3878
Regional Brain Resting-State Neural Activity in Patients with Single Ventricle Heart Disease1Departments of Anesthesiology, University of California Los Angeles, Los Angeles, CA, United States, 2School of nursing, University of California Los Angeles, Los Angeles, CA, United States, 3Division of Pediatric Cardiology, University of California Los Angeles, Los Angeles, CA, United States, 4Division of Pediatric Cardiology, Children's Hospital Los Angeles, Los Angeles, CA, United States, 5University of California Los Angeles, Los Angeles, CA, United States
Synopsis
Patients with single ventricle heart disease (SVHD) commonly show brain structural
injuries in autonomic, mood, and cognition regulatory areas. However, whether SVHD
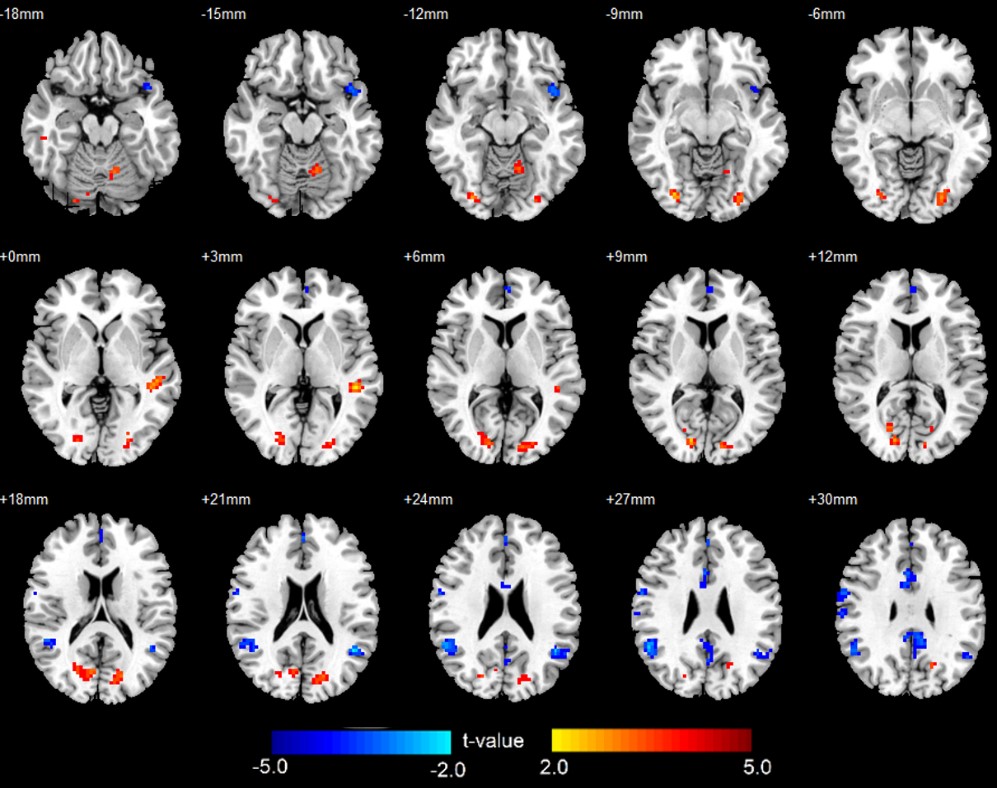
subjects have functional impairments in these sites is unknown. We examined regional
neural activity changes in SVHD patients, and found reduced regional
homogeneity (ReHo) in posterior cingulate, medial prefrontal cortex, inferior
parietal lobule, and left insula, and increased ReHo in bilateral middle
occipital gyrus, cerebellar cortices, and left superior temporal gyrus over control
subjects. These functional changes might be associated with impairments in autonomic,
mood, and cognitive functions found in the condition.
Introduction
Single ventricle heart disease (SVHD) is a form of complex congenital heart disease, with only one ventricle has formed, instead of two. Patients with SVHD undergo multiple heart surgeries at a young age and show brain injury in sites that control autonomic, mood, and cognitive deficits,1 functions that are deficient in the condition. However, it is unclear whether SVHD subjects have altered neural activities in restating-state. Resting‐state functional magnetic resonance imaging (fMRI) measures the blood-oxygen-level dependent (BOLD) signal changes induced by spontaneous neural activities. Among all the fMRI procedures, regional homogeneity (ReHo) is better to examine local coherence neuronal activities, and can be used to examine brain functional integrity of SVHD patients. The procedures have been widely-applied in various clinical studies to examine neural activities and brain functions in heart failure and other neurological diseases, 2 and thus, may be useful in assessing brain resting-state neural activity in SVHD subjects. Our aim was to examine regional brain neural activity changes in SVHD patients compared to healthy controls using fMRI-based ReHo procedures.Methods
We collected high-resolution T1-weighted and resting-state fMRI data from 13 SVHD (age, 15.7±1.4 years; 7 male) and 17 control subjects (age, 15.9±1.4 years; 9 male), using a 3.0-Tesla MRI (Siemens, Prisma) scanner. BOLD-fMRI data were collected with an echo planar imaging (EPI)‐based pulse sequence in the axial plane (repetition time [TR] = 2,000 ms; echo time [TE] = 30 ms; flip angle [FA] = 90°; field‐of‐view [FOV] = 230 × 230 mm2; matrix size = 64 × 64; slice thickness = 4.2 mm; volumes = 59). High resolution T1-weighted images were collected using a magnetization prepared rapid acquisition gradient-echo (MPRAGE) pulse sequence (TR = 2200 ms; TE = 2.4 ms; inversion time = 900 ms; FA = 9 °; matrix size = 320 × 320; FOV = 230 × 230 mm; slice thickness = 0.9 mm; number of slices = 192). After standard pre-processing, we calculated whole-brain ReHo maps of each subject by evaluating the temporal similarity between the fMRI time course of each voxel with the nearest neighbors. The ReHo maps were normalized to a common space, transformed to z-score maps, and compared between groups using ANCOVA (FDR corrected p<0.05; covariates: age and sex).Results
No significant differences in age or sex appeared between groups. Reduced ReHo appeared in multiple sites in SVHD, including the posterior cingulate, medial prefrontal cortex, inferior parietal lobule, and left insula. In addition, increased ReHo appeared in bilateral middle occipital gyrus, cerebellar cortices, and left superior temporal gyrus in SVHD over controls.Discussion
SVHD subjects showed altered resting-state neural activity in the insula and other brain areas. Previous studies suggested that the left insula is important for parasympathetic activities, and lateralized impairment in the insula may result in increased sympathetic tones, as reported in adult heart failure subjects.2 Thus, the reduced left insula regional neural synchronization may indicate impaired autonomic regulatory functions in SVHD. Decreased ReHo also appeared in the posterior cingulate, medial prefrontal cortex, and inferior parietal lobule may reflect impairment in the default mode network (DMN), a circuit responsible for high-order cognition, sleep, and mood regulations,3 and impairments in network may underlying various cognitive and mood symptoms in the condition. The increased ReHo emerged in visual, auditory, and motor areas, indicating hyper-activities in the perceptual networks. These increased regional neural activities in the perceptual circuits might be a compensatory mechanism for impaired high order cognitive functions in the condition.Conclusion
Adolescents with SVHD show significant regional neural activity changes at resting-state in brain areas that are associated with autonomic, mood, and cognition regulation functions. The functional deficits may result from delayed brain development and/or hypoxia/ischemia-induced structural changes in the condition.Acknowledgements
This research work was supported by the National Institutes of Health R01NR 013930 and R01NR016463.References
1.Tyagi M, Fteropoulli T, Hurt CS, et al. Cognitive dysfunction in adult CHD with different structural complexity. Cardiology in the young. Jul 2017;27(5):851-859.
2. Song X, Roy B, Fonarow GC, Woo MA, Kumar R. Brain structural changes associated with aberrant functional responses to the Valsalva maneuver in heart failure. Sep 2018;96(9):1610-1622.
3. Raichle ME, MacLeod AM, Snyder AZ, Powers WJ, Gusnard DA, Shulman GL. A default mode of brain function. Proceedings of the National Academy of Sciences. 2001;98(2):676-682.
Figures