3949
Optimization of Simultaneous Multi-slice Imaging with Autocalibrating Reconstruction for Cartesian Imaging Parameters for Human Connectome Type Protocol1Radiology, Medical College of Wisconsin, Milwaukee, WI, United States, 2Center for Imaging Research, Medical College of Wisconsin, Milwaukee, WI, United States, 3Neurosurgery, Medical College of Wisconsin, Milwaukee, WI, United States, 4GE Healthcare, Waukesha, WI, United States
Synopsis
The optimal parameterization of simultaneous multi-slice (SMS) unaliasing kernel fitting with autocalibrating reconstruction for cartesian imaging (ARC) is not obvious. Here we systematically varied five variables that parameterize this calibration process to empirically determine optimal values for human connectome project (HCP) harmonized image reconstruction. Low levels of regularization, moderate sizes of ky-kernels, and increased numbers of ky-calibration points yield improved unaliasing performance.
Introduction
Simultaneous multi-slice (SMS) excitation has become ubiquitous in echo-planar imaging for increasing slice coverage efficiency. This work presents a systematic investigation into design choices for a data-driven SMS reconstruction. In the calibration step of parallel imaging, an optimization problem is solved in which fully sampled data are fit as a function of sparsely sampled data. In synthesis, the optimized fit is applied to sparsely sampled data to generate data which is similar to fully sampled data. This work focuses upon SMS image reconstruction using the autocalibrating reconstruction for cartesian imaging1 (ARC) method of parallel imaging2. Specifically, the resulting image synthesis is evaluated based upon the systematic modulation of the ARC kernel size, the data used for calibration, and regularization of the fit.Methods
SMS acquisitions, based upon the HCP imaging protocol3, were performed on a GE Healthcare Discovery MR750 with a Nova Medical 32-channel receive only head coil. Imaging parameters included: TE 30ms, TR 6400ms, matrix 104x104, slice thickness 2mm, 8x SMS acceleration, 72 total slices. Images were acquired of an fBIRN phantom and a human participant under informed consent. An elevated repetition time (TR) was selected than is needed with HB=8 to achieve the needed slice coverage for a comparable single band series to be used for the accurate comparison of images based upon structural similarity index (SSIM), and root mean squared error (RMSE). SMS images were reconstructed with an external calibration dataset, and calibration parameters including x-kernel size (number of points in the x-direction used as weights to fit a given point), ky-kernel size, x-calibration points (number of points in the x-direction used to perform the least squares fitting of the kernel), ky-calibration points, and fitting regularization (lambda scale parameter in Tikhonov regularization4) were modulated in the kernel fitting algorithm. SSIM and RMSE of reconstructed images were calculated with respect to single-band images.Results
Changes in the x-kernel size and number of x-calibration points did not impact SSIM and RMSE measurements (data not shown). Results are shown in Figures 1 and 2 from the phantom experiment, and 3 and 4 from the human experiment.
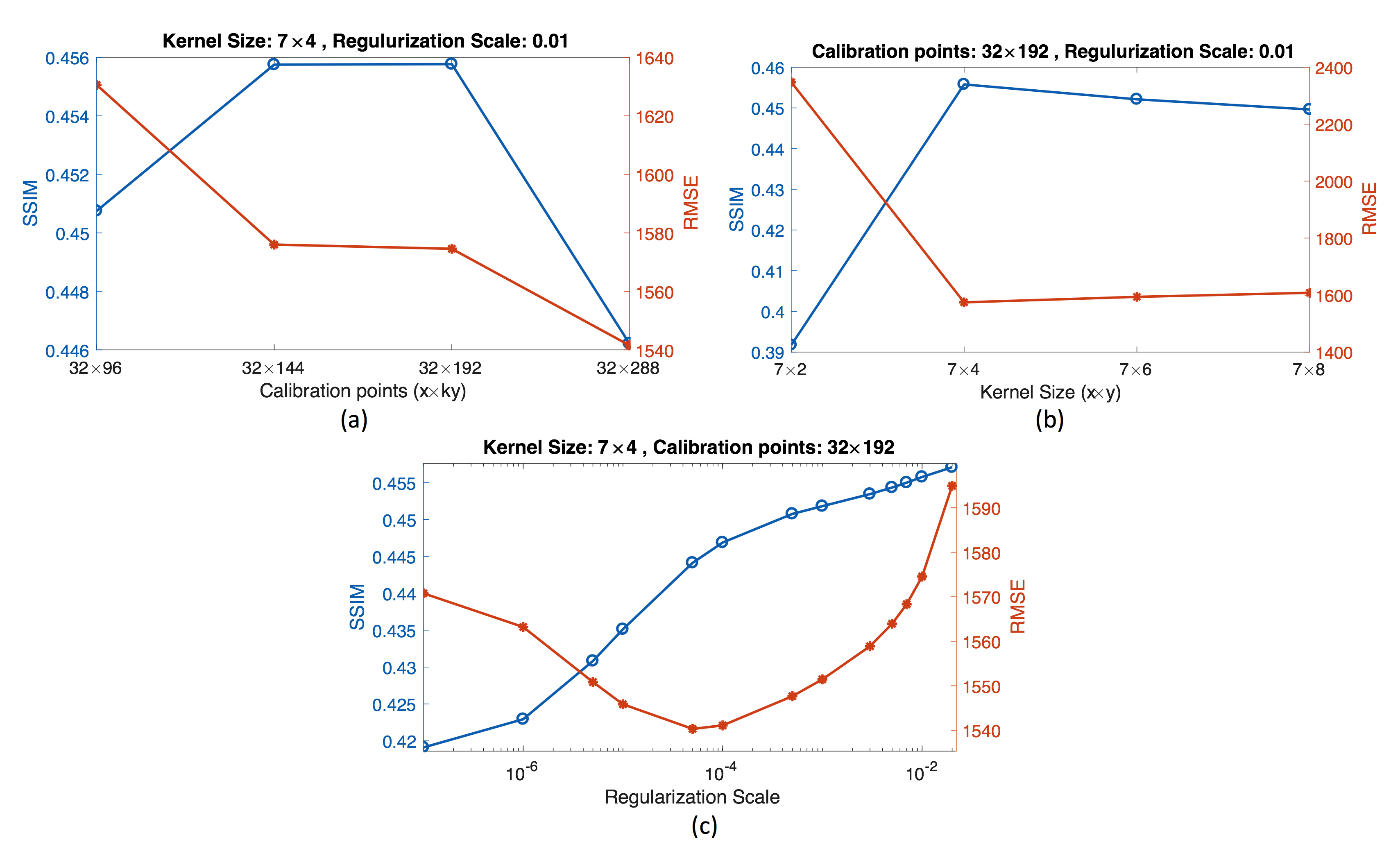
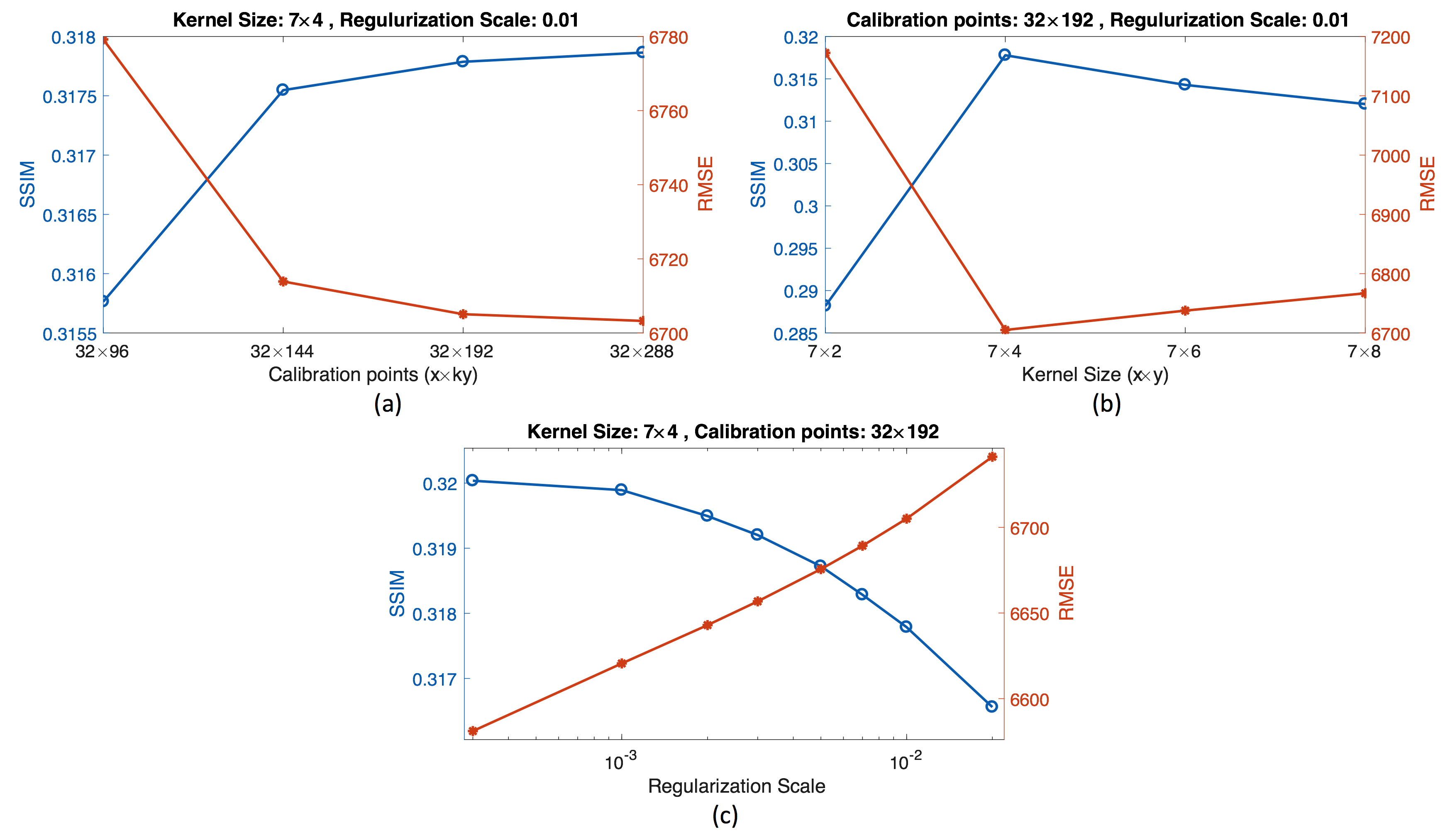
In Figures 1(a) and 3(a) increasing the number of calibration lines in the ky-direction used for fitting the kernel, the GRAPPA equivalent of increasing the autocalibrating (ACS) region, yields improved SSIM and RMSE values. Improvement drops off using at least 144 points. As the number of observations used in fitting the kernel increases, computational time increases linearly5.
Figures 1(b) and 3(b) show dependence upon the number of ky-kernel points. Maximal SSIM and minimal RMSE occurs with 4 ky-kernel points. While the accuracy of the reconstruction degrades slowly with too many kernel points, the fitting algorithm slows by a factor proportional to the square of the number of kernel points5.
Figures 1(c) and 3(c) show opposing trends between the phantom and human experiment. SSIM improves monotonically with regularization and RMSE reaches a minimum with a relatively small (1e-4) regularization parameter in the phantom. In the human, SSIM and RMSE degrade with regularization.
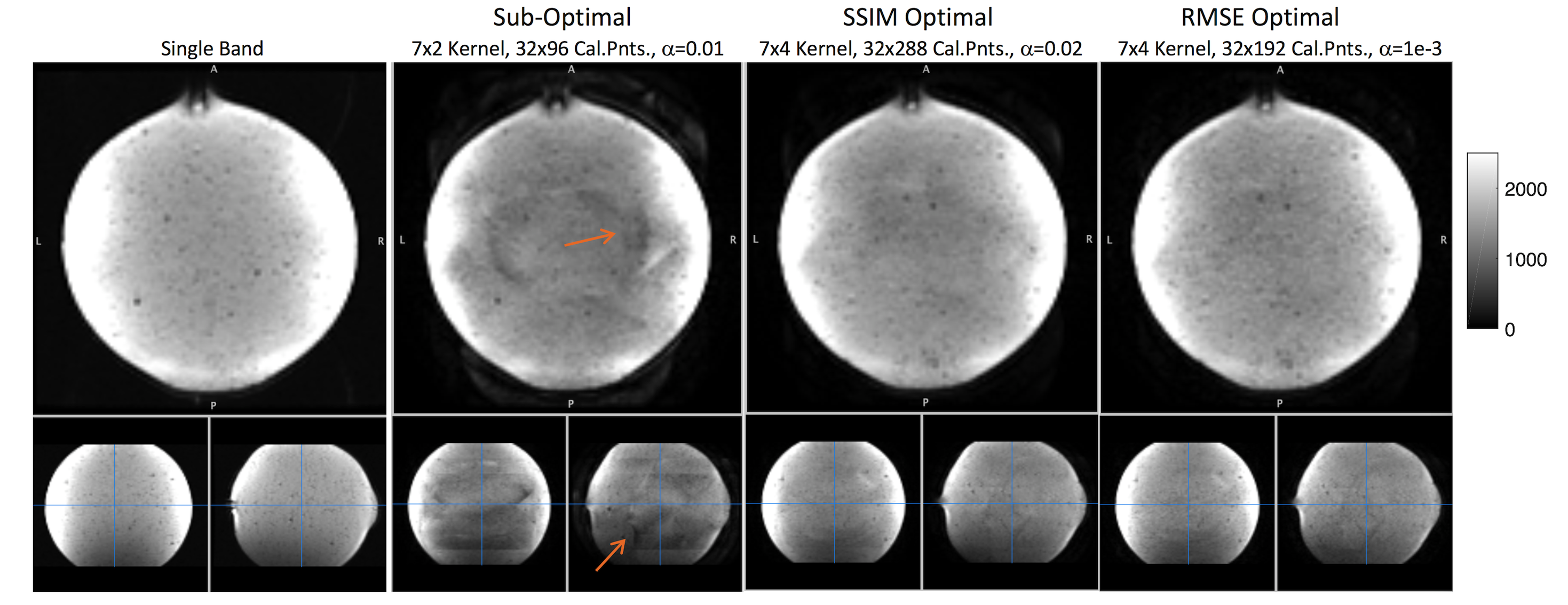
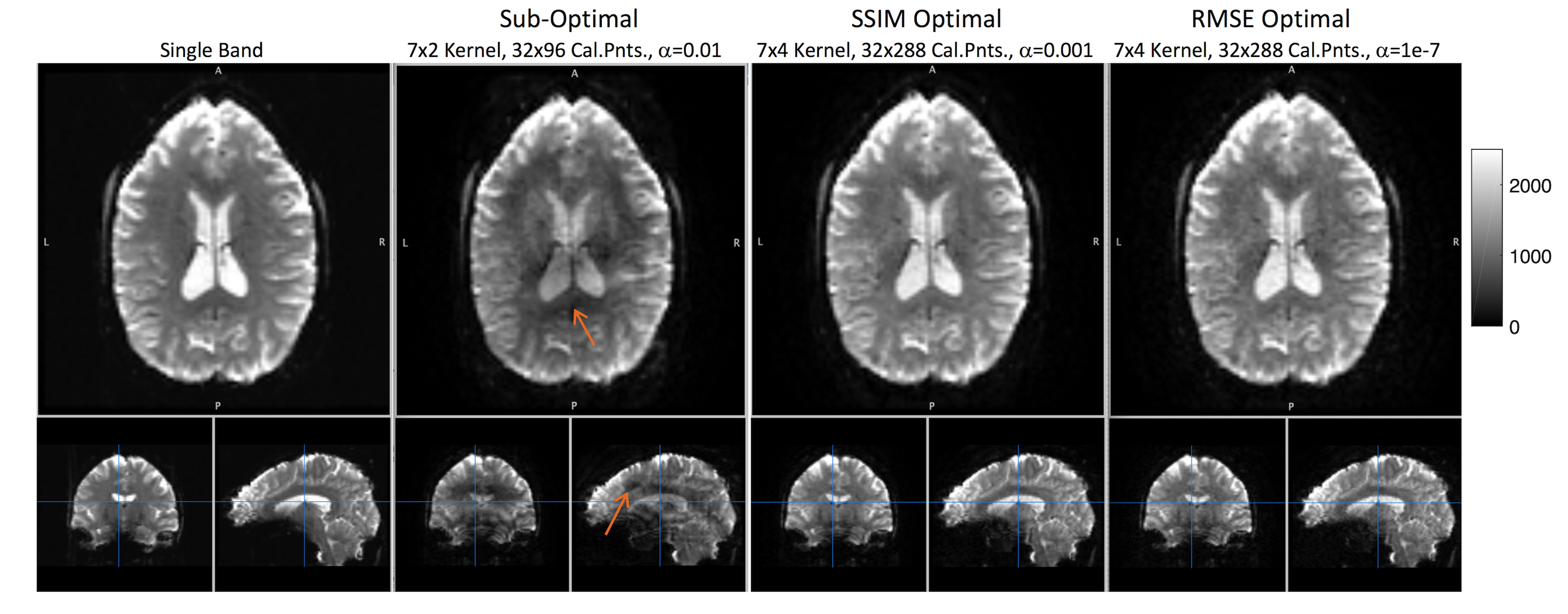
Figures 2 (phantom) and 4 (human) have images from the single band (first column), SMS data with a poorly parameterized calibration algorithm (second column), optimal SSIM calibration algorithm (third column), and optimal RMSE calibration algorithm (fourth column). Minor residual aliasing is apparent in the phantom data in the third and fourth columns, and more subtle shading is apparent in the human data (arrows).
Discussion
Phantom and human experiments showed similar results with changing of kernel size and calibration points, but different results with regularization. This likely results from the low-resolution, external calibration dataset used for kernel fitting. As regularization biases reconstructed images to be similar to calibration data, the uniform phantom does not exhibit degradation with this bias towards smoothness, while the anatomical variation in the human head contains detail that is not captured in the calibration map.
It has been shown that kernel fitting with lower signal-to-noise ratio (regions distant from the center of k-space) yield improved results with GRAPPA6. These results, where kernel fitting includes an increased number of ky-calibration points displaced from the center of k-space, yields results that are consistent with this observation.
Conclusion
Low regularization, and an increase in y-calibration points improves reconstruction performance. A moderate ky-kernel size of 4 points yielded best results. Worse results were obtained with larger and smaller ky-kernel sizes, strong regularization, and reduced ky-calibration points.Acknowledgements
This work supported by GE Healthcare technological development grand.References
1. Brau AC, Beatty PJ, Skare S, Bammer R. Comparison of reconstruction accuracy and efficiency among autocalibrating data-driven parallel imaging methods. Magn Reson Med. 2008; 59:381-395.
2.Beatty PJ, Brau AC, Chang S, et al. A Method for Autocalibrating 2-D Accelerated Volumetric Parallel Imaging with Clinically Practical Reconstruction Times. 2007 ISMRM Proceedings, 2007; 1749.
3. Van Essen DC, Ugurbil K, Auerbach E, The Human Connectome Project: a data acquisition perspective. Neuroimage. 2012; 54:2222-2231.
4. Tiknonov AN, Solution of incorrectly formulated problems and the regularization method". Soviet Mathematics.1963; 4:1035-1038.
5. Teukolsky SA, Flannery BP, Press WH, Vetterling WT, Numerical recipes in C. SMR; 1992.
6. Ding Y, Xue H, Ahmad R, Chang TC, et al. Paradoxical effect of the signal‐to‐noise ratio of GRAPPA calibration lines: A quantitative study. Magn Reson Med. 2015; 74(1): 231-239.
Figures