3884
Disrupted Cerebellar Connectivity with the Central Executive Network and the Default-mode Network in unmedicated Bipolar II Disorder1Medical Imaging Center, First Affiliated Hospital of Jinan University, Guangzhou, China, 2Institute of Molecular and Functional Imaging, Jinan University, Guangzhou, China, 3Department of Psychiatry, First Affiliated Hospital of Jinan University, Guangzhou, China, 4Department of Radiology, Six Affiliated Hospital of Sun Yat-sen University, Guangzhou, China, 5Department of Radiology, Gansu Provincial Hospital, Gansu, China, 6GE Healthcare, MR Research China, Beijing, China
Synopsis
The present study aims to investigate the FC between the cerebellum and cerebrum, particularly the central executive network (CEN) and the default-mode network (DMN) in BD II. Seed-based connectivity analyses were performed in 94 unmedicated BD II depression and 100 healthy controls (HCs). Patients with BD II depression showed disrupted FC between the cerebellum and the CEN (mainly in the left dlPFC and ACC) and DMN (mainly in the left mPFC and temporal lobe), suggesting the significant role of the cerebellum-CEN and -DMN connectivity in the pathogenesis of BD.
Introduction
The cerebellum was recently reported to participate in not only motor fuctions but also higher-order functions, such as cognition as well as emotion 1-3. And several resting-state functional magnetic resonance imaging (rs-fMRI) data have demonstrated FC between the cerebellar subregions and cerebral networks in normal humans, particularly the central executive network (CEN) and the default-mode network (DMN) 4-6. Bipolar disorder (BD) is a common psychiatric disease. Although structural and functional abnormalities of the cerebellum in BD patients have been reported by recent neuroimaging studies 7-9, the cerebellar-cerebral functional connectivity (FC) has not yet been examined. The present study aims to investigate the FC between the cerebellum and cerebrum, particularly the CEN and the default-mode network DMN in bipolar II disorder (BD II).Methods
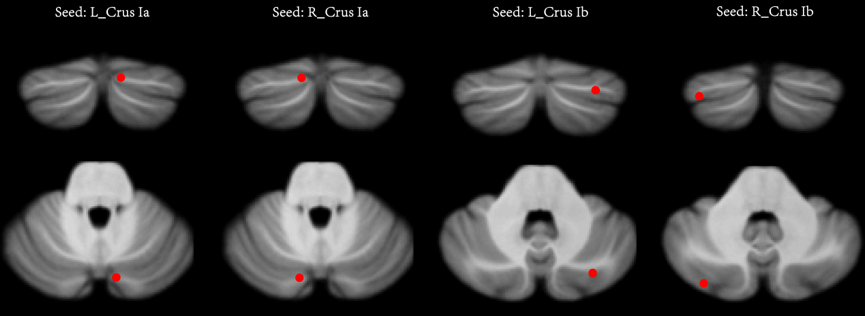
All patients met Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (known as DSM-V) criteria for BD II according to the diagnostic assessment by the Structured Clinical Interview for DSM-V Patient Edition (SCID-P). And they were diagnosed with total YMRS score<7 and HDRS-24 score>21. Ninety-four patients with unmedicated BD II depression and 100 healthy controls (HCs) underwent the resting-state functional magnetic resonance imaging. Seed-based connectivity analyses were performed using cerebellar seeds previously identified as being involved in the CEN (bilateral Crus Ia) and DMN (bilateral Crus Ib) (Fig. 1). The two-sample t test was performed to assess the significant differences of the FC for each seed between BD II and HCs. Age, gender and the mean framewise displacement were included as nuisance covariates. Statistical maps were thresholded using permutation tests (1000 trials). The threshold-free cluster enhancement and voxel-wise correction with permutation tests were tested at two-tailed p<0.05 for multiple comparisons.Results
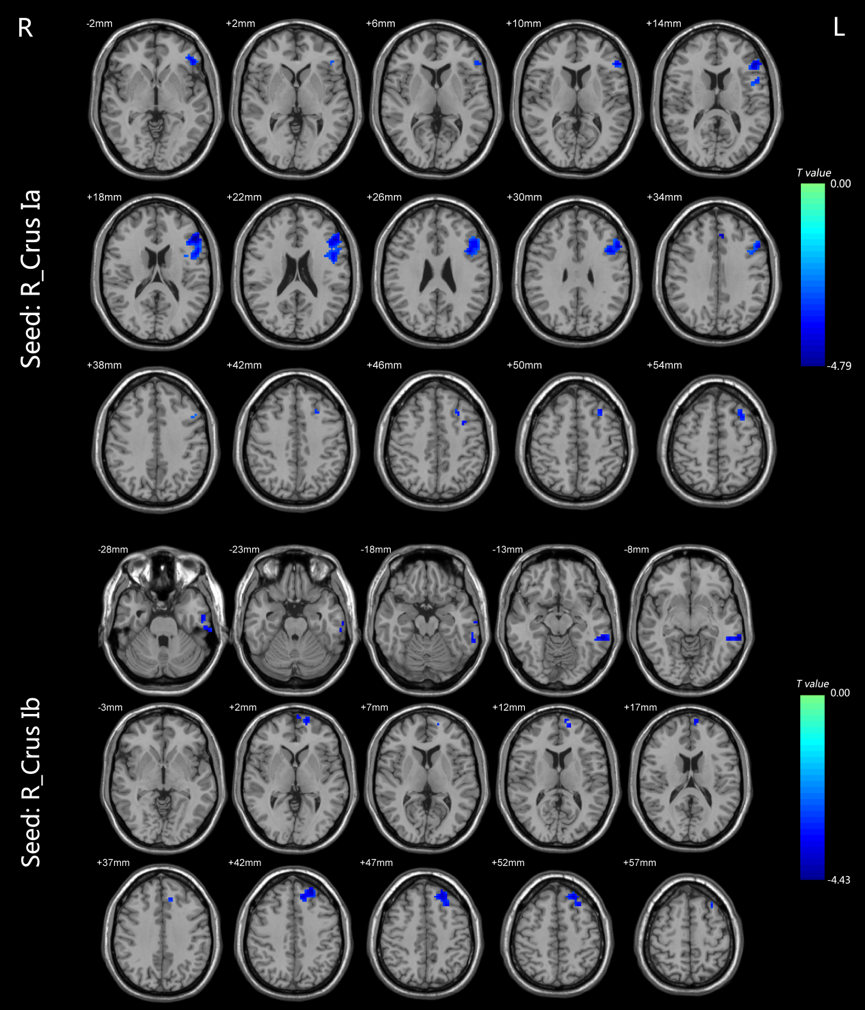
Compared with HCs, BD II depression patients appeared decreased FC in the right Crus Ia-left dorsal lateral prefrontal cortex (dlPFC) and -left anterior cingulate cortex (ACC), the right Crus Ib-left medial prefrontal cortex (mPFC), -left middle temporal gyrus (MTG), and -left inferior temporal gyrus (ITG) (Fig.2). No altered FC between the left Crus Ia or Crus Ib and the cerebral regions was found.Discussion and conclusion
Patients with BD II depression showed disrupted FC between the cerebellum and the CEN (mainly in the left dlPFC and ACC) and DMN (mainly in the left mPFC and temporal lobe), suggesting the significant role of the cerebellum-CEN and -DMN connectivity in the pathogenesis of BD.Acknowledgements
No acknowledgement found.References
1. Kirschen MP, Davis-Ratner MS, Milner MW, Chen SHA, Schraedley-Desmond P, Fisher PG, et al. Verbal memory impairments in children after cerebellar tumor resection. Behav Neurol. 2008; 20:39-53.
2. Laricchiuta D, Petrosini L, Picerni E, Cutuli D, Iorio M, Chiapponi C, et al. The embodied emotion in cerebellum: a neuroimaging study of alexithymia. Brain Struct Funct. 2015; 220:2275-87.
3. Stoodley CJ, Schmahmann JD. Functional topography in the human cerebellum: A meta-analysis of neuroimaging studies. Neuroimage. 2009; 44:489-501.
4. Habas C, Kamdar N, Nguyen D, Prater K, Beckmann CF, Menon V, et al. Distinct Cerebellar Contributions to Intrinsic Connectivity Networks. J Neurosci. 2009; 29:8586-94.
5. Krienen FM, Buckner RL. Segregated Fronto-Cerebellar Circuits Revealed by Intrinsic Functional Connectivity. Cereb Cortex. 2009; 19:2485-97.
6. Sang L, Qin W, Liu Y, Han W, Zhang YT, Jiang TZ, et al. Resting-state functional connectivity of the vermal and hemispheric subregions of the cerebellum with both the cerebral cortical networks and subcortical structures. Neuroimage. 2012; 61:1213-25.
7. Zhao L, Wang Y, Jia Y, Zhong S, Sun Y, Zhou Z, et al. Cerebellar microstructural abnormalities in bipolar depression and unipolar depression: A diffusion kurtosis and perfusion imaging study. Journal of Affective Disorders. 2016; 195:21-31.
8. Dolan RJ, Bench CJ, Brown RG, Scott LC, Friston KJ, Frackowiak RS. Regional cerebral blood flow abnormalities in depressed patients with cognitive impairment. J Neurol Neurosurg Psychiatry. 1992; 55:768-73.
9. Liu CH, Li F, Li SF, Wang YJ, Tie CL, Wu HY, et al. Abnormal baseline brain activity in bipolar depression: A resting state functional magnetic resonance imaging study. Psychiat Res-Neuroim. 2012; 203:175-9.
Figures