3851
Feasibility and Demonstration of Controlled, Comprehensive Delivery of Clot-busting Drugs for MR Image-Guided Intracerebral Clot Evacuation1Medical Physics, University of Wisconsin, Madison, WI, United States, 2Animal Sciences, University of Wisconsin, Madison, WI, United States, 3Radiology, University of Wisconsin, Madison, WI, United States, 4Neurosurgery, University of Wisconsin, Madison, WI, United States
Synopsis
A recent NIH Trial has shown success in minimizing the effects of intracerebral hemorrhage through insertion of a minimally invasive catheter into the clot through a craniotomy. The catheter then injects 1 ml of clot-busting drugs followed by an 8 hour period of draining the lysed blood. The conservative procedure is repeated for 3-5 days as only very small dosages can be administered due to CT’s inability to directly monitor the drug’s safe distribution. We demonstrate how pressurized infusions can create broader treatments that lyse the clot rapidly while MRI visualizes the drug distributions to maintain safety.
Introduction
Currently,
the primary clinical treatment of intracerebral hemorrhage (ICH) simply stabilize
the patient’s condition, resigning the individual to a lifetime of considerable
cognitive deficits, motor deficits, loss of independence, and extended care
costs. Recently, a large-scale NIH Trial, termed MISTIE (Minimally Invasive
Surgery Plus rtPA for Intracerebral Hemorrhage Evacuation [1,2]) whose workflow
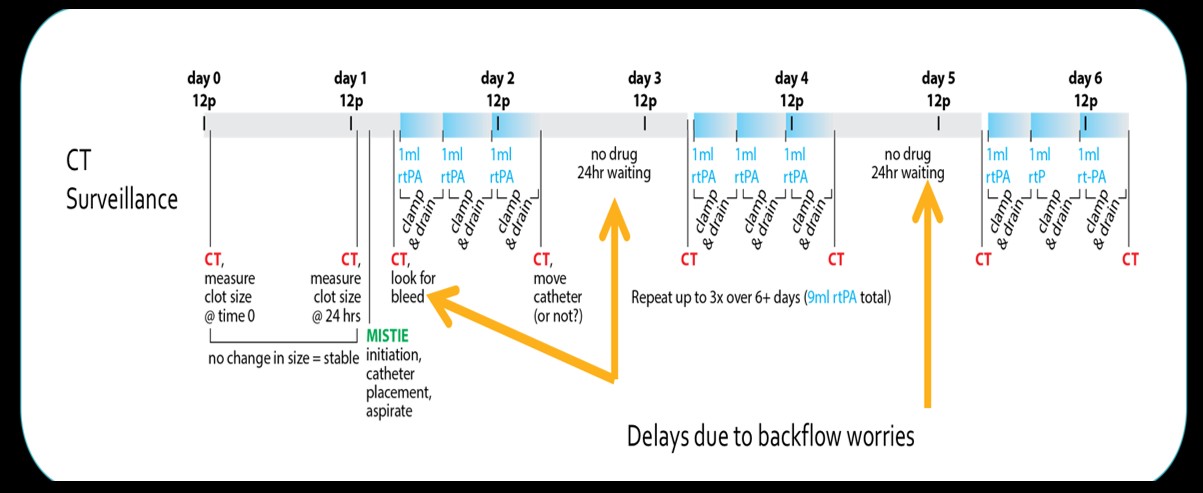
is illustrated in Figure 1, has shown promise. The procedure inserts a
minimally invasive catheter into the clot through a craniotomy, and then slowly
iterates between injecting clot-busting drugs, waiting, and draining the lysed
blood. Periodic CT surveillance (Figure
1), is used to minimize chances of a rebleed by guiding the neurosurgeon to
evacuate as much of the clot interior without disturbing the exterior shell where
the bleed originated. As CT can’t
depict the distribution of clot-busting drugs administered within the clot, the
therapy is administered slowly and iteratively in 1 ml increments every 8 hours
over 3 -5 days, as shown in Figure 1.
MRI visualizes the changing, heterogeneous distribution of plasma and fibrin-rich, semi-rigid clot regions, as shown in Fig. 2(Top). We illustrate a workflow for MR-guided clot evacuation in Figure 2(Bottom), where real-time guided plasma extraction is followed by MR-guided clot-busting. We investigate: 1) using MRI as a surveillance tool to visualize distribution of administered drugs within an ex-vivo clot and 2) attempt to achieve a more controlled distribution of the clot buster by driving the drug slowly under pressure into the clot with new catheter technology.
Methods
As MISTIE aims to evacuate only the clot interior as illustrated in Fig. 2(Bottom), simulating the interface between the clot and normal brain parenchyma is not immediately necessary. Instead significant insight can be garnered on a simple ex-vivo phantom of swine blood, consisting of blood that naturally clots and then is placed into a 5 x 5 x 7 cm clear plastic box [3].
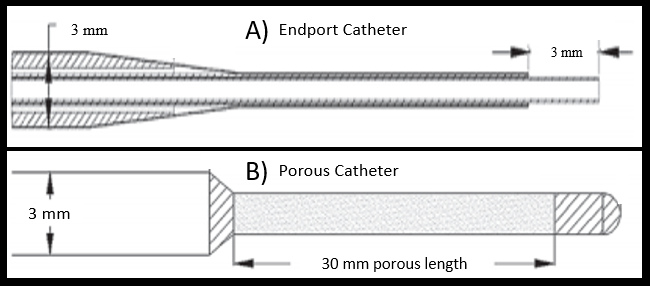
We performed experiments using different methods of drug administration: 1) manual catheter injection with a 3 mm diameter catheter simulating today’s surgical practice, 2) pressurized infusion through a 0.7 mm fused silica, single endport catheter (Engineering Resources Group, Pembroke Pines, FL), and 3) pressurized infusion through a porous catheter (invenTX, Lexington KY). Illustrations of the catheters are provided in Figure 3. The pressurized infusions aim to leverage our experience in intraparenchymal convection-enhanced delivery (CED) within the brain, a technique that bypasses the blood brain barrier by creating a bulk flow through interstitial spaces [4-6]. We hypothesize that pressurized infusions can drive clot-busting drugs deeper into the interstitial spaces in fibrin-rich clot, creating more interaction between the drug and clot than possible with the simple injections used in MISTIE today.
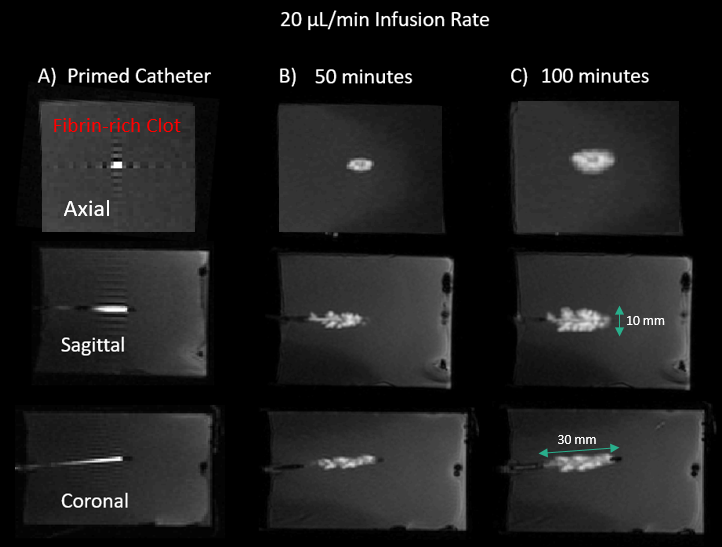
All experiments administered with 1-2 mL of a recombinant tissue plasminogen activator (rtPA) (Alteplase, Genentech) into the clot phantom. Some were co-infused with a Gd-doped buffer (2 millimolar) for simplified detection of the infusion distribution within the clot. Infusion rates of 12, 20, and 50 µL/min were tested, in accordance with moderate and high flow rates used in brain CED infusions. The porous brain infusion catheter (PBIC), originally designed for infusing chemotherapeutic drugs in the brain [7], has a 3 cm long porous region with a 1 mm diameter at its distal end, as shown in Fig. 3. The porous region consists of 10 micron pores interspersed at 50 pores/cm. The PBIC was primed and then infused at 20 µL/min until a volume of 2 mL was distributed.
Results
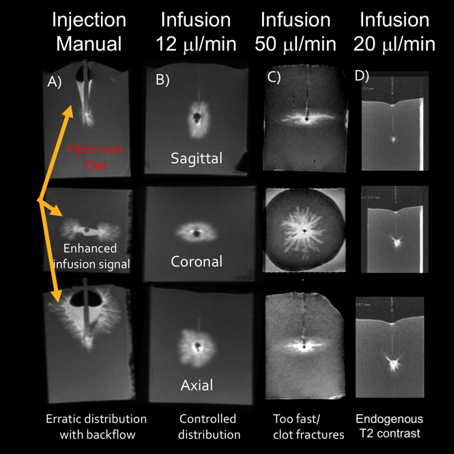
Prior to infusion, we use real-time MR guidance to aspirate plasma pockets, as depicted in Fig. 2(Bottom). Imaging of manual drug injection, shown in Fig. 4A, shows significant and possibly dangerous unwanted backflow along the exterior of the catheter. Pressurized infusions at 12 and 20 µL/min for the endport catheter showed a controlled, spherical, and much more symmetric distribution (Fig. 4B,D). The higher flow rate of 50 µL/min showed the infusate fracturing the clot, which risks lysing at unsafe locations (Fig. 4C). The porous catheter created the most desirable delivery: a constrained, ellipsoidal region along the catheter’s 3 cm axis, as shown in Fig. 5, without backflow or fracture.Conclusion
Pressurized CED infusions create more controlled distributions than the manual injection technique used by surgeons today. The porous catheter demonstrated a long, controlled, and symmetric cylindrical distribution, which can be aligned with the often ellipsoidal ICH morphology in humans. MRI’s simplified surveillance and controlled drug distribution could permit administration of higher drug doses over broader clot regions in each treatment iteration. The approach could substantially decrease treatment iterations, evacuating ICH faster while maintaining safety and improving patient outcomes.Acknowledgements
We acknowledge the support of the University of Wisconsin - Madison Radiology Research and Development fund and the technical and in kind assistance of invenTX.References
[1] W. A. Mould, J. R. Carhuapoma, J. Muschelli, K. Lane, T. C. Morgan, N. A. McBee, et al., "Minimally invasive surgery plus recombinant tissue-type plasminogen activator for intracerebral hemorrhage evacuation decreases perihematomal edema," Stroke, vol. 44, pp. 627-34, Mar 2013.
[2] D. F. Hanley, R. E. Thompson, J. Muschelli, M. Rosenblum, N. McBee, K. Lane, et al., "Safety and efficacy of minimally invasive surgery plus alteplase in intracerebral haemorrhage evacuation (MISTIE): a randomised, controlled, open-label, phase 2 trial," Lancet Neurol, vol. 15, pp. 1228-1237, Nov 2016.
[3] M. Olsen, Meudt, J, M. McCue, R. Weyker, R. Moskwa, T. Oakes, et al., "Feasibility Study of MR Image-Guided Intracerebral Clot Evacuation," in 12th Interventional MRI Symposium, Boston, 2018.
[4] R. R. Lonser, R. Schiffman, R. A. Robison, J. A. Butman, Z. Quezado, M. L. Walker, et al., "Image-guided, direct convective delivery of glucocerebrosidase for neuronopathic Gaucher disease," Neurology, vol. 68, pp. 254-61, Jan 23 2007.
[5] R. M. Richardson, A. P. Kells, K. H. Rosenbluth, E. A. Salegio, M. S. Fiandaca, P. S. Larson, et al., "Interventional MRI-guided putaminal delivery of AAV2-GDNF for a planned clinical trial in Parkinson's disease," Mol Ther, vol. 19, pp. 1048-57, Jun 2011.
[6] J. H. Sampson, R. Raghavan, J. M. Provenzale, D. Croteau, D. A. Reardon, R. E. Coleman, et al., "Induction of hyperintense signal on T2-weighted MR images correlates with infusion distribution from intracerebral convection-enhanced delivery of a tumor-targeted cytotoxin," AJR Am J Roentgenol, vol. 188, pp. 703-9, Mar 2007.
[7] M. L. Brady, R. Raghavan, J. Mata, M. Wilson, S. Wilson, R. M. Odland, et al., "Large-Volume Infusions into the Brain: A Comparative Study of Catheter Designs," Stereotact Funct Neurosurg, vol. 96, pp. 135-141, 2018.
Figures
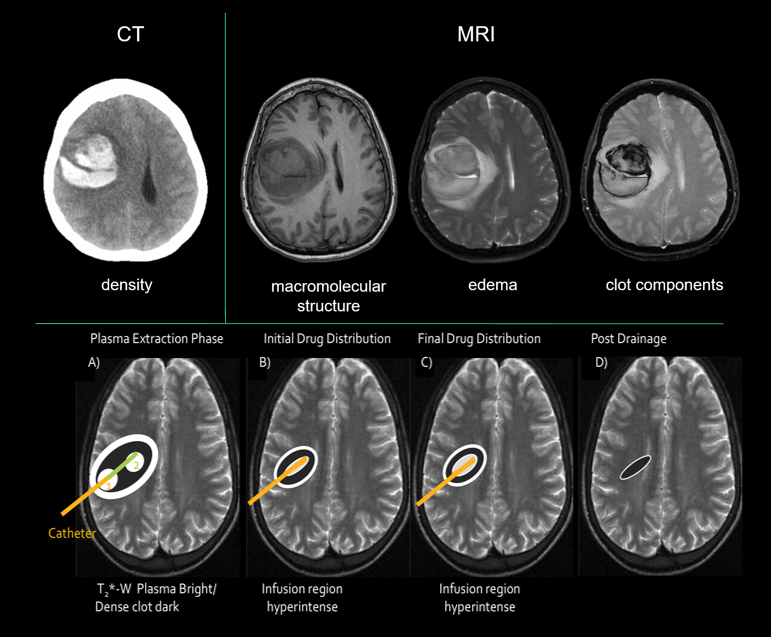
Top: CT of ICH shows little detail within clot. MRI show much more detail regarding clot components. The T2* image (far right) clearly separates fibrin-rich (top) from plasma (entire bottom half) portion of clot.
Bottom: Proposed MR-guided workflow A) Real-time MR-guided aspiration of bright plasma pockets during catheter insertion (orange line–first extraction, green line 2nd plasma extraction). B) Reduced clot volume then reduces nearby edema (white boundary), with initial depiction of drug distribution about catheter. C) MR surveillance demonstrates final rtPA infusion while safely leaving clot exterior unaffected. D) Drainage of lysed clot significantly reduces clot volume and edema.