4039
MR manifestations of polypoid endometriosis: Clinical feasibility of conventional and advanced MR techniquesMayumi Takeuchi1, Kenji Matsuzaki2, and Masafumi Harada1
1Department of Radiology, Tokushima University, Tokushima, Japan, 2Department of Radiological Technology, Tokushima Bunri University, Kagawa, Japan
Synopsis
Polypoid endometriosis (PE) is a rare variant of benign endometriosis and may mimic malignant tumors. MR manifestations of five women with pathologically proven PE were retrospectively evaluated. PE was associated with pelvic endometriosis (4/5) with “black rim sign” (3/5), and with adenomyosis (5/5). PE showed high intensity on T2WI (5/5), high intensity hemorrhagic foci on T1WI (3/5), hemorrhagic signal voids on susceptibility-weighted sequences (2/2), high intensity on DWI (4/4) with relatively high ADC values (mean, 1.67 x 10-3 mm2/s), gradually increasing time-intensity curve pattern on DCE-MRI (4/4) with intense contrast-enhancement (4/5) or weak contrast-enhancement (1/5, with malignant transformation).
Introduction
Polypoid endometriosis is a rare variant of benign endometriosis with histological features resembling endometrial polyps 1-3. Polypoid endometriosis may frequently affect peri-menopausal women, and hormonal factors can play a role in its pathogenesis. Polypoid endometriosis may form multiple polypoid nodules in the peritoneal cavity or endometriotic cyst mimicking malignant tumors on imaging examination, at operation, and on gross pathologic examination 2-4. Takeuchi reported that high intensity masses with the presence of surrounding fibrous tissue showing low intensity on T2WI may be diagnostic clues as “black rim sign” 5. Kozawa reported a case of the ovary, which showed slight high intensity on DWI with relatively high ADC (1.69 x 10-3 mm2/s), and concluded that DWI findings may contribute to the diagnosis 6. The purpose of this study is to evaluate the MR findings of polypoid endometriosis including DWI, DCE-MRI, and susceptibility-weighted MR sequences (SWS) for the differentiation from malignancy to avoid aggressive treatment.Methods
Five women (30 to 52 years of age, mean 41 years) with pathologically proven polypoid endometriosis who had undergone MRI examinations with 3-T (four cases) or 1.5-T (one case) superconducting MRI systems before surgery were retrospectively evaluated. Fast spin-echo T2WI and spin-echo or gradient-echo T1WI with/without fat-saturation (before and after the administration of gadolinium DTPA) are obtained in all five patients. DWI (b=800 to 1000 s/mm2) was obtained in four patients and ADC measurement was available in three patients. DCE-MRI was performed in four patients and SWS was obtained in two patients. Two radiologists qualitatively evaluated the images: signal intensity on T1WI (plain/CE), T2WI, and DWI; the presence of hemorrhagic foci (high intensity on T1WI and signal voids on SWS); the presence of pelvic endometriosis (low intensity fibrous adhesion on T2WI) and adenomyosis; the presence of “black rim sign” on T2WI; time-intensity curve pattern on DCE-MRI. The reviewers examined all images of the cases independently and then resolved discrepancies by consensus. The mean ADC values in three lesions obtained by 3-T scanner were measured in a circular ROI in one representative region from ADC maps generated by using b-values of 0 and 800 s/mm2 on the workstation (AW4.2).Results and Discussions
Two cases appeared as multiple polypoid masses with “black rim sign” in the peritoneal cavity (Douglas’ pouch) arising from pelvic endometriosis 5 (Fig. 1). Two cases were arising from endometriotic cysts with transmural extensions (one showed peritoneal extension with “black rim sign”, and the other showed prominent myometrial infiltration) (Fig. 2) and one case was arising from adenomyotic cyst. Co-existing pelvic endometriosis was observed in four lesions and adenomyosis was observed in all five lesions on T2WI. All five lesions showed high intensity on T2WI. High intensity hemorrhagic foci on T1WI were observed in three of five lesions. SWS were obtained in two lesions and signal voids reflecting hemorrhage were revealed in all two lesions (Fig. 3). In one of two lesions signal voids on SWS were more prominent than high intensity on T1WI, and in the other lesion hemorrhagic foci were revealed on SWS but not on T1WI. The presence of hemorrhagic foci may be associated with aberrant endometrial tissue with cyclic hemorrhage, and may be suggestive for its endometriotic nature. DWI was obtained in four lesions and all lesions showed high to slight high intensity. ADC measurement was available in three lesions and showed relatively high ADC values (1.57 to 1.77, mean 1.67 x 10-3 mm2/s), and the signal intensity was decreased on computed DWI with higher b values (b=2000) in all the three lesions. High signal intensity on DWI with high ADC value is considered to be due to T2 shine-through effect, and may contribute to differentiate polypoid endometriosis from malignant tumors 6, 7 (Fig. 4). On post-contrast T1WI, four lesions showed intense contrast-enhancement and the other one lesion showed weak contrast-enhancement. DCE-MRI was performed in four lesions and the time-intensity curve was gradually increasing pattern in all four lesions (Fig. 5). The lesion exhibiting weak contrast-enhancement histologically revealed as the admixture of benign to atypical hyperplasia and well-differentiated endometrioid carcinoma (malignant transformation of polypoid endometriosis), and weak contrast-enhancement pattern similar to that of endometrial carcinoma might be suggestive for the malignant transformation 8.Conclusion
We conclude that polypoid endometriosis may appear as solid pelvic masses with extension to the adjacent structures mimicking malignancy. “Black rim sign” may be suggestive for polypoid endometriosis arising from pelvic endometriosis. The presence of hemorrhagic foci revealed on SWS may be suggestive for its endometriotic nature, and relatively high ADC value may be suggestive for its benignity.Acknowledgements
No acknowledgement found.References
- Mostoufizadeh M, Scully RE. Malignant tumors arising in endometriosis. Clin Obstet Gynecol 1980;23:951-963.
- Parker RL, Dadmanesh F, Young RH, et al. Polypoid endometriosis: a clinicopathologic analysis of 24 cases and a review of the literature. Am J Surg Pathol 2004;28:285-297.
- Stewart CJ, Bharat C. Clinicopathological and immunohistological features of polypoid endometriosis. Histopathology 2016;68:398-404.
- Kwek JW, H'ng MW, Chew SH, et al. Florid polypoid endometriosis of the cervix with left ureteric obstruction: a mimic of cervical malignancy. Ultrasound Obstet Gynecol 2010;36:252-254.
- Takeuchi M, Matsuzaki K, Furumoto H, et al. Case report: a case of polypoid endometriosis: MR pathological correlation. Br J Radiol 2008;81:e118-119.
- Kozawa E, Inoue K, Iwasa N, et al. MR imaging of polypoid endometriosis of the ovary. Magn Reson Med Sci 2012;11:201-204.
- Davarpanah AH, Kambadakone A, Holalkere NS, et al. Diffusion MRI of uterine and ovarian masses: identifying the benign lesions. Abdom Radiol 2016;41:2466-2475.
- Takeuchi M, Matsuzaki K, Bando Y, et al. A case of polypoid endometriosis with malignant transformation. Abdom Radiol 2016;41:1699-1702.
Figures
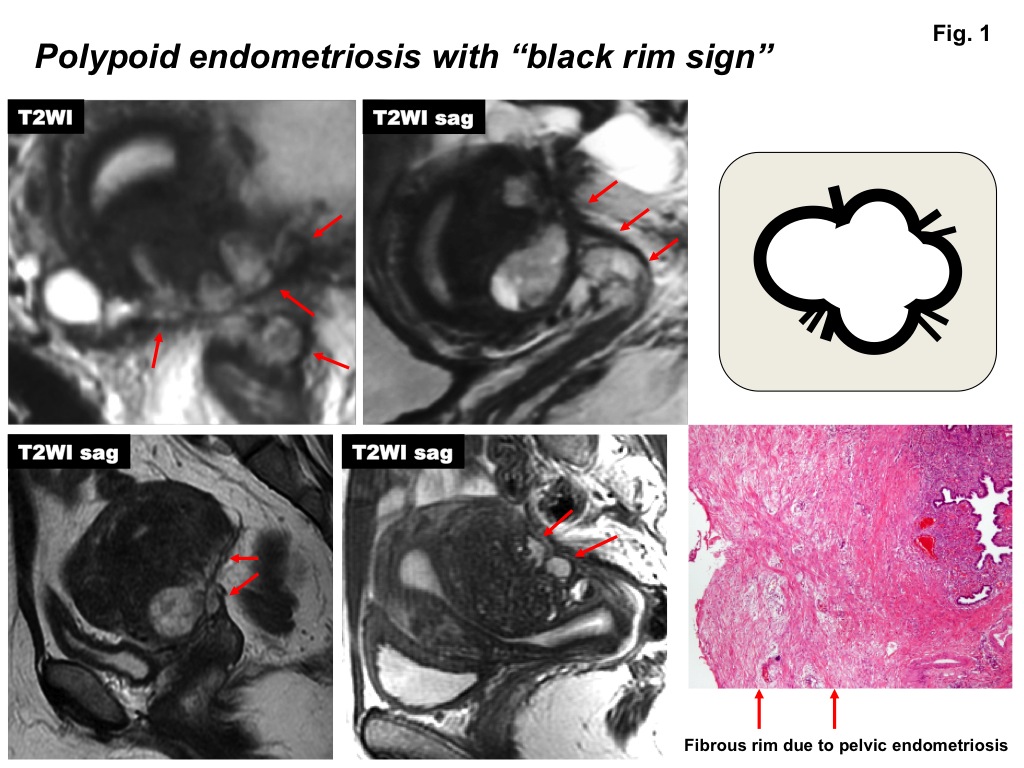
Polypoid endometriosis with pelvic endometriosis: Polypoid endometriosis arising from pelvic
endometriosis (upper row case and left case of lower row) show high intensity
masses on T2WI in the Douglas’ pouch surrounded by low intensity fibrous rim as
“black rim sign” (arrows). Polypoid endometriosis arising from endometriotic
cyst extending into the Douglas’ pouch with pelvic endometriosis (right case of
lower row) also shows “black rim sign” (arrows). Co-existing adenomyosis is
observed in all these cases.
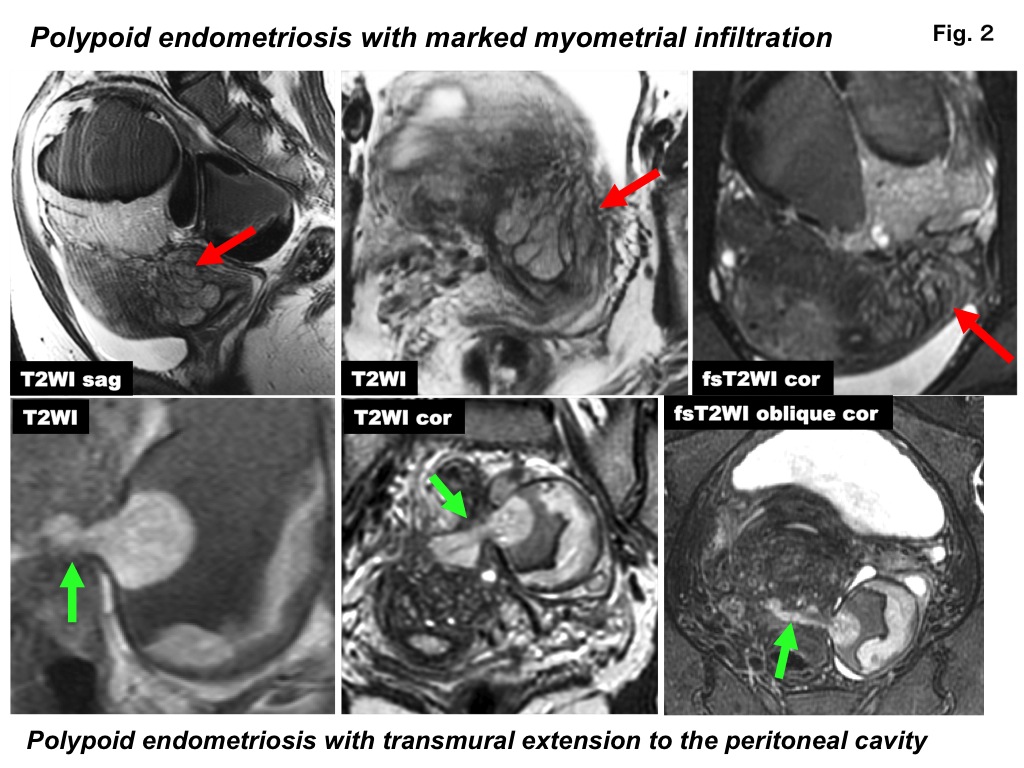
Polypoid endometriosis with local extension: Polypoid endometriosis arising from endometriotic
cyst (upper row) shows high intensity mass (arrow) on T2WI along the cyst wall
and prominent myometrial infiltration (arrow) mimicking low-grade endometrial stromal
sarcoma. Polypoid endometriosis arising from endometriotic cyst (lower row)
shows high intensity mural nodule on T2WI with transmural extension (arrow)
into the Douglas’ pouch and uterine serosa mimicking advanced ovarian cancer.
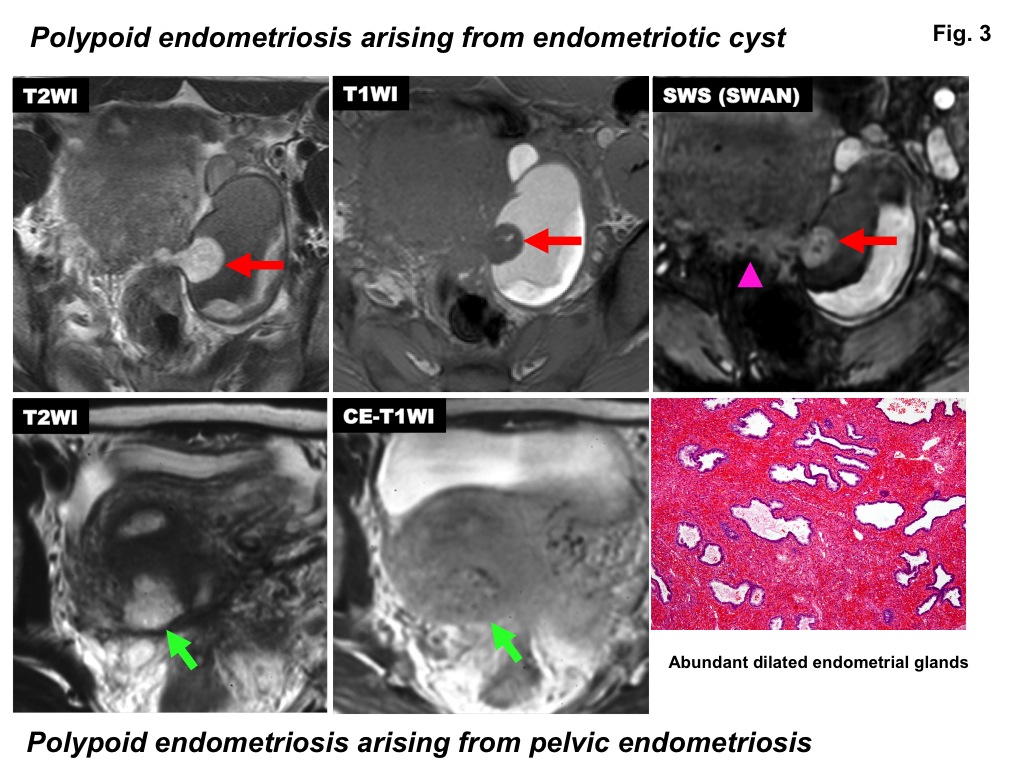
Signal intensity pattern of polypoid endometriosis: Polypoid endometriosis arising from
endometriotic cyst (upper row) shows high intensity mural nodule (arrow) on
T2WI, which contains hemorrhagic foci (high on T1WI and signal voids on SWS). SWS
also revealed hemorrhagic foci in the extending portion into the Douglas’ pouch
and uterine serosa (arrowhead). Polypoid endometriosis arising from pelvic
endometriosis (lower row) shows high intensity polypoid mass (arrow) on T2WI
and intense contrast enhancement on post-contrast T1WI.
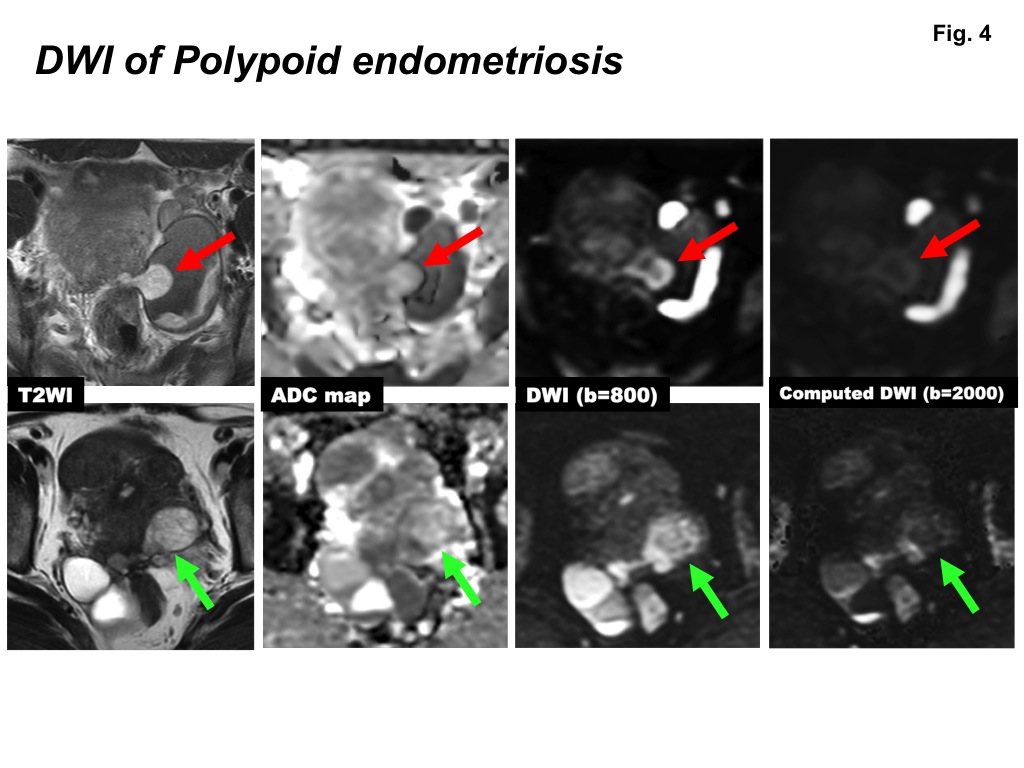
DWI of polypoid endometriosis: Polypoid endometriosis arising from
endometriotic cyst (upper row) and from pelvic endometriosis (lower row) show
high intensity masses (arrows) on T2WI and DWI (b=800 s/mm2) with
relatively high ADC values (1.66 and 1.77 x 10-3 mm2/s,
respectively). The signal of the masses is decreased on high b-value (b=2000
s/mm2) computed DWI.
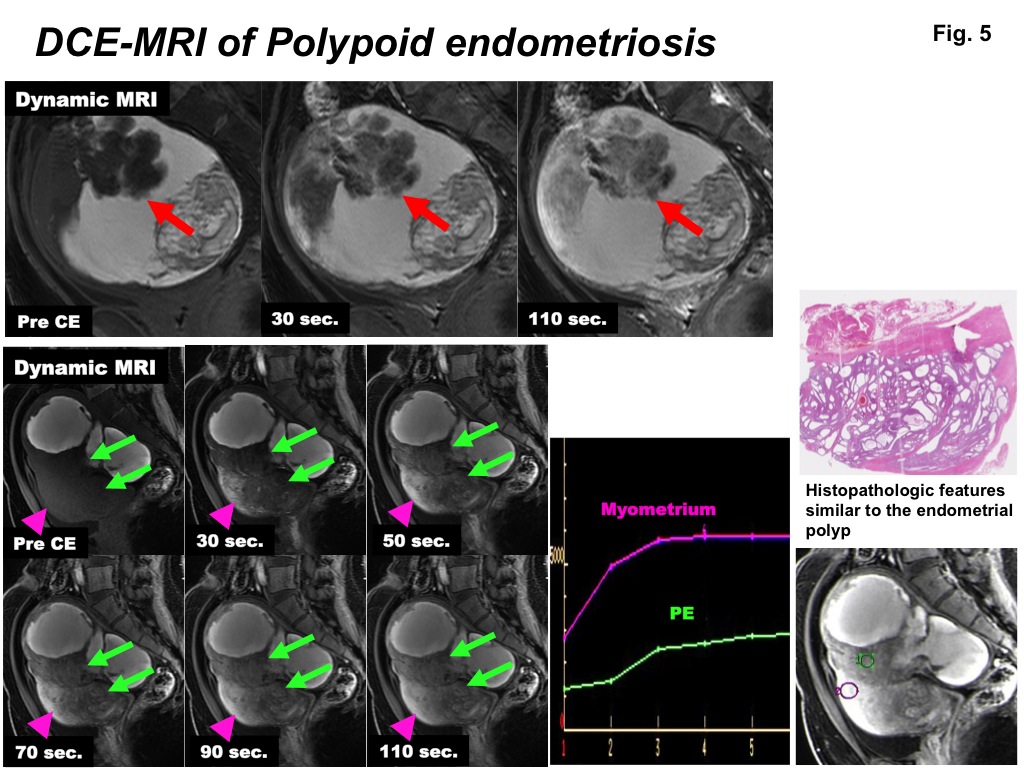
DCE-MRI of polypoid endometriosis: Polypoid endometriosis arising from adenomyotic
cyst (upper row) and from endometriotic cyst with myometrial infiltration
(lower row) show gradually increasing pattern on DCE-MRI.