3847
Proof-of-concept of retrospective gating for interventional cardiac MRI using catheter microcoils readings.1IHU LIRYC, PESSAC, France, 2Siemens Healthcare, Saint-Denis, France, 3Univ. Bordeaux, Centre de recherche Cardio-Thoracique de Bordeaux, Bordeaux, France, 4INSERM U1045, Bordeaux, France
Synopsis
In the context of radiofrequency ablation of cardiac arrhythmia, a catheter is inserted into the heart for contact electrophysiology recording and/or ablating the arrhythmogenic substrate. In this context, we propose to exploit MR-compatible microcoils located near the catheter tip to estimate the local motion of the heart. For this, a tracking module was interleaved with segments of a radial acquisition in a FLASH sequence. k-space segments were sorted retrospectively according to tracking readings before image reconstruction. Using this approach, artifact free images of a pig in vivo could be reconstructed.
Introduction
Conventional cardiac
MRI uses ECG and respiratory sensors (belt, navigator) to prospectively/retrospectively
compensate the cardiac and respiratory motion. In the context of radiofrequency
ablation of cardiac arrhythmia, a catheter is inserted into one or several
cardiac chambers for contact electrophysiology recording and/or ablating the
arrhythmogenic substrate [1,2]. These instruments may include position sensors
whose readings may be used to sort k-space data to improve image quality,
particularly in presence of arrhythmia where ECG may be distorted. Moreover,
respiratory compensation using navigator-based techniques may suffer from
different scaling factors between displacement of the diaphragm and actual
displacement of the heart, depending on the slice location (ex atrium vs apex)
[3]. This study presents a method that exploits MR-compatible microcoils
located near the catheter tip to retrospectively sort k-space data and retrieve
a correct image without using conventional physiological sensors or
echo-navigation. The method was evaluated in vivo in pig.Methods
After sedation of the animal and mechanical ventilation at 12
breaths/min (protocol approved by ethic committee), a 9Fr MR-compatible
steerable catheter (Vision-MR, Imricor, Burnsville, MN, USA) was inserted
through the femoral vein and navigated until it reached the right ventricle
(RV) wall close to the apex. Conventional surface ECG were used to record
cardiac rhythm of the animal (85bpm). To perform active catheter tracking
during MRI scans and determine the 3D coordinates of the micro coils, a pulse
sequence integrating a tracking module interleaved with a radial Gradient Echo
(FLASH) imaging sequence was implemented [4]. Radial acquisition was chosen for
its intrinsic robustness to motion. The active tracking sequence comprised
three non-selective projection acquisitions along the respective axis followed
by acquisition of N k-space projections (Figure 1a-b).
Imaging parameters were slice thickness=3mm, TE/TR=4.6 /24.96ms, FA
= 15°, FOV=169mm, matrix=112*112, N=3 segments per TR, radial views = 6000, TA
= 98s), interleaved with tracking data acquisitions (FOV = 450mm, 512 sampled
points, time of tracking = 24.04ms). All MRI scans were performed on a 1.5 T MR
scanner (MAGNETOM, Aera, Siemens Healthcare, Erlangen, Germany).
Following the acquisition, phase of the k-space of the tracking data
for each microcoils was analyzed and converted into relative displacement.
Directions where a dominant modulation due to cardiac and/or respiratory motion
were filtered using a low pass Gaussian filters (sigma = 9) to extract both respiratory
and cardiac motion components. Data were binned into 10 cardiac phases then
each cardiac phase was sorted into 2 respiratory motion phases. Images were then
reconstructed after Cartesian regriding and inverse Fourier transform of the
corresponding k-space data. A cine image was reconstructed by playing out the
10 cardiac phases for a fixed respiratory phase.Results
Figure 2a shows an example of raw signals derived from the most distal microcoil of the catheter on X and Y axes. From these signals, cardiac and respiratory motion were extracted through filtering Figure 2b. The resulting respiratory rate was 12.8 breath/min and ECG 87 bpm, consistent with ventilator frequency and ECG readings (around 85 bpm). Figure 3 displays the segmentation of signals in Figure 2b in 2 respiratory and 10 cardiac phases. As a result, between 246 to 492 projections were combined together to create each image. Figure 4 displays each image at different cardiac phase reconstructed from the proposed method for one respiratory state (Figure 5 is an animated gif of images of Figure 4). A good image quality is obtained with contraction-relaxation of the myocardium.Discussions and conclusions
This proposed retrospective gating method exploits intra-cardiac position sensors integrated into the catheter. The time penalty introduced by the tracking module appears acceptable (around 20 ms). Although the results presented here show image quality with 3 segments per TR, the sequence implementation offers flexibility between tracking update time and the number of segments acquired between two consecutive tracking modules. Such a method relies on local measurement of displacement of the catheter during cardiac contraction and respiration. Thus it is expected to provide alternative means for retrospective image reconstruction in presence of arrhythmia where conventional ECG and navigator-based approaches may fail. The method has been implemented on a radial gradient echo image acquisition for proof of concept but may be extended to other acquisition sequences.Acknowledgements
References
[1] Grothoff, Matthias, et al. "Magnetic resonance imaging guided transatrial electrophysiological studies in swine using active catheter tracking–experience with 14 cases." European radiology 27.5 (2017): 1954-1962
[2] Mukherjee, Rahul K., et al. "Epicardial electroanatomical mapping, radiofrequency ablation, and lesion imaging in the porcine left ventricle under real-time magnetic resonance imaging guidance—an in vivo feasibility study." EP Europace (2017).
[3] Roujol, Sébastien, et al. "Characterization of respiratory and cardiac motion from electro-anatomical mapping data for improved fusion of MRI to left ventricular electrograms." PloS one 8.11 (2013): e78852.
[4] Homagk, Ann‐Kathrin, et al. "An expandable catheter loop coil for intravascular MRI in larger blood vessels." Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine 63.2 (2010): 517-523.
Figures
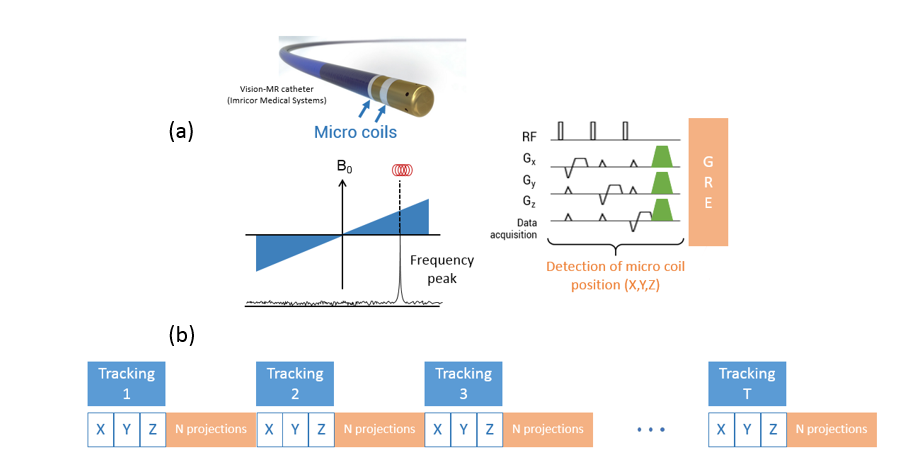
Figure 1. Schematic of the Pulse Sequence used and acquisition pattern.
(a) Integration of a Tracking module inside a Gradient Echo sequence for retrospective gating. Before the acquisition of N radial k-space projections, a nonselective excitation followed by the acquisition of Projection data is applied for each axis (X,Y,Z) to determine the position of the catheter.(b)One tracking module gives acces to the positions in which the N projections were acquired.
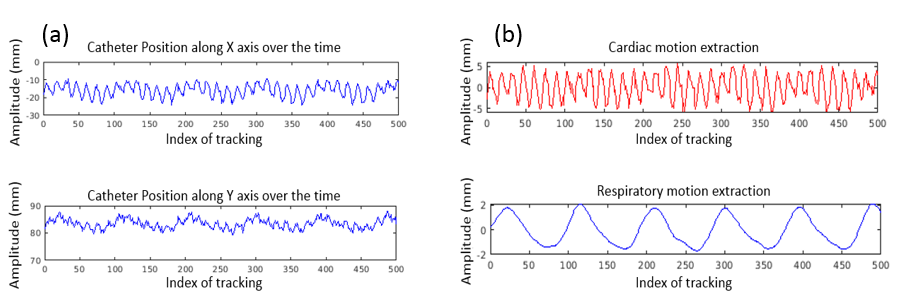
Figure 2. Extraction of cardiac and respiratory motion from recorded micro coils signal.
(a) Signals of micro coils recorded along X and Y axes. (b) Filters are then used to demodulate both motion components. For better visualization, only the first 500 tracking data are showed.
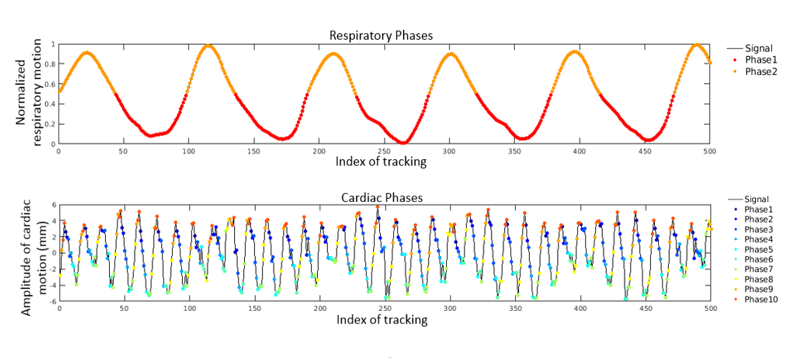
Figure 3. Extraction of cardiac phases-respiratory phases and sorting of the data.
2 respiratory phases and 10 cardiac phases are selected from the respiratory and cardiac motion signals. For better visualization, only the first 500 tracking data are showed.
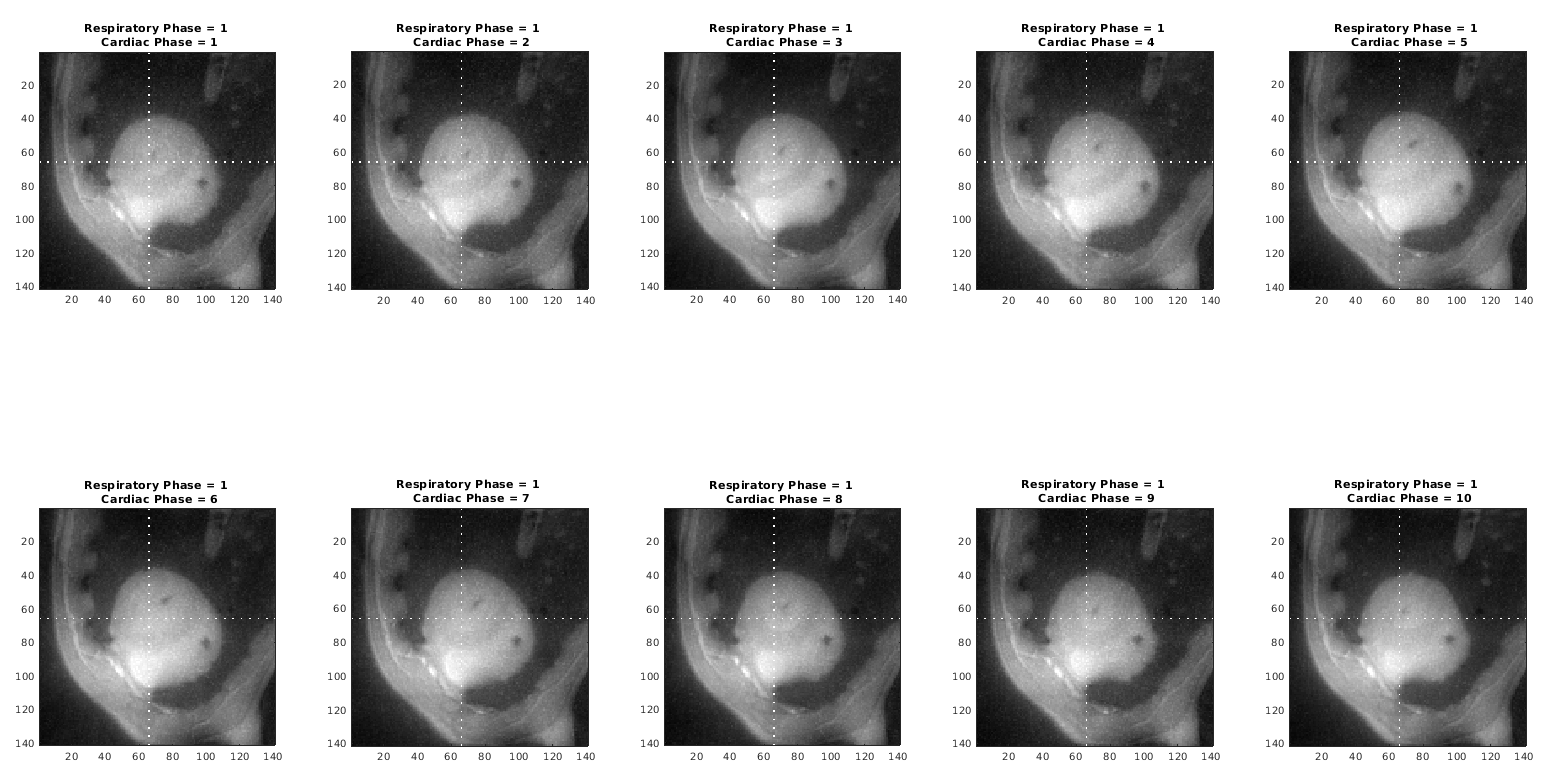
Figure 4. Reconstruction of 10 cardiac phases for a fixed respiratory phase (phase 1).
The dashed White axis enables to see the tip of the catheter displacement throughout the cardiac contraction. A gif has been done to make a cine of this 10 images.
Figure 5. Cine of the 10 respiratory cardiac phases at a fixed respiratory phase (phase 1).
It is possible to see the contraction of the myocardium and the catheter tip displacement with the contraction.