3964
In Vivo Cardiac MR Elastography with a Gravitational Transducer1Division of Imaging Sciences and Biomedical Engineering, King’s College London, London, United Kingdom, 2Philips Healthcare, Guildford, Surrey, United Kingdom, 3Amsterdam UMC, Amsterdam, Netherlands, 4Guy's and St.Thomas' NHS Foundation Trust, London, United Kingdom, 5Department of Biomedical Engineering and Cardiac Surgery, University of Michigan, Ann Arbor, MI, United States
Synopsis
MR Elastography is beneficial in measuring the
stiffness values of tissues which can change in disease. Nevertheless, cardiac MR
Elastography is not only challenging from the acquisition side but also from
the reconstruction side because of the higher stiffness values expected in the
cardiac muscle compared to the other organs in which MR Elastography is commonly
applied. Here, we present data in healthy subjects and a patient acquired with
the gravitational transducer with a novel synchronising strategy in combination
with a single-shot SE-EPI-MRE sequence employing second-order motion
compensated motion encoding gradients with and without ZOnal Oblique Multislice
Imaging.
INTRODUCTION
MR Elastography (MRE) is a technique to evaluate the biomechanical properties of soft tissues noninvasively in vivo. Diseases often fundamentally alter these biomechanical properties, making MRE a valuable technique for diagnosis and staging of disease. Despite the value of MRE detecting potential pathological tissues, applications of this technology in the heart have been limited due to several factors, including hardware, hardware/scanner interfacing, robust MR sequences and reconstruction strategies suitable for reconstructing the long wavelengths observed in the myocardium. The purpose of this study was to acquire cardiac MRE data using a gravitational transducer with a new synchronisation strategy in combination with a single-shot SE-EPI-MRE sequence employing second-order motion compensated MRE motion encoding gradients (MEGs) with and without ZOnal Oblique Multislice (ZOOM)1 imaging. We also introduce a novel reconstruction technique to estimate stiffness and to reconstruct the data acquired from healthy volunteers and a representative patient case.METHODS
Hardware: The MRE gravitational transducer concept2 was used to produce shear waves where the transducer runs continuously to maintain the periodic steady-state of the waves. The previous need for external hardware to achieve the synchronization3 has been mostly eliminated by pulse sequence modifications to measure the exact ECG detection time point and delay the excitation accordingly to synchronise the sequence with the transducer. An Arduino UNO is used to send periodic triggers to the transducer to ensure its correct position.
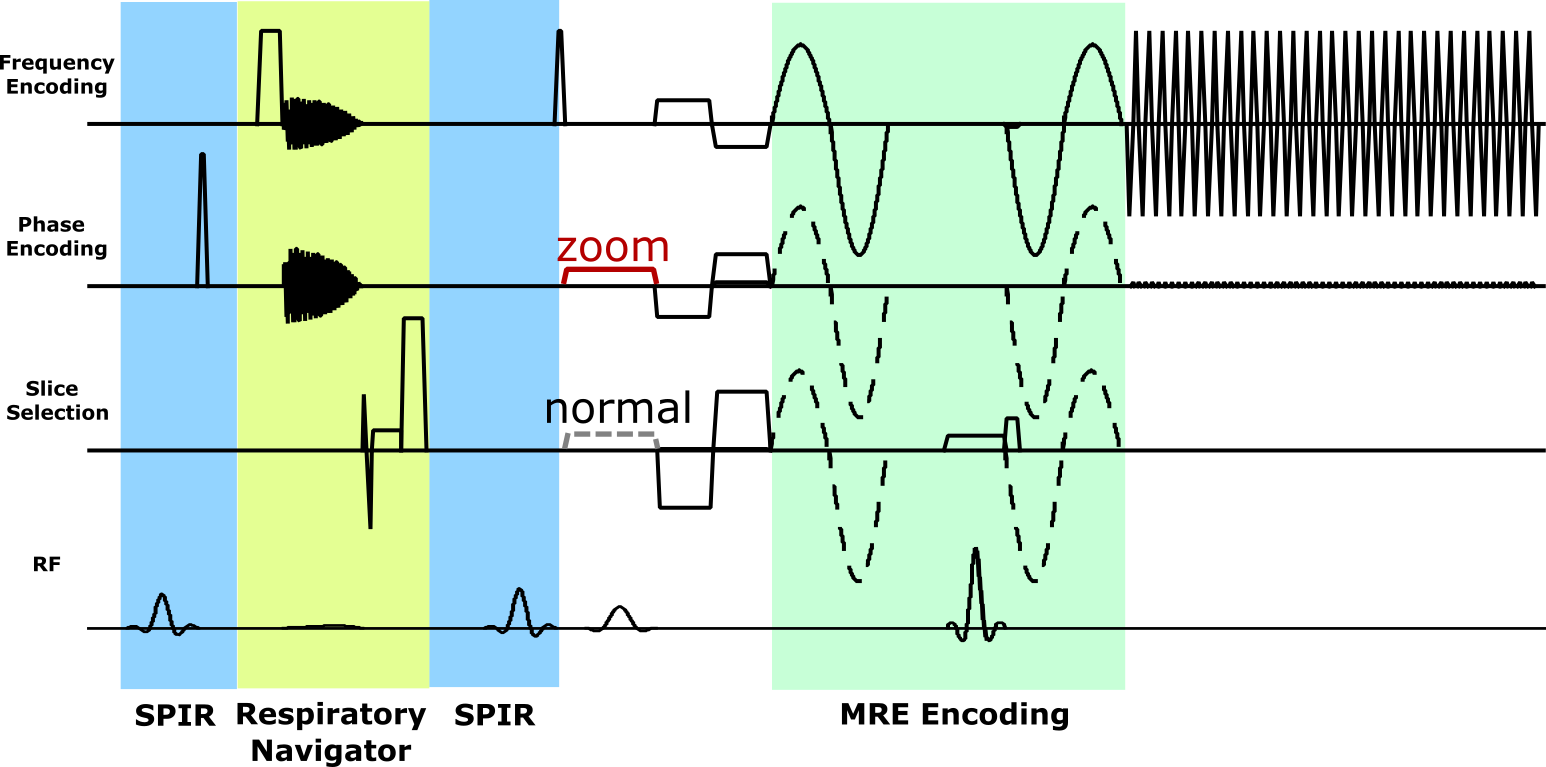
MR Sequence: A cardiac-triggered single-shot SE-EPI sequence, similar to the study4 but with flow and acceleration compensated MEGs, was implemented as shown in Fig.1 with and without ZOOM imaging options. In addition to the delay in the sequence providing synchronization with the transducer, gradually increasing delays were used to achieve different mechanical wave phases.
MR Measurements: Measurements were performed on a 3T Achieva MR scanner (Philips Healthcare, The Netherlands) in breath-hold with imaging parameters: TR=RR; TE = 60ms/76ms with/without ZOOM for a 2x2x4mm3 voxel; SENSE factor = 2; ETL = 31/63 with/without ZOOM. 3 slices were acquired from 3 healthy volunteers (1 female) and a representative patient case at 80Hz MRE vibration frequency where one of the healthy volunteers was scanned for reproducibility on different days with both options of the sequence. Data were acquired with MEGs applied in slice selection, phase encoding, and readout directions including a reference scan without MEGs.
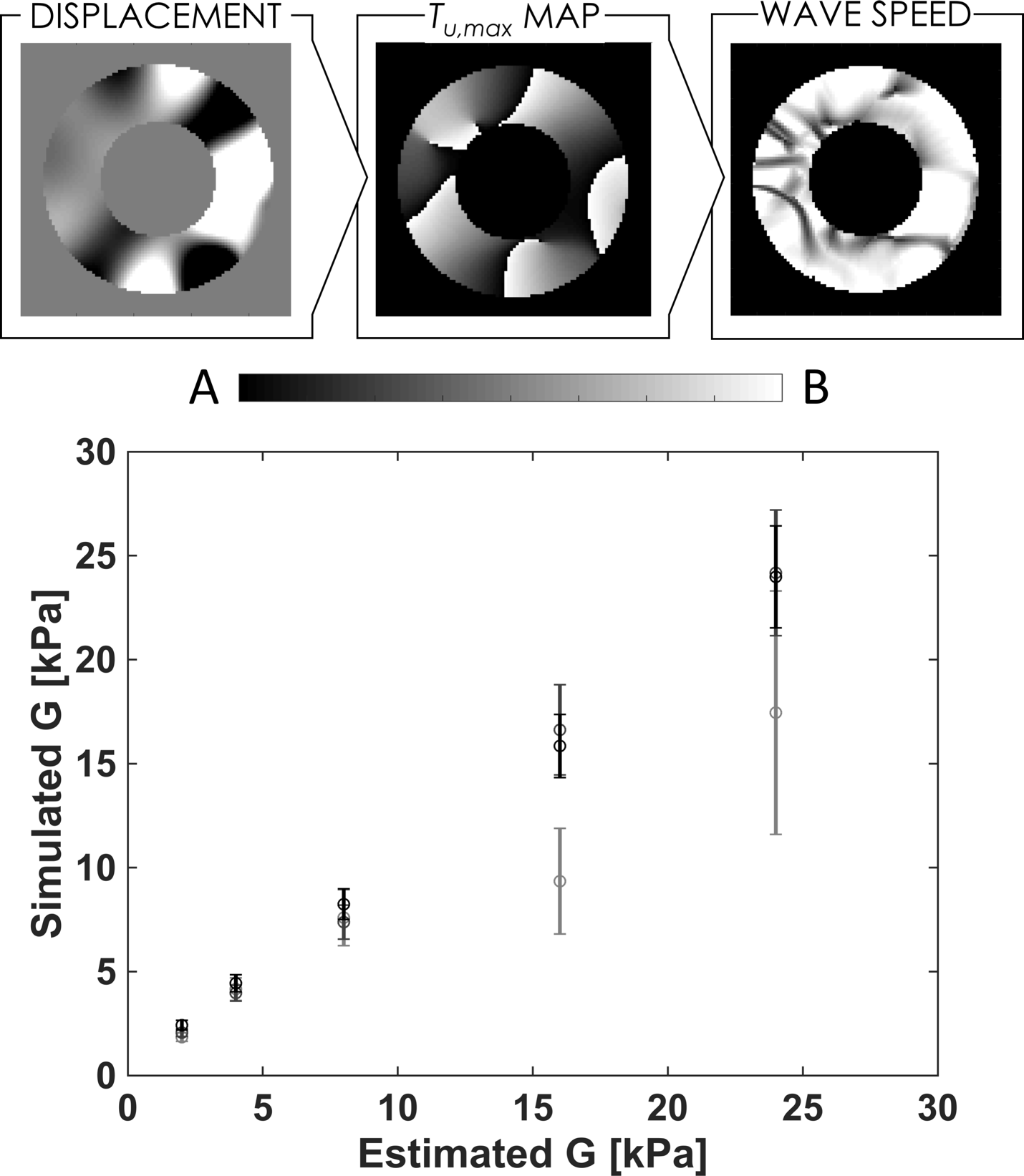
MRE Reconstruction: Measurements from cardiac MRE present challenges for traditional reconstruction algorithms due to the data quality, limited number of available pixels transmurally, and long wavelengths. To overcome these challenges, we introduce a new method which estimates speed by computing the time to max displacement and performing an inversion (see Figure 2, top). To validate the method, we compared in simulated viscoelastic cylinders with varying frequency and stiffnesses, demonstrating efficacy of the estimate for sufficiently high vibration frequency (see Figure 2, bottom).
RESULTS AND DISCUSSION
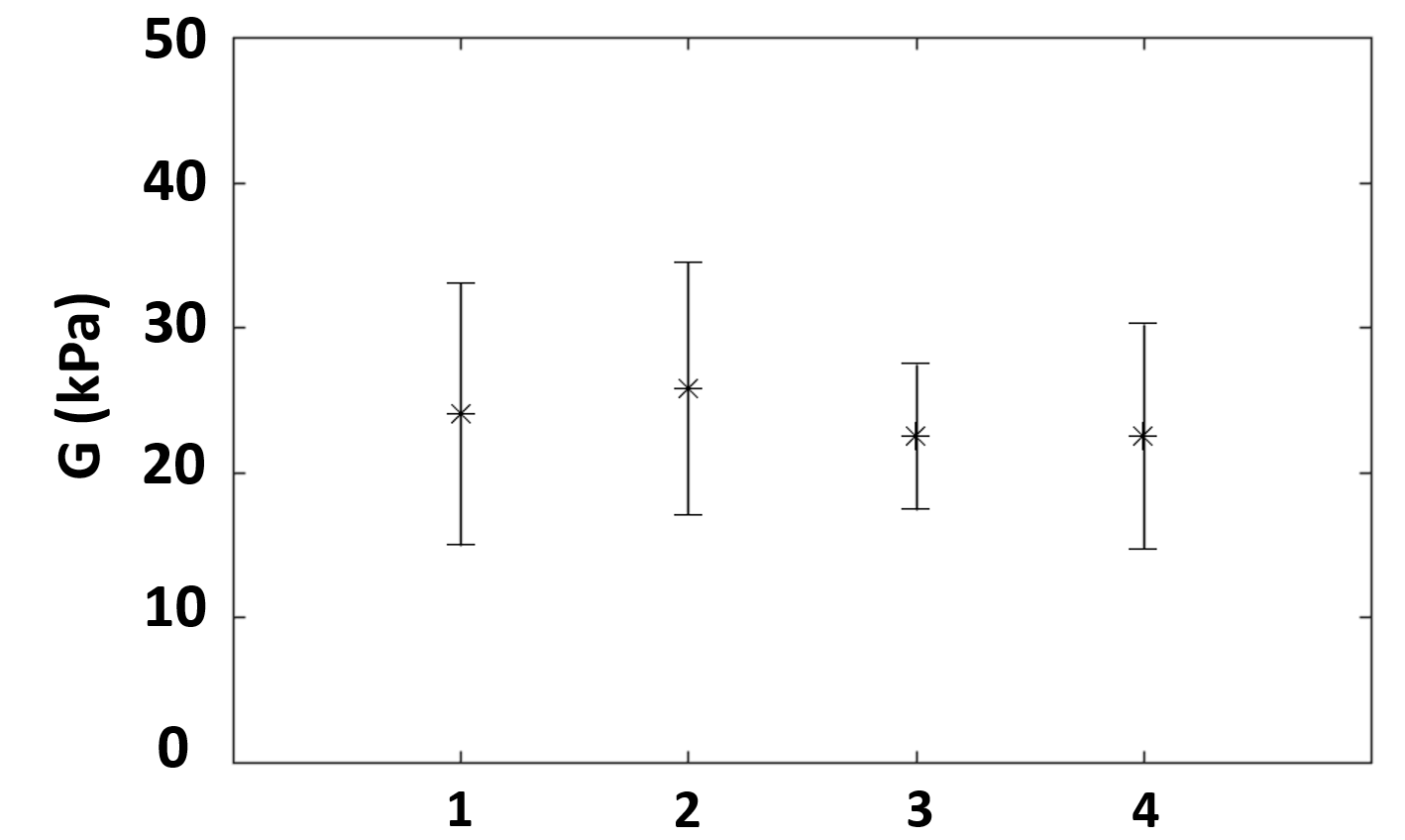
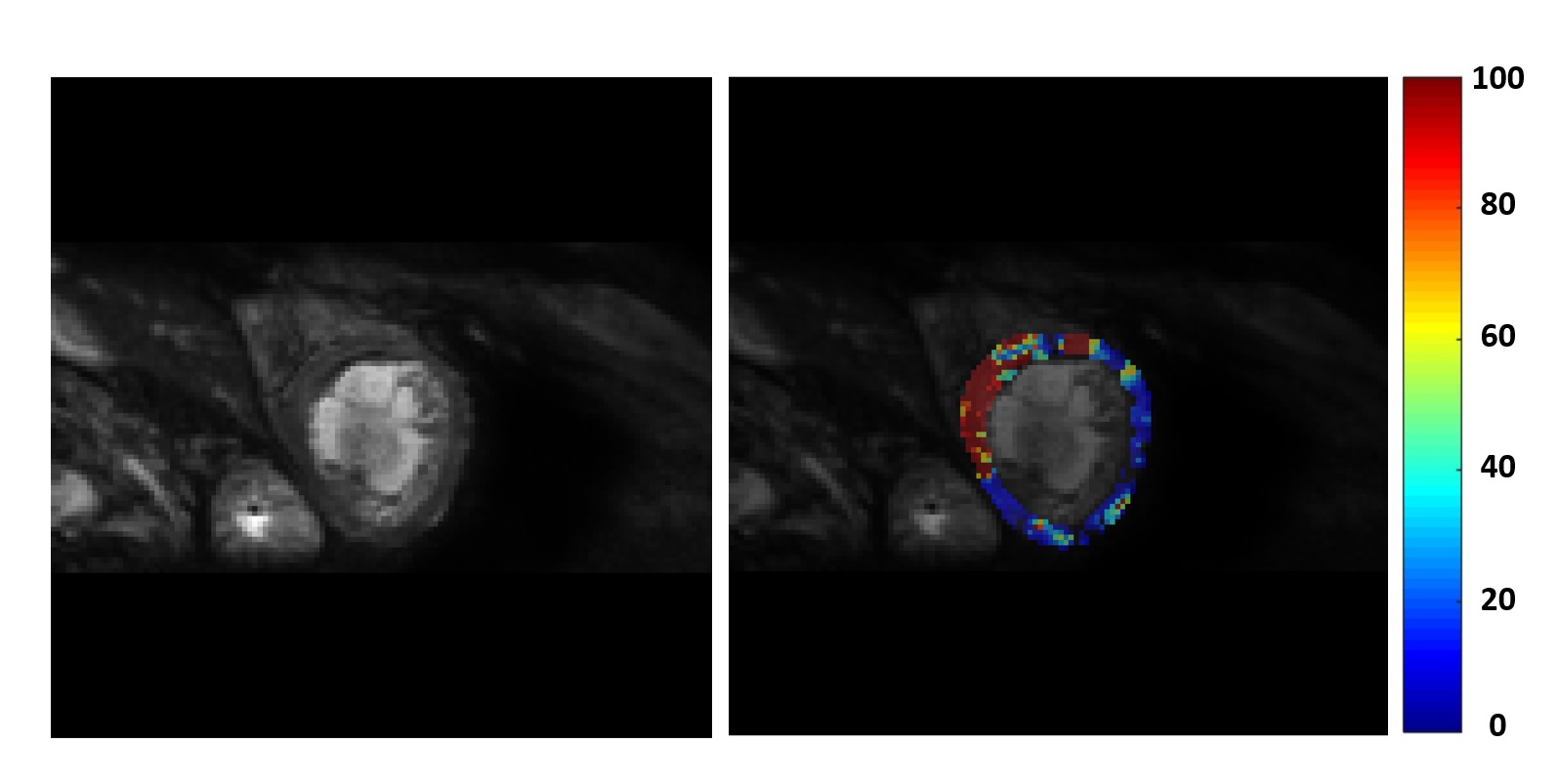
Figure 3 shows the results demonstrating reproducibility of the measurements for a healthy volunteer in diastole. On two days the sequence was repeated both with and without the ZOOM options. ZOOM imaging was the preferred method for subjects needing bigger FOVs and both sequences provided similar stiffness values. In addition to the similar results between the sequences, scans on two different days resulted in similar stiffness values demonstrating the reproducibility of the acquisition methods. For the patient data, clinical scans showed scar tissue in the left ventricular septal and anterior walls which was in agreement with the increased stiffness values in the septum from the representative patient data as seen in figure 4.CONCLUSION
We extended our previous work3 by improving the MR sequence and the hardware design to acquire minimal additional hardware as well as implementing a novel reconstruction algorithm which is more suited to the nature of the long wavelengths expected in the myocardium. We showed reproducibility of the sequence in a healthy volunteer and applied the method in a patient as well where high stiffness corresponded to a known scar location. The sequence provides good quality images in a reasonable breath hold time for patients. The reconstruction can potentially provide higher accuracy spatial maps of stiffness as indicated in the patient case.Acknowledgements
Authors would like to acknowledge funding from the EPSRC (EP/N011554/1 and EP/R0037866/1)References
1. Feinberg DA, Hoenninger JC, Crooks LE, Kaufman L, Watts JC, Arakawa M. Inner Volume MR Imaging: Technical Concepts and Their Application. Radiology. 1985; 156:743-747.
2. Runge J, Hoelzl S, Sudakova J, Dokumaci AS, Nelissen JL, Lee J, Stoker J, Nederveen AJ, Nordsletten D, Sinkus R. A Novel MR Elastography Transducer Concept Based on a Rotational Eccentric Mass: The Gravitational Transducer. In: Intl. Soc. Mag. Reson. Med. 25. Vol 1369. Honolulu; 2017.
3. Dokumaci AS, Schneider T, Hadjicharalambous M, Hoelzl S, Sudakova J, Hollands D, Sinkus R, Nordsletten DA. In Vivo Cardiac MR Elastography Using a Gravitational Transducer. In: Intl. Soc. Mag. Reson. Med. 26. Vol 5585. Paris; 2018.
4. Arani A, Arunachalam SP, Chang ICY, Baffour F, Rossmann PJ, Glaser KJ, Trzasko JD, McGee KP, Manduca A, Grogan M, Dispenzieri A, Ehman RL, Araoz PA. Cardiac MR Elastography for Quantitative Assessment of Elevated Myocardial Stiffness in Cardiac Amyloidosis. J Magn Reson Imaging. 2017;46(5):1361-1367.
Figures