3928
Real-time fMRI amygdala neurofeedback training reduces depression symptoms and appears to normalize amygdala and hippocampal volumes1Laureate Institute for Brain Research, Tulsa, OK, United States, 2Electrical and Computer Engineering, University of Oklahoma, Tulsa, OK, United States, 3Department of Psychiatry, University of Pittsburg, Pittsburg, PA, United States, 4Stephenson School of Biomedical Engineering, University of Oklahoma, Norman, OK, United States
Synopsis
We evaluated structural brain changes as a result of real-time fMRI neurofeedback (rtfMRI-
Introduction
Although real-time functional magnetic resonance imaging neurofeedback (rtfMRI-nf) increases amygdala response to positive memories while significantly decreasing depressive symptoms1, research has yet to identify how rtfMRI-nf impacts brain structure. This study examined acute rtfMRI-nf training effects on anatomical brain structures, with a specific focus on amygdala and hippocampus grey matter volumes in a cohort of individuals with major depressive disorder (MDD). We also investigated the association between pre-training volume abnormalities and volume change after rtfMRI-nf training.
Method
We analyzed structural MRI data in previously published two studies of rtfMRI-nf training1,2. Unmedicated MDD patients (N=62; 46 female; ages 18-55) were randomly assigned to receive two rtfMRI-nf sessions either from the left amygdala (N=33, active) or left intraparietal sulcus, a region putatively not involved in emotional processing (N=29, control). Two rtfMRI-nf sessions were performed on separate days (interval between sessions: M=8 days, SD=4 days). Structural T1-weighted MRI scans were obtained at each day before the nf training, which were analyzed as pre- (1st session) and post-training (2nd session) scans to investigate structural change between the sessions. MDD symptoms were assessed with the Montgomery-Åsberg Depression Rating Scale (MADRS)3 one week before the first session and week after the second session. FreeSurfer (version 20180607) was used to process structural MRI images utilizing a longitudinal processing pipeline4,5. Seven hippocampus subregions6 and nine amygdala nuclei7 were evaluated. Two sets of statistical analyses were performed to test hypotheses. First, linear mixed-effect model (LME) analysis tested volume changes due to training (e.g., post- minus pre-training; dependent variable) with fixed effects of rtfMRI-nf group (active, control), MADRS symptom change (post- minus pre-training), brain laterality (left, right), and their interactions, with age, estimated total intracranial volume (eTIV), scan interval, and sex. Random effects included subject and study. Power-proportion correction8 was applied to the eTIV covariate. With 16 multiple independent tests, the significance level was set to p<0.05/16=0.003 for multiple comparison correction. Next, informed by the first analysis, in the regions with significant volume change due to nf training, we investigated pre-training volume abnormalities in MDD. Pre-training abnormalities in MDD were quantified by comparing to a healthy volume estimated within a healthy cohort (HC; N=62). A linear model was fitted for each volume with age, sex, and eTIV covariates for HC samples. The model was used for each MDD subject to estimate a demographically-matched healthy regional brain volume, and then the difference between the estimated volume and actual MDD pre-training volumes (normalized by the standard deviation of HC residual values) was calculated as a measure of pre-training volume abnormalities. An LME analysis tested such volume changes (dependent variable) with fixed effects of the pre-training volume abnormality, rtfMRI-nf group, brain laterality, age, eTIV, scan interval, sex, and random effects of subject and study.Results
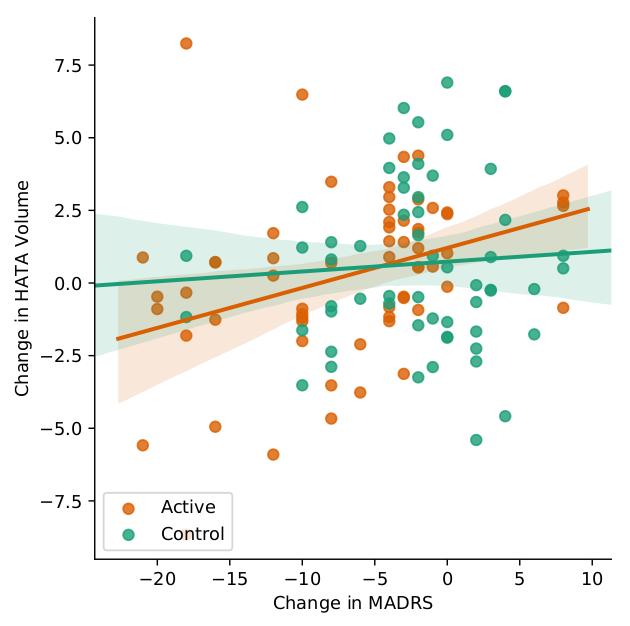
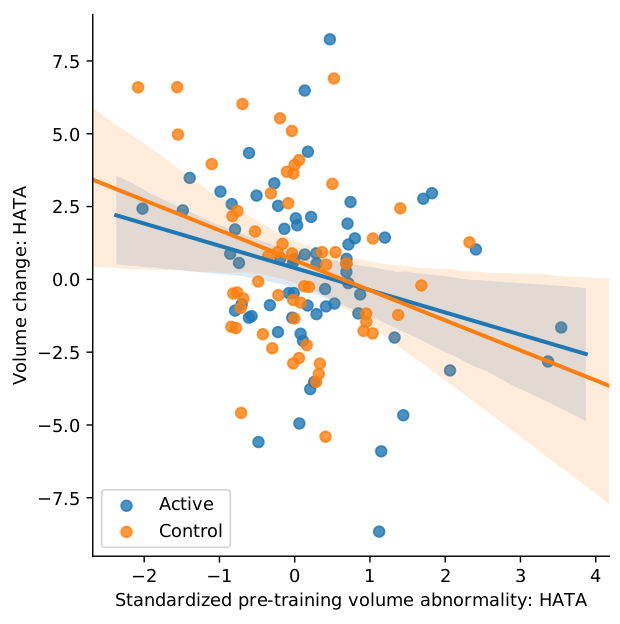
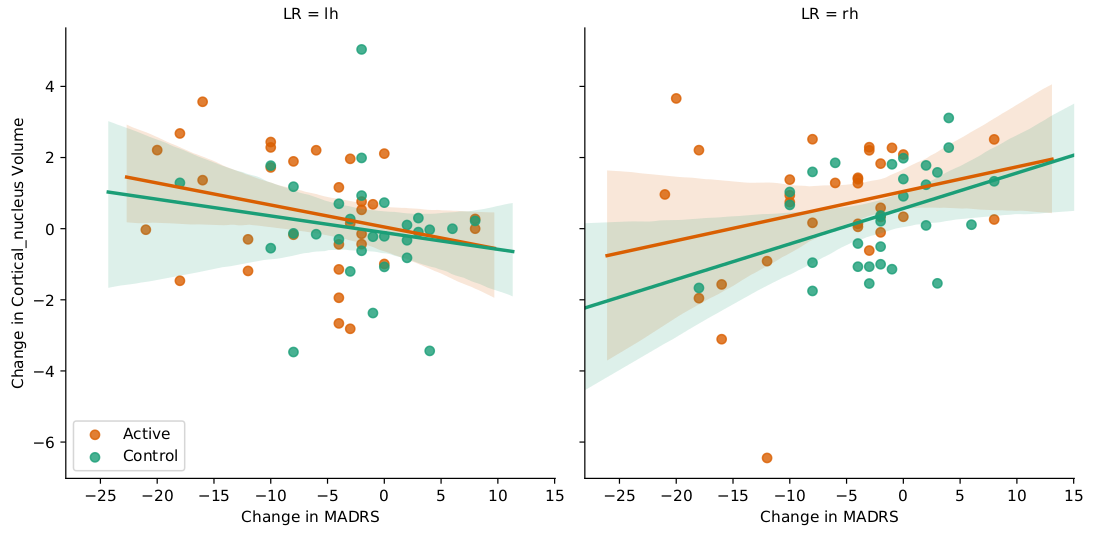
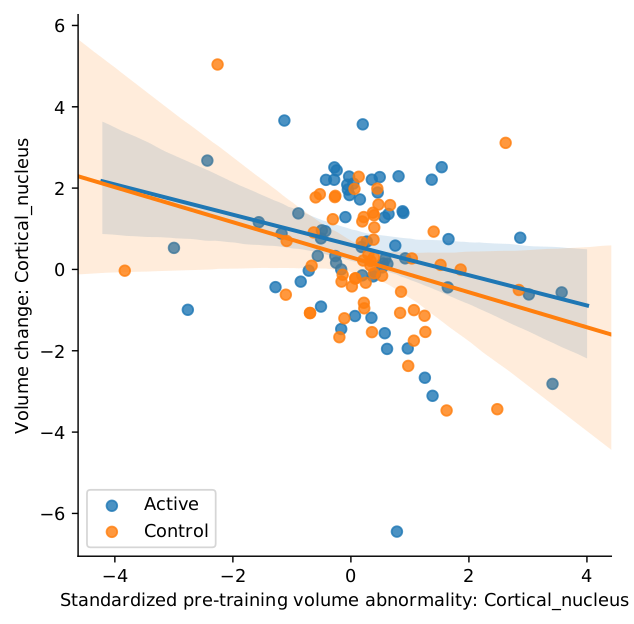
Figure 1 illustrates that Hippocampus Amygdala Transition Areas (HATA) volume decreases were associated with MADRS decreases, t(52)=3.29, p=0.002; this effect was significant for the active group, t(52)=3.29, p=0.004, but not the control group, t(52)=0.57, p=0.813. Figure 2 demonstrates that larger pre-training HATA volume abnormalities were associated with greater HATA decreases across active and control groups, t(97)=-3.46, p<0.001. Amygdala cortical nucleus decreases were linked to MADRS decreases that differed as a function of brain laterality (p=0.002 for the interaction of MADRS decreases by laterality). Figure 3 shows that this relationship was more significant for the right, t(99)=2.56, p=0.024, than the left, hemisphere t(99)=-1.37, p=0.313. Figure 4 indicates that larger pre-training volume abnormalities were associated with greater cortical nucleus decreases across active and control groups, t(116)=-2.73, p=0.007.Discussion
Decreases in hippocampus HATA and amygdala cortical nucleus volume were associated with decrease in MDD symptoms as an acute (one-week after the training) effect of a single rtfMRI-nf training session. Although decreased hippocampus volume was consistently reported for MDD patients, amygdala volume abnormality for MDD was not consistent across studies9,10. Results indicated that volume reduction due to a single nf training was more pronounced for a patient with larger volume abnormality at pre-training baseline. Importantly, this suggests individual variability of volume abnormality for MDD patients and an acute effect of the training on the hippocampus and amygdala volumes could be seen as normalizing an abnormally increased volume of the regions.Conclusion
Depression symptom decrease with rtfMRI-nf amygdala training was associated with normalizing (decreasing) amygdala and hippocampus volumes in MDD patients. Results also suggest that individual differences in pre-treatment grey matter volume abnormalities may contribute to the degree of structural volume changes that can be anticipated to be recovered by rtfMRI-nf interventions.Acknowledgements
This work was supported by the Laureate Institute for Brain Research.References
[1] Young, K.D., Siegle, G.J., Zotev, V., Phillips, R., Misaki, M., Yuan, H., Drevets, W.C., Bodurka, J., 2017. Randomized Clinical Trial of Real-Time fMRI Amygdala Neurofeedback for Major Depressive Disorder: Effects on Symptoms and Autobiographical Memory Recall. Am J Psychiatry 174, 748-755.
[2] Young, K.D., V. Zotev, R. Phillips, et al., Real-time FMRI neurofeedback training of amygdala activity in patients with major depressive disorder. PLoS One, 2014;9(2):e88785.
[3] Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry 1979, 134:382–389.
[4] Reuter, M., et al. (2012). Within-subject template estimation for unbiased longitudinal image analysis. Neuroimage, 61(4), pp. 1402-18.
[5] Iglesias JE, Van Leemput K, Augustinack J, Insausti R, Fischl B, Reuter M. Bayesian longitudinal segmentation of hippocampal substructures in brain MRI using subject-specific atlases. Neuroimage, 141, November 2016, 542-555.
[6] Iglesias, J.E., et al. (2015). A computational atlas of the hippocampal formation using ex vivo, ultra-high resolution MRI: Application to adaptive segmentation of in vivo MRI. Neuroimage, 115, pp. 117-37.
[7] Saygin ZM & Kliemann D (joint 1st authors), Iglesias JE, van der Kouwe AJW, Boyd E, Reuter M, Stevens A, Van Leemput K, Mc Kee A, Frosch MP, Fischl B, Augustinack JC. High-resolution magnetic resonance imaging reveals nuclei of the human amygdala: manual segmentation to automatic atlas. Neuroimage, 155, July 2017, 370-382.
[8] Liu, D., et al. (2014), ‘The power-proportion method for intracranial volume correction in volumetric imaging analysis’, Front Neurosci, 8, 356.
[9] Averill, C.L., R.M. Satodiya, J.C. Scott, et al., Posttraumatic Stress Disorder and Depression Symptom Severities Are Differentially Associated With Hippocampal Subfield Volume Loss in Combat Veterans. Chronic Stress (Thousand Oaks), 2017;1.
[10] Schmaal, L., D.J. Veltman, T.G. van Erp, et al., Subcortical brain alterations in major depressive disorder: findings from the ENIGMA Major Depressive Disorder working group. Mol Psychiatry, 2016;21(6):806-12
Figures