3972
Repeatability and Clinical Performance of Non-gated, Free-breathing, MR Elastography (MRE) of the Liver1Radiology, Mayo Clinic, Rochester, MN, United States, 2Gastroenterology, Mayo Clinic, Rochester, MN, United States
Synopsis
While conventional MRE is easily performed during suspended respiration, a free breathing MRE technique would be advantageous in pediatric and other patients. We assessed the repeatability of free-breathing MRE in comparison to conventional breath held acquisitions in volunteers and the clinical performance of free-breathing MRE in a cohort of 56 patients with chronic liver diseases. Results demonstrated comparable repeatability and excellent agreement of the averaged liver stiffnesses measured using the two techniques. In summary, free-breathing MRE provides highly repeatable and accurate liver stiffness values.
Introduction
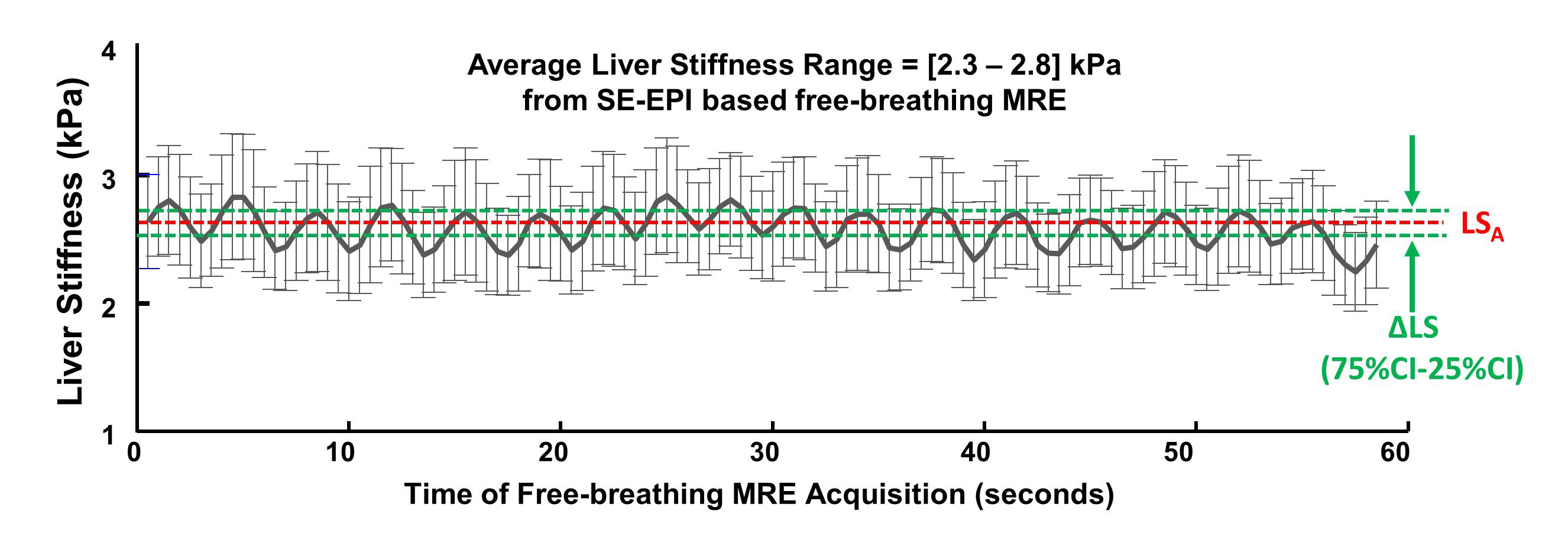
Liver MR elastography (MRE), a quantitative imaging method for noninvasively assessing hepatic fibrosis, is conventionally performed using a breath-held, multi-slice, 2D, spin-echo echo-planar imaging (SE-EPI) or gradient-recalled echo (GRE) acquisition1. Both SE-EPI and GRE MRE are performed using expiration breath holds to avoid respiratory motion artifacts in the images and because end-expiration is considered a more reproducible breath-hold location than end-inspiration. However, some patients have difficulty performing adequate end-expiration breath holds (e.g., pediatric and sedated patients). Preliminary studies have demonstrated that a non-gated, free-breathing, single-shot, multi-slice 2D EPI-MRE technique with a view-sharing-based reconstruction strategy can eliminate the need for breath holds2 and is capable of using the respiratory cycle to measure liver stiffness and other third-order mechanical parameters that may be helpful in disease diagnosis3. The purpose of this study is to evaluate the test-retest repeatability of this rapid, free-breathing MRE technique and to assess the accuracy of the liver stiffness measurements compared to conventional breath-held MRE.Methods
All activities related to human subjects were reviewed and approved by our institutional review board. Six patients and one healthy volunteer underwent test-retest scans to evaluate the repeatability of free-breathing MRE. The exam consisted of a breath-held 2D SE-EPI MRE scan, a free-breathing 2D SE-EPI MRE scan, and a conventional Dixon acquisition for hepatic fat quantification. The exam was performed and then the subject was removed from the scan room, repositioned, and rescanned approximately 15 minutes later. The same data were collected in another cohort of 56 patients with chronic liver disease without the retest scan to evaluate the clinical performance of free-breathing MRE. The examinations were carried out on multiple whole-body GE 1.5T scanners (Excite HDxt and Optima MR 450w; GE Healthcare, Waukesha, WI). In this implementation of free-breathing MRE, a 4-offset MRE data set was collected every 4 seconds and repeated 25 times (~1.5 min acquisition time), allowing for a view-shared reconstruction of 100 liver stiffness images over ~20-30 respiratory cycles. We calculated the baseline liver stiffness (LSB) from the conventional breath-held MRE stiffness images, and the average liver stiffness (LSA) and stiffness variation ΔLS (ΔLS=75%-25% quantiles) from the 100 free-breathing stiffness images, within anatomically co-registered ROIs (Figure 1). The repeatability coefficients (RC)4 and intra-class correlation coefficients (ICC) were used to analyze the test-retest repeatability of breath-held and free-breathing MRE. Spearman correlations were used to evaluate the relationships between LSB and LSA, fat fraction, and ΔLS. We also classified the patients into two groups, one group with fatty liver disease and the other group with other chronic liver diseases (alcoholic hepatitis, cirrhosis, primary sclerosing cholangitis, etc.). For all statistical analysis, a significance level of less than 0.05 was used and a correlation coefficient (ρ) greater than 0.90 was considered excellent.Results
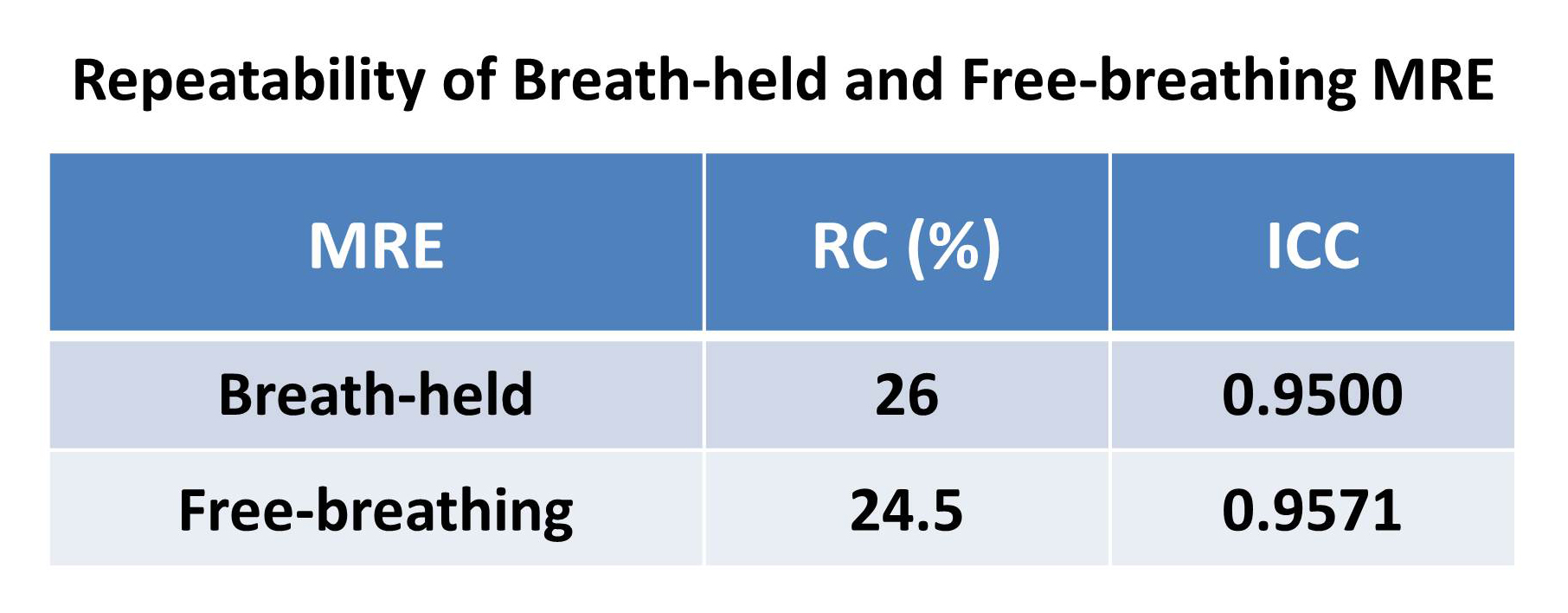
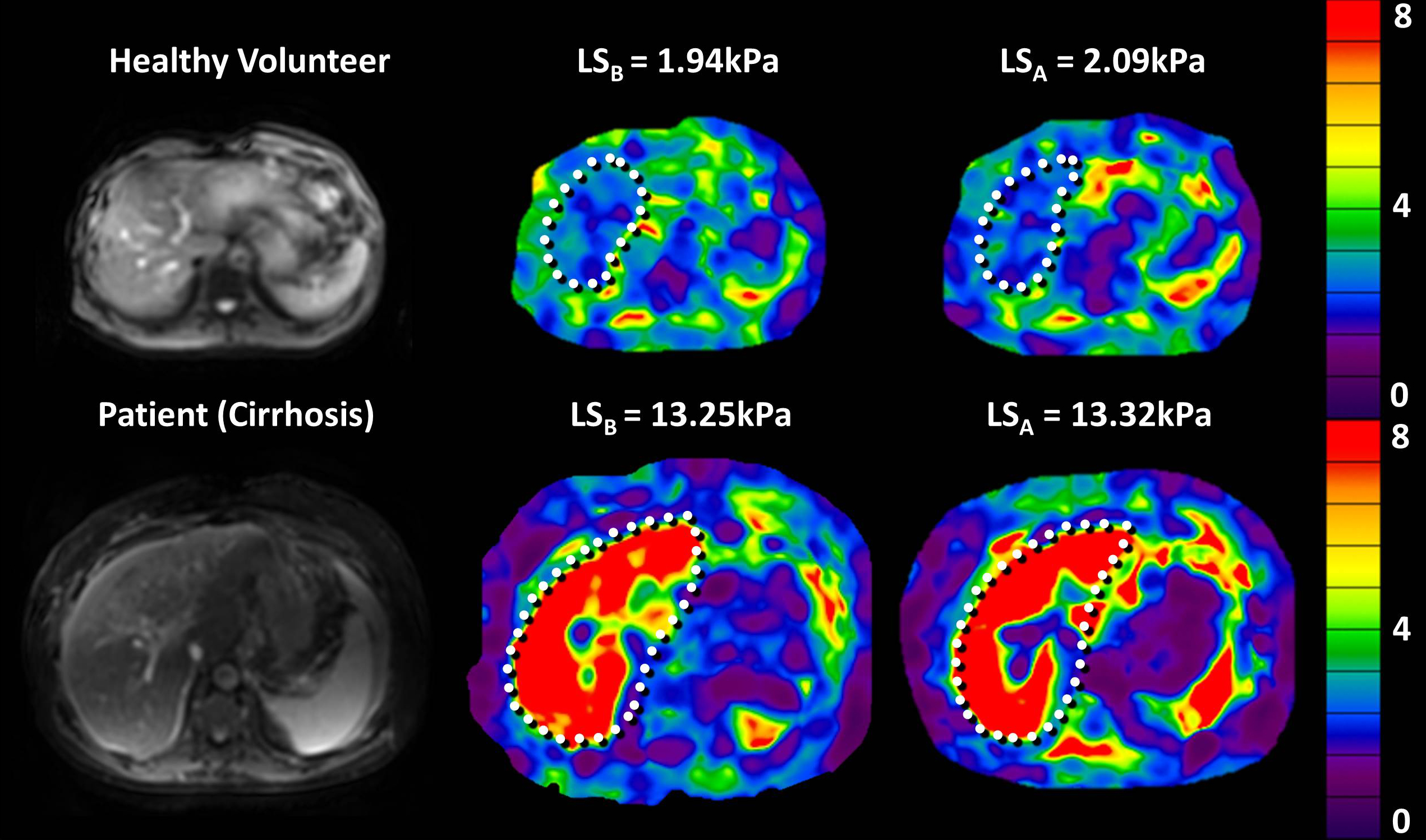
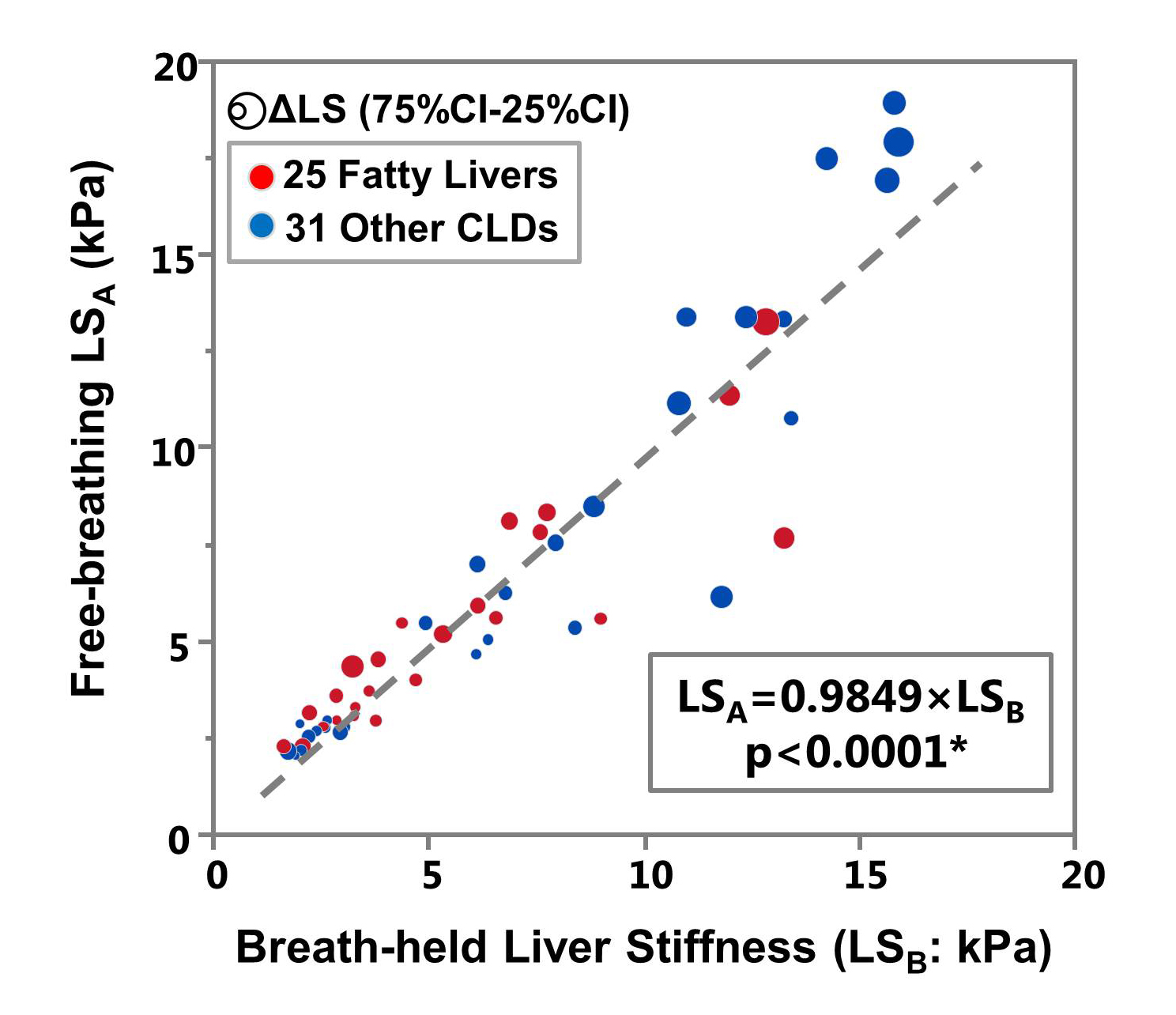
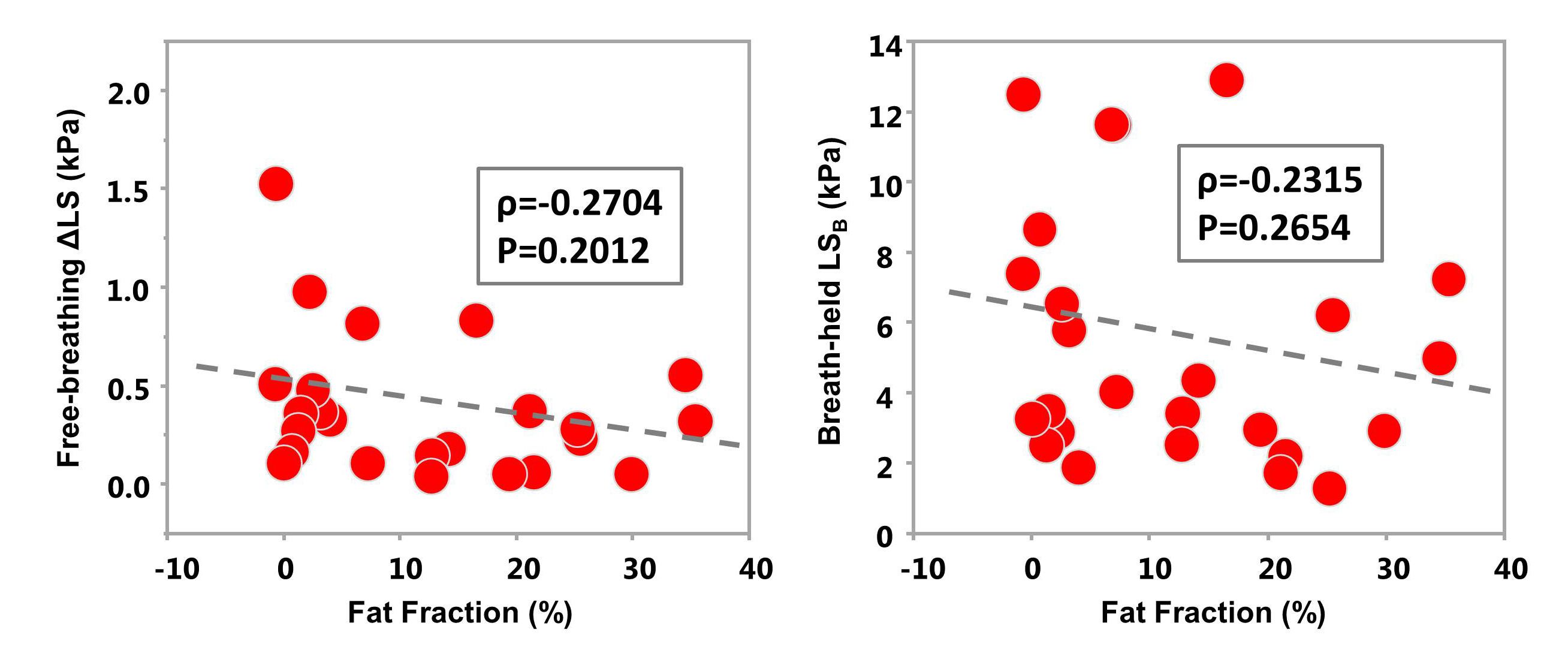
Table 1 illustrates that the RC of free-breathing MRE (24.5%) is comparable with that of breath-held MRE (26%). The ICC of free-breathing MRE (0.9571) is also comparable with that of breath-held MRE (0.9500). Figure 2 shows example images of a healthy volunteer and a patient. With Spearman’s correlation analysis, we found that LSA excellently agrees with LSB (LSA=0.9849×LSB, ρ=0.9562, p<0.0001*)( Figure 3). Figure 4 illustrates that there is no significant correlation between fat fraction and ΔLS or LSB in the 25 patients with fatty liver disease.Discussion
The RC is a percentage of the measured hepatic stiffness change and indicates that a measured change larger than that can be considered a true change with 95% confidence. The RC of 2D MRE in healthy volunteers from QIBA is 19%4, while in another study in 94 patients it was 25.3%5. In our study, the RC calculated from free-breathing MRE (24.5%) was similar to breath-held MRE (26%) and was similar to these other studies. This suggests that different breath-held position could be a substantial source of measurement variation in breath-held MRE. Free-breathing MRE has potentials to mitigate this variation if calculating LS at different respiratory states. The LSA calculated from free-breathing MRE excellently agrees with LSB from conventional breath-held MRE in patients. The stiffness variation across the breathing cycle, ΔLS, did not appear to be related to stiffness or hepatic fat fraction. Additional studies are required to determine if this variation may be another promising parameter for patient assessment.Conclusion
Free-breathing MRE has comparable repeatability to conventional breath-held MRE. It also provides an accurate averaged liver stiffness measurement that has potential for the assessment of patients with chronic liver diseases. This technique will be very beneficial for pediatric and sedated patients and could improve the comfort and patient experience for the general population as well.Acknowledgements
This study is funded by NIH grant EB017197, EB001981, and Mayo Clinic Center for Individualized Medicine Imaging Biomarker Discovery Program.References
1. Yong Seek Kim, Yu Na Jang, Ji Soo Song. Comparison of gradient-recalled echo and spin-echo echo-planar imaging MR elastography in staging liver fibrosis: a meta-analysis. Eur Radiol. 2018;28:1709-1718.
2. Glaser K, Chen J, Ehman R. Fast 2D hepatic MR elastography for free-breathing and short breath hold applications. The 23rd Annual Meeting of International Society of Magnetic Resonance in Medicine (ISMRM); May; Toronto, Ontario, Canada 2015. p. 6579.
3. Ziying Yin, Bogdan Dzyubak, Jiahui Li, Kevin J. Glaser, Sudhakar K. Venkatesh, Armando Manduca, Richard L. Ehman, Meng Yin. A Feasibility Study of Nonlinear Mechanical Response Assessment of the Liver with MR Elastography (MRE). The 26rd Annual Meeting of International Society of Magnetic Resonance in Medicine (ISMRM); June; Paris, France 2018. p.0606.
4. QIBA MR Elastography Biomarker Committee. MR Elastography of the Liver, Quantitative Imaging Biomarkers Alliance. Profile Stage: Consensus. QIBA, May 2, 2018. Available from: http://qibawiki.rsna.org/index.php/Profiles
5. Ye ji lee, Jeong Min Lee, Jeong Eun Lee, et al. MR Elastography for Noninvasive Assessment of Hepatic Fibrosis: Reproducibility of the Examination and Reproducibility and Repeatability of the Liver Stiffness Value Measurement. Journal of Magnetic Resonance Imaging. 2014;39:326-331
Figures