4031
Comparison of SENSE-accelerated PROPELLER and Single-shot Turbo Spin-Echo Sequences for Visualization of the Prostatic Urethra during MRI-based Radiotherapy Treatment Planning1Medical Physics, Memorial Sloan Kettering Cancer Center, New York, NY, United States, 2Radiology, Memorial Sloan Kettering Cancer Center, New York, NY, United States, 3Philips Medical Systems, Best, Netherlands, 4Radiation Oncology, Memorial Sloan Kettering Cancer Center, New York, NY, United States
Synopsis
At our institution, a Foley catheter is inserted during prostate SBRT simulation to ensure visualization of the prostatic urethra. Our goal was to find an optimal motion-robust T2-weighted pulse sequence that would allow for accurate catheter-free visualization and segmentation of the urethra. We compared Multivane XD (MVXD), a PROPELLER-based multislice TSE sequence with SENSE acceleration to single-shot TSE with SENSE (SSTSE). Two expert GU radiologists scored urethra visibility in MVXD and SSTSE series of equivalent spatial resolution and duration. Urethra visibility scores were significantly higher in the MVXD series and SNR was found to be superior in all MVXD series.
Introduction
High radiation doses employed for prostate radiotherapy can result in urethral side effects. Stereotactic body radiation therapy (SBRT) employs very high radiation doses in limited fractions and may further increase the probability of urethral toxicity1. At our institution, a Foley catheter is inserted during the simulation process for prostate SBRT patients to ensure visualization of the prostatic urethra for contouring. However, catheterization is particularly unpleasant for patients. Our goal was to find an optimal motion-robust T2-weighted pulse sequence that would allow for accurate catheter-free visualization and segmentation of the urethra. While isotropic T2-weighted 3D-MRI is excellent for high-resolution soft tissue differentiation, artifacts in two dimensions due to respiration, bladder and bowel motion can obscure the urethra. Therefore, we compared Multivane XD (MVXD), a 2D multislice radial fast-spin-echo sequence based on PROPELLER2 where SENSE3 parallel imaging acceleration is incorporated within each blade to single-shot turbo spin echo with SENSE (SSTSE).Methods
All scans were performed on a 3T Philips Ingenia (Philips, Best, The Netherlands) equipped with a flat tabletop for MR simulation. Twelve prostate cancer patients underwent MRI as part of simulation for conventionally fractionated or moderately hypofractionated prostate radiotherapy. Our standard procedure is to require Foley catheterization for patients undergoing ultra-hypofractionated therapy while urethral location for patients treated with other fractionations is estimated using other anatomical features.
Standard imaging series include large FOV 3D Dixon-based T1-weighted gradient-echo, small FOV multislice axial T2 fast-spin-echo, and sagittal multislice fast spin echo or 3D balanced fast field echo (bFFE). As patients are scanned with a full bladder, exam time must be limited and the MVXD and SSTSE sequences were optimized to provide sub-millimeter in-plane resolution and adequate SNR in 2-3 minutes. Parameters common to both sequences were: FOV = 220 mm2-300 mm2, in-plane resolution = 0.9x0.9 mm2, slice thickness = 2.5 mm, TR = 3500 ms, TEeff = 80 ms. MVXD parameters included: 35 echoes per shot/blade, 1 average, percent of Cartesian sampling = 220, SENSE factor = 1.8. SSTSE parameters included echo train length 79-96 and SENSE factor = 2.0. Two-averages were used for the SSTSE to provide comparable SNR compared to MVXD. Two radiologists with GU experience > 10 years and > 5 years assessed the MVXD and SSTSE series. A 1-5 scale was used to score visibility of the prostatic urethra where 1 = urethra not visible and 5 = urethra completely visible. In addition, readers were asked to comment on signal-to-noise ratio and the presence of artifacts.
Results
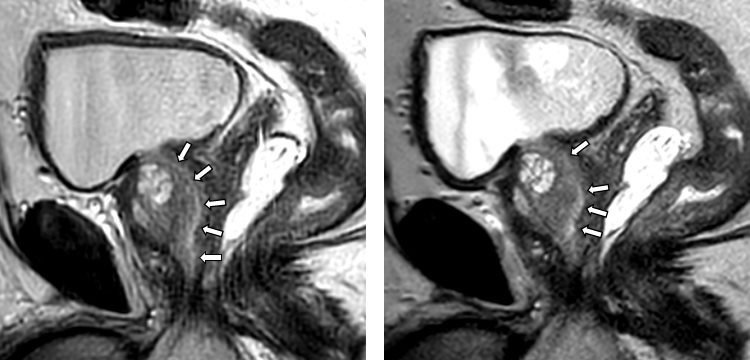
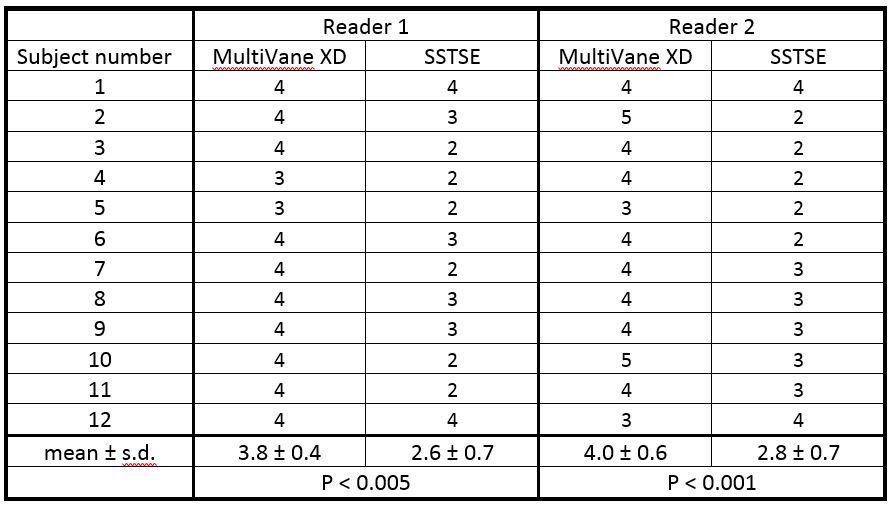
Figure 1 contains MVXD and SSTSE series for subject 2. Both readers gave MVXD a higher urethral visibility score than SSTSE (4 vs. 3 and 5 vs. 2). As seen in Table 1, both readers scored urethra visibility higher in MVXD images than in SSTSE images in 10/12 subjects. In the remaining 2 subjects, urethral visibility was good (score ≥3) for either method as ranked by both readers. SSTSE was rated slightly superior (4 vs 3) in 1 case (Reader 2). Using a paired Student’s t-test for comparison, urethra visibility scores were significantly higher in the MVXD series (See table). Qualitatively, both readers rated MVXD as having superior SNR in all patients. Readers noted streak artifacts in 7/12 and 6/12 MVXD data sets, respectively; however, these were near the periphery and did not interfere with urethra visualization. No artifacts were noted in the SSTSE images. Despite identical effective echo times, the different sampling schemes resulted in subtle differences in T2 contrast; this did not affect urethra visualization.Discussion
Single shot fast spin-echo is widely used for motion-insensitive T2-weighted imaging, but can be SNR-limited. We found that two averaged single-shot TSE acquisitions were needed to achieve sufficient SNR and spatial resolution, increasing the potential for between-shot motion. Optimized Multivane XD provided superior urethra visualization in 10 of 12 cases. Limiting scan time to 2-3 minutes and incorporating SENSE acceleration of 1.8 permitted sampling of 220% over conventional Cartesian k-space, mitigating streaking artifacts and providing superior SNR. In this patient group, motion artifacts were not observed in either series suggesting that the SNR advantage of MVXD was the source of enhanced urethra visibility.Conclusions
Mutlivane XD, a PROPELLER-based pulse sequence with SENSE encoding, provided superior visibility of the prostatic urethra over a single-shot TSE sequence of equivalent resolution and duration. At our institution, Multivane XD has been incorporated into the MR-only simulation workflow for the prostate, and elimination of the Foley catheter is being studied.Acknowledgements
The authors would like to thank the MRI technologists and therapists in the MSKCC Department of Radiation Oncology for their valuable assistance.References
1. Repka, MC, Guleria, S. et. al. Acute Urinary Morbidity Following Stereotactic Body Radiation Therapy for Prostate Cancer with Prophylactic Alpha-Adrenergic Antagonist and Urethral Dose Reduction. Front Oncol 2016 May 18; 6:122.
2. Pipe, JG. Motion correction with PROPELLER MRI: application to head motion and free-breathing cardiac imaging. Magn Reson Med 1999 Nov;42(5):963-9.
3. Pruessmann, KP, Weiger, M., et. al. SENSE: Sensitivity Encoding for Fast MRI. Magn Reson Med 1999 Nov; 42(5): 952-962.
Figures