3901
Resting-state network distinguishes level of cerebral microbleed burden in patients with Immune Thrombocytopenia1Medicine, Imperial College London, London, United Kingdom, 2Haematology, Imperial College London, London, United Kingdom, 3Clinical Brain Sciences, University of Edinburgh, Edinburgh, United Kingdom
Synopsis
In this study we evaluated resting state networks associated with cerebral microbleed presence in patients diagnosed with Immune Thrombocytopenia and identified a potential correlate of tiredness in the right superior parietal lobule.
Introduction
Immune Thrombocytopenia (ITP) is an autoimmune disease characterized by a low platelet count (<100 x 109/L) and exclusion of other causes of thrombocytopenia [1]. Most patients diagnosed with ITP experience bleeding symptoms in varying locations of the body, therefore current treatment is aimed at both increasing platelet count and avoiding any major bleeding events.
Recently it was discovered that ITP patients habor tiny hemosiderin blood deposits in the brain called cerebral microbleeds (CMBs). CMBs have been observed in numerous other clinical populations and are thought to be associated with reductions in cognitive performance [2-4].
In this study we evaluated, (i) the prevalence of CMBs in adult ITP patients (ii) risk factors for CMB development and (iii) resting-state functional magnetic resonance imaging (rsfMRI) networks associated with different levels of CMB burden.
Methods
With approval from our internal ethics committee, 51 patients (29 F; median age 39 (range 18-87)) diagnosed with ITP provided informed written consent to participate in this prospective study. Inclusion criteria included at least one platelet count <30 x 109/L over the course of their disease and no contraindications to MRI. All imaging data were acquired on a 3T scanner (Siemens Verio). The dedicated imaging protocol included susceptibility-weighted imaging (SWI) (TR/TE = 28ms/20ms, FA=15, .5x.5 mm in-plane resolution, 1mm slice thickness, 35x45cm FOV) and rsfMRI (TR/TE = 2000ms/30ms, FA =80,3x3mm in-plane resolution, 3mm slice thickness, 384x384 pixel resolution).
CMBs were quantified by an experience rater using a semi-automated CMB detection algorithm [5]. A multivariate logistic regression was used to assess the relationship between CMB burden and clinical characteristics including platelet count, disease duration, and number of treatments. Resting-state fMRI data were analysed for a sub-set of patients (44/51) using a group-level independent component analysis (ICA) from FSL's MELODIC ICA software package [6]. A logistic dual-regression revealed network differences for patients with low versus high CMB burden characterized as less than 3 or 3 or more CMBs, respectively.
Results
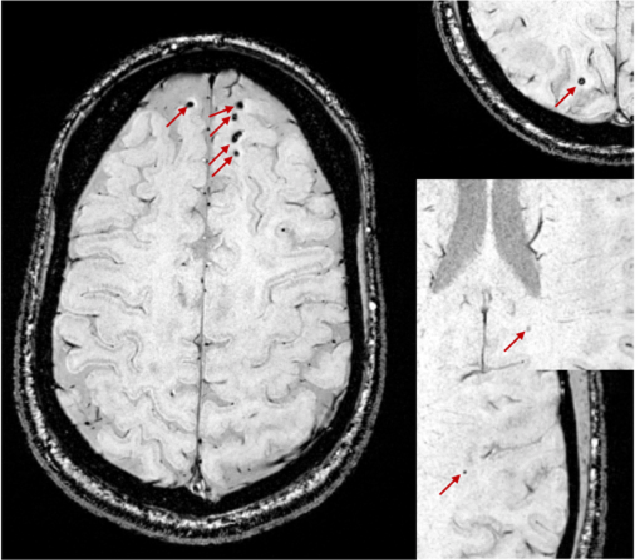
Cerebral microbleeds were detected in 45% (23/51) patients (Fig 1). Approximately 10% (5/51) of patients whom had disease durations greater than 10 years presented with more than 5 CMBs. One of these patients who had 16 CMBs, predominately in the frontal lobe, had experienced a head injury during their disease course (Fig 2). Another patient whom underwent total body irradiation following an allogenic transplant, presented with a total of 56 CMBs.
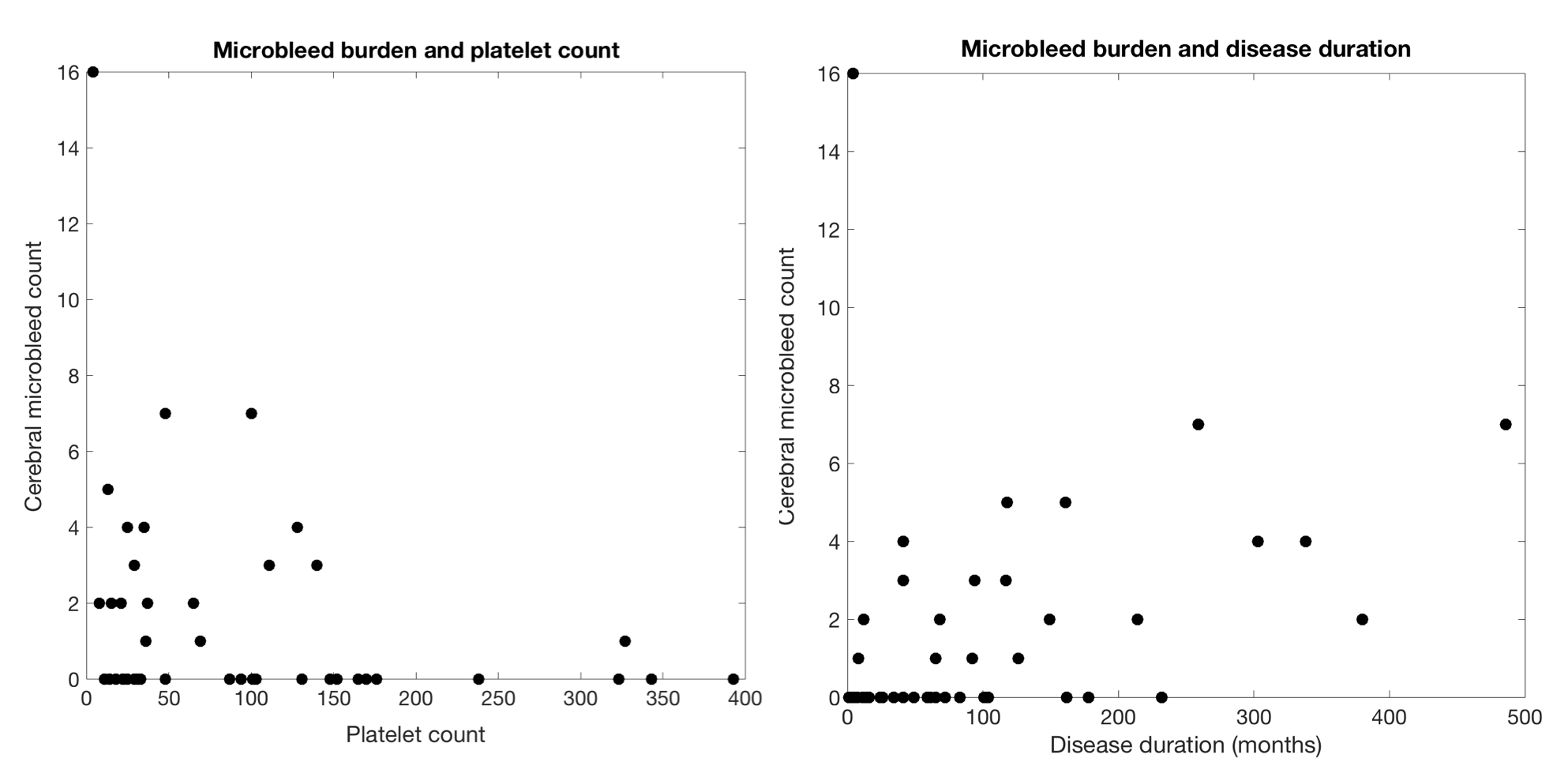
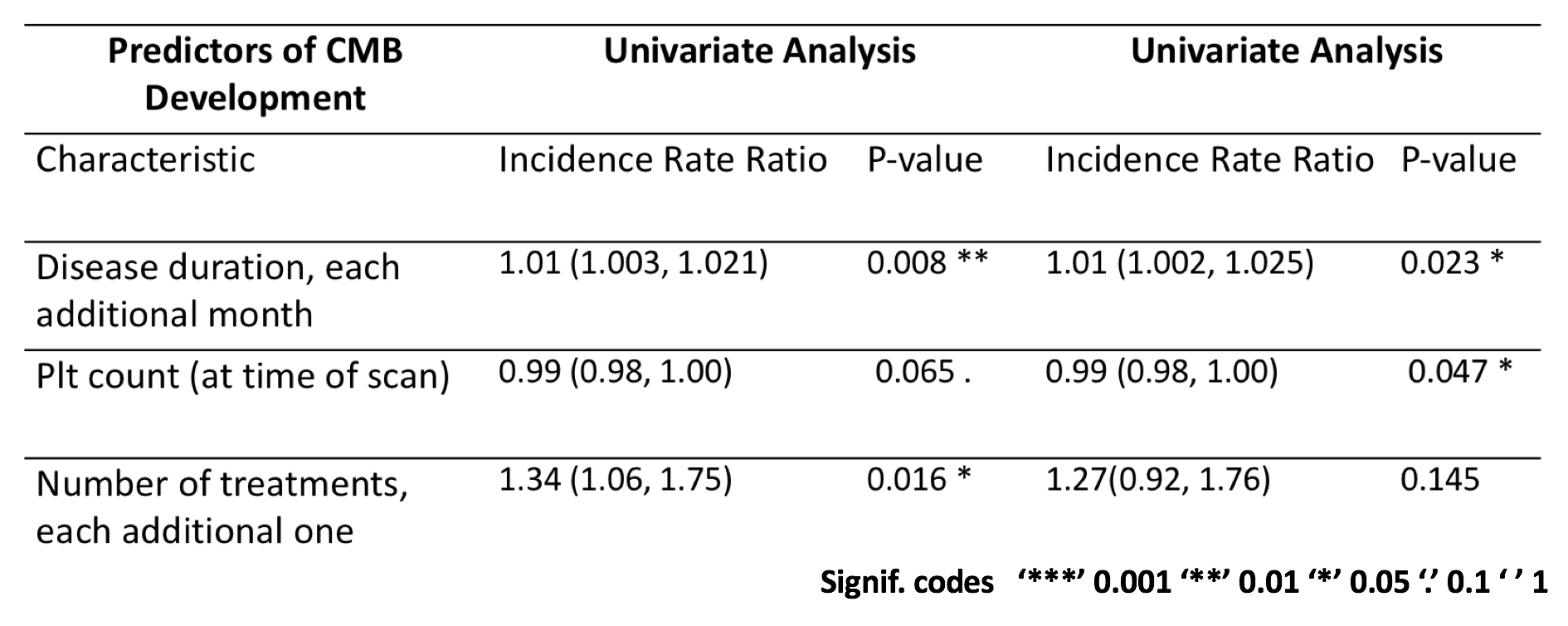
Multivariate analysis revealed significant associations between CMB burden, disease duration (p-value = .035) and platelet count (p-value = .053). Longer disease durations and lower platelet counts, as expected, were risk factors for increased CMB burden (Fig 3).
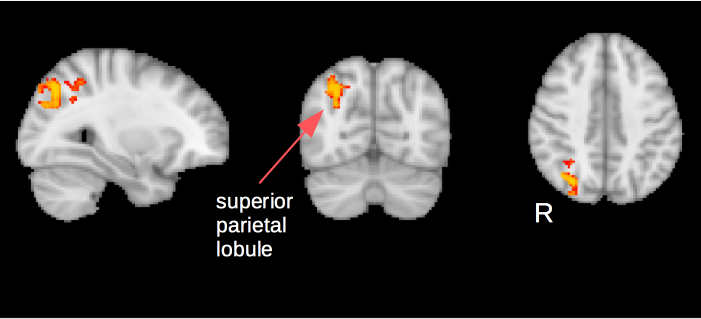
Connectivity analysis revealed an area of increased connectivity in the right superior parietal lobe for patients included in the high CMB burden group, denoted as having 3 or more bleeds (Fig 4).
Discussion
The results from this study confirm the presence of CMBs in ITP patients and furthermore provide markers for risk assessment of CMB development. One of the main concerns with CMB presence as previously mentioned, is its potential impact on cognitive performance [2-4]. Unfortunately in the present work we were unable to assess the relationship between CMB burden and direct measures of cognitive performance, however, our rsfMRI connectivity analysis revealed an area of increased connectivity in the superior parietal lobule for patients in the high CMB burden group. This area of the brain has previously been associated with aspects of attention and visuospatial perception [7], potentially providing a correlate of chronic tiredness that is often experienced by ITP patients and proven difficult to quantify using subjective measurements. Augmented by ongoing recruitment, future work will evaluate these networks longitudinally and in comparison to healthy control data.
MRI may play a valuable role in the clinical management of ITP patients, as a means of assessing disease-related neuropathologies and the degree to which they manifest as a clinical symptom.
Acknowledgements
The authors would like to acknowledge support from Albert Busza at the Imperial College Clinical Imaging Facility.References
[1] Rodeghiero F, Stasi R, Gernsheimer T, et al. Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adutls and children: report from an international working group. Blood, 2009, 113(11):2386-93.
[2] Roddy E. Sear K, Felton E, et al. Presence of cerebral microbleeds is associated with worse executive function in pediatric brain tumor survivors. Neuro Oncol, 2016, 18(11):1548-1558.
[3] Li X, Yuan J, Yang L, et al. The significant effects of cerebral microbleeds on cognitive dysfunction: An updated meta-analysis. PLoS One, 2017, 12(9), e0185145.
[4] Cerebral microbleeds are associated with worse cognitive function: The Rotterdam Scan Study. Neurology, 2012, 78(5):326-333.
[5] Morrison MA, Payabvash S, Chen Y, et al. A user-guided tool for semi-automated cerebral microbleed detection and volume segmentation: evaluating vascular injury and data labeling for machine learning. NeuroImage: Clinical, 2018, 20:498-505.
[6] Jenkinson M, Beckmann CF, Behrens TE, et al. FSL. NeuroImage, 2012, 62:782-90.
[7] Wu Y, Wang J, Zhang Y, et al. The Neuroanatomical basis for posterior superior parietal lobule control lateralization of visuospatial attention. Front Neuroanat, 2016, 10:32.
Figures