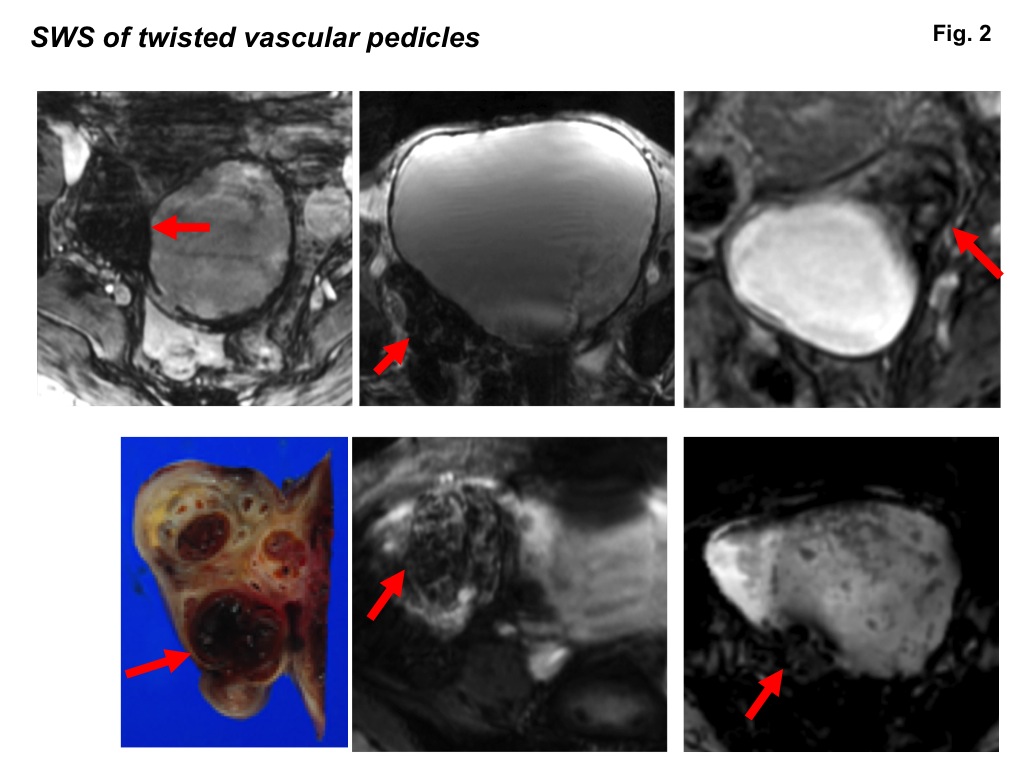
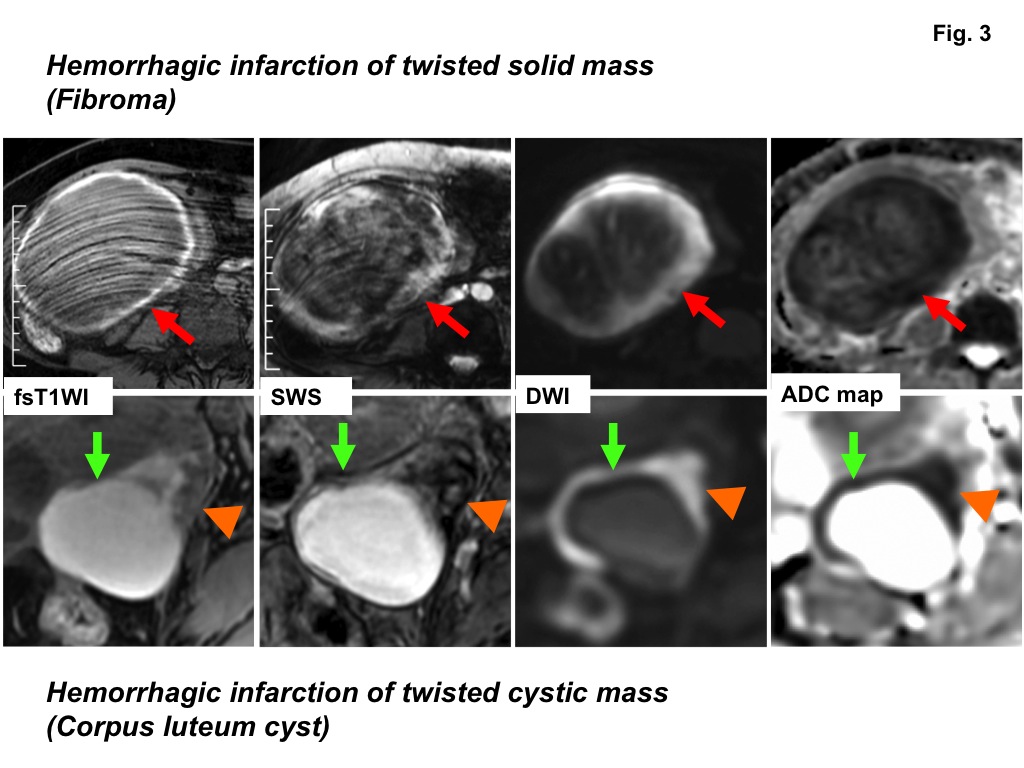
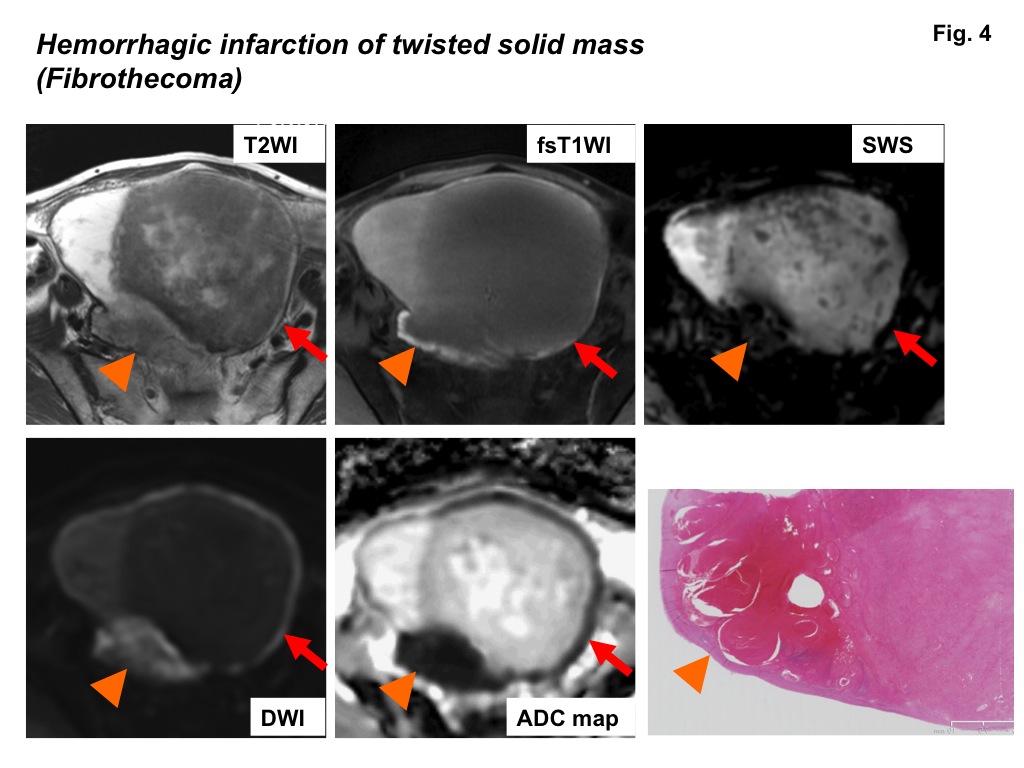
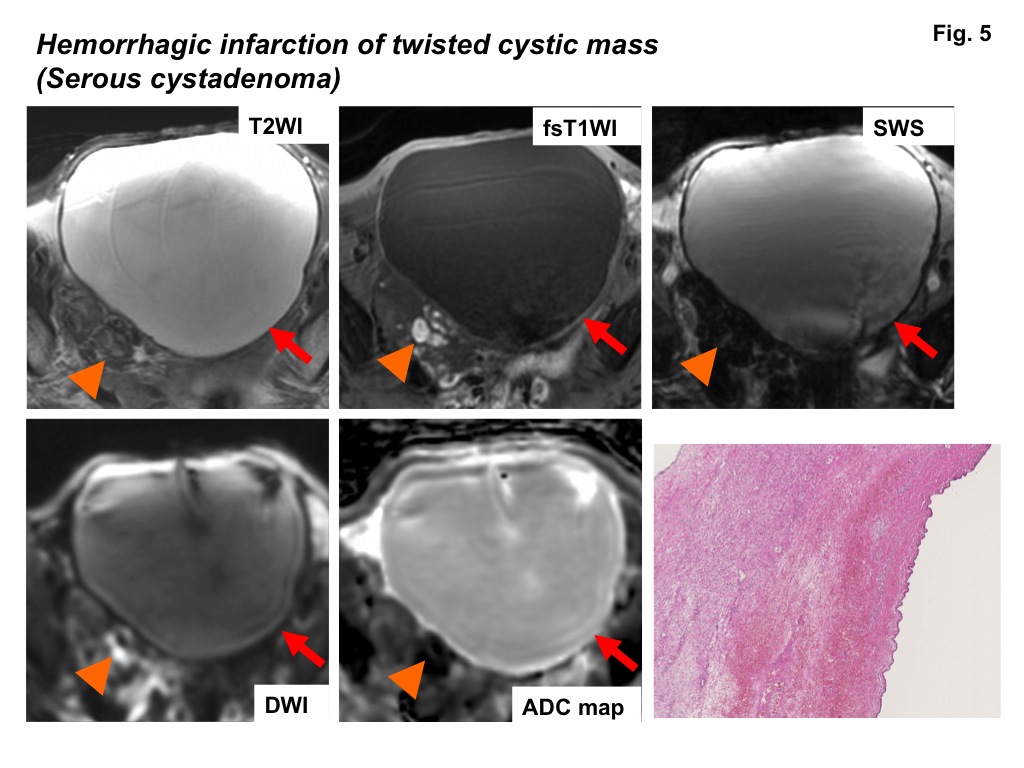
High intensity on fsT1WI was detected in the vascular pedicles of four subacute to chronic adnexal torsions (80%), whereas the vascular pedicle of the other one acute torsion showed low intensity (Fig. 1). High intensity on DWI and signal voids on SWS were detected in all vascular pedicles (100%), and all five vascular pedicles showed low ADC (0.43 to 0.71, mean 0.53 x 10-3 mm2/s) (Fig. 2-4). These results suggested that high intensity due to the T1 shortening effect of methemoglobin may reflect only subacute hemorrhage, whereas signal voids on SWS may reflect all phases of hemorrhage, especially deoxyhemoglobin in acute venous thrombus and may be more feasible for the diagnosis of adnexal torsion. High intensity on DWI due to water diffusion restriction by the venous thrombus may also suggestive for adnexal torsion, however, high intensity on DWI is not specific because malignant tumors may also show high intensity reflecting high cellularity of cancerous tissue. High intensity on fsT1WI was detected in the wall of two of three cystic masses and all two solid masses, whereas SWS demonstrated signal voids in the wall of all three cystic masses and all two solid masses (100%) reflecting hemorrhagic infarction 7, 8 (Fig. 3-5). DWI shows high intensity in the wall of all three cystic masses and all two solid masses. The wall of one of three cystic masses and two solid masses showed low ADC (0.55 to 0.82) possibly due to hemorrhagic infarction (Fig. 3, 4) and the wall of the other two cystic masses showed high ADC (2.87 and 3.09) possibly due to marked congestion and edema co-existing with hemorrhagic infarction, which may cause signal increase on DWI due to T2 shine-through effect 3, 9-11 (Fig. 5).Conclusion
We conclude that the demonstration of venous thrombus in twisted vascular pedicle of adnexal torsion by SWS may provide valuable diagnostic findings. In addition, SWS may be also useful in evaluating the hemorrhagic infarction associated with adnexal torsion.Acknowledgements
No acknowledgement found.References
1) Béranger-Gibert S, Sakly H, Ballester M, et al. Diagnostic Value of MR Imaging in the Diagnosis of Adnexal Torsion. Radiology 2016;279:461-470.
2) Moribata Y, Kido A, Yamaoka T, et al. MR imaging findings of ovarian torsion correlate with pathological hemorrhagic infarction. J Obstet Gynaecol Res 2015;41:1433-1439.
3) Fujii S, Kaneda S, Kakite S, et al. Diffusion-weighted imaging findings of adnexal torsion: initial results. Eur J Radiol 2011;77:330-334.
4) Rha SE, Byun JY, Jung SE, et al. CT and MR imaging features of adnexal torsion. Radiographics 2002;22:283-294.
5) Haacke EM, Xu Y, Cheng YC, et al. Susceptibility weighted imaging (SWI). Magn Reson Med 2004;52:612-618.
6) Boeckh-Behrens T, Lutz J, Lummel N et al. Susceptibility-weighted angiography (SWAN) of cerebral veins and arteries compared to TOF-MRA. Eur J Radiol 2012;81:1238-1245.
7) Takeuchi M, Matsuzaki K, Harada M. Susceptibility-weighted Imaging of Ovarian Torsion: A Case Report. Magn Reson Med Sci 2015;14:355-358.
8) Kawai N, Kato H, Kanematsu M, et al. Usefulness of T2*-weighted MRI in the detection of adnexal torsion. Acta Radiol Open 2016;5:2058460116645375.
9) Kato H, Kanematsu M, Uchiyama M, et al. Diffusion-weighted imaging of ovarian torsion: usefulness of apparent diffusion coefficient (ADC) values for the detection of hemorrhagic infarction. Magn Reson Med Sci 2014;13:39-44.
10) Bekci T, Polat AV, Aslan K, et al. Diagnostic performance of diffusion-weighted MRI in the diagnosis of ovarian torsion: comparison of torsed and nonaffected ovaries. Clin Imaging 2016;40:1029-1033.
11) CÖzdemir O, Metin Y, Metin NO, et al. ontribution of diffusion-weighted imaging to conventional MRI for detection of haemorrhagic infarction in ovary torsion. BMC Med Imaging 2017;17:56.
Figures