3846
Clinical MRI-guided right heart catheterization with standard metallic devices using a high performance 0.55T system1Cardiovascular Branch, Division of Intramural Research, National Heart, Lung, and Blood Institute, National Institutes of Health, Bethesda, MD, United States
Synopsis
MRI-guidance of invasive cardiovascular procedures has been limited by the unavailability of safe devices. Most cardiovascular procedures require long conductive devices (eg. guidewires and catheters) that are susceptible to RF-induced heating. Because heating is related quadratically to field strength, we propose to reduce the MRI field strength to 0.55T. Using a custom high-performance 0.55T MRI system, we performed MRI-guided catheterizations on patients with commercial metallic guidewires using standard high flip angle bSSSP real-time imaging to produce good image quality and contrast without RF-induced heating. Low field MRI combined with high-performance hardware will be fundamentally enabling for MRI guidance of invasive procedures.
Introduction
MRI guidance of invasive cardiovascular procedures has been impeded by the unavailability of MRI safe and visible devices. Safety is especially problematic for long conductive devices such as guidewires and braided catheters, which generate substantial RF-induced heating during real-time imaging. MR-guided right heart catheterization has been performed at numerous centers using only polymer catheters[1-4]. In previous work we have demonstrated modified low RF duty cycle pulse sequences, such as gradient echo spiral imaging, to enable procedural guidance with metallic devices in patients [5]. In this work, we show that imaging using a high-performance 0.55T system can significantly reduce heating of metallic devices, while still generating high quality images, which is fundamentally enabling for interventional MRI. We use this system to perform for MRI-guided catheterization in patients with commercial conductive guidewires.Methods
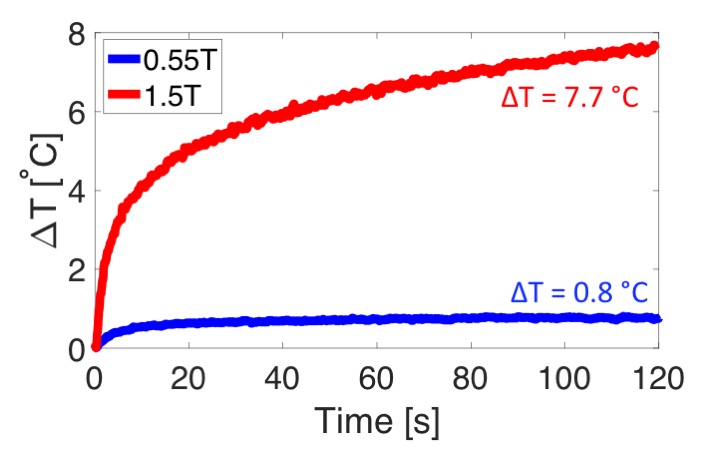
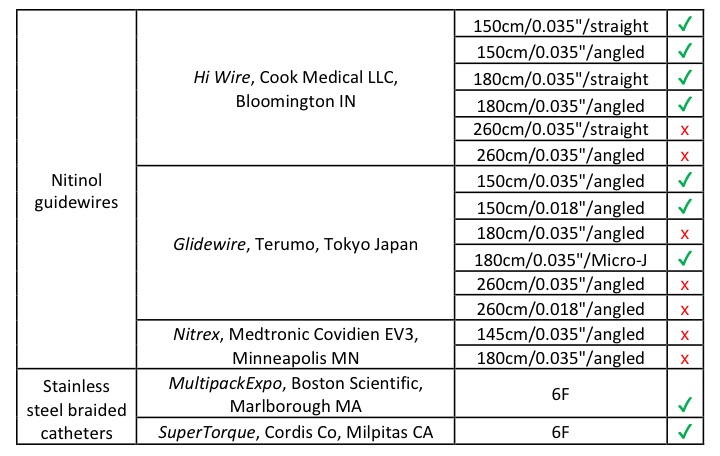
A commercial MRI system was modified to operate at 0.55T (MAGNETOM Aera, Siemens Healthcare, Erlangen Germany). This system was equipped with high performance shielded gradients (45mT/m maximum amplitude and 200T/m/s maximum slew rate) for real-time imaging. Because RF power is quadratically related to field strength, this 0.55T MRI system reduces heating by a factor of 7.4X compared to a conventional 1.5T MRI system, and 29.7X compared to a conventional 3T MRI system. Heating was evaluated for standard commercial guidewires and stainless steel braided catheters according to ASTM 2182. A total of 16 devices were assessed on this custom MRI system.
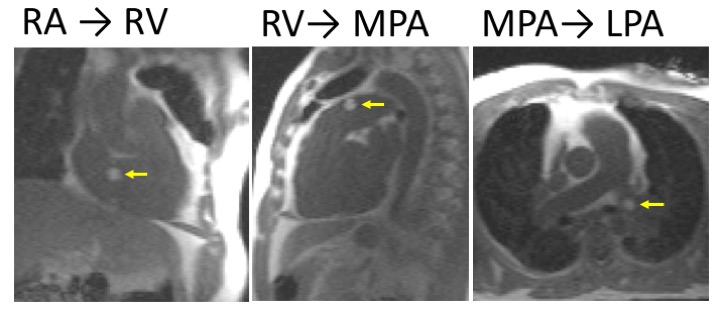
This study was approved by the NIH institutional review board. For our clinical study we used a commercial Glidewire (180cm/0.035”, 1.5mm “Micro J” tip, Terumo, Tokyo, Japan) paired with a balloon wedge catheter (“T” tip, Edwards, Irvine, CA) with gadolinium filled balloon to perform MRI guided right heart catheterization in 7 patients. The guidewire was used, as in a traditional catheterization laboratory, to augment catheter navigation when required, most commonly to navigate from the inferior vena cava to superior vena cava and to navigate the pulmonary vasculature.
Importantly, standard high flip angle Cartesian bSSFP imaging was used for real-time procedural guidance in patients using the selected guidewire (TE/TR = 2/4ms, flip angle = 45°, FOV = 400mm, slice thickness = 8-24mm, matrix = 160x144, GRAPPA acceleration factor = 2, temporal resolution = 288ms). A partial saturation pulse [6] (flip angle = 60°) was used to visualization the gadolinium filled balloon.
Simultaneous invasive pressure and cardiac function was measured at baseline and during physiological provocation (eg. nitric oxide) [7]. Cardiac cines were generated using a real-time acquisition with retrospectively cardiac binning and motion correction [8] and cardiac output was measured using standard ECG-gated gradient echo phase contrast flow.
Results
Heating at the tip of a standard clinical guidewire was reduced to 0.8°C at 0.55T, compared to 7.7°C on a standard 1.5T MRI system (Figure 1). Of the 16 devices tested, 9 generated < 1°C heating during 2 minutes of high RF duty cycle imaging (flip = 65° and TR = 2.5ms), and therefore may be suitable candidates for application for clinical MRI guided procedures at 0.55T (Table 1), but were all unsafe under these imaging conditions at 1.5T.
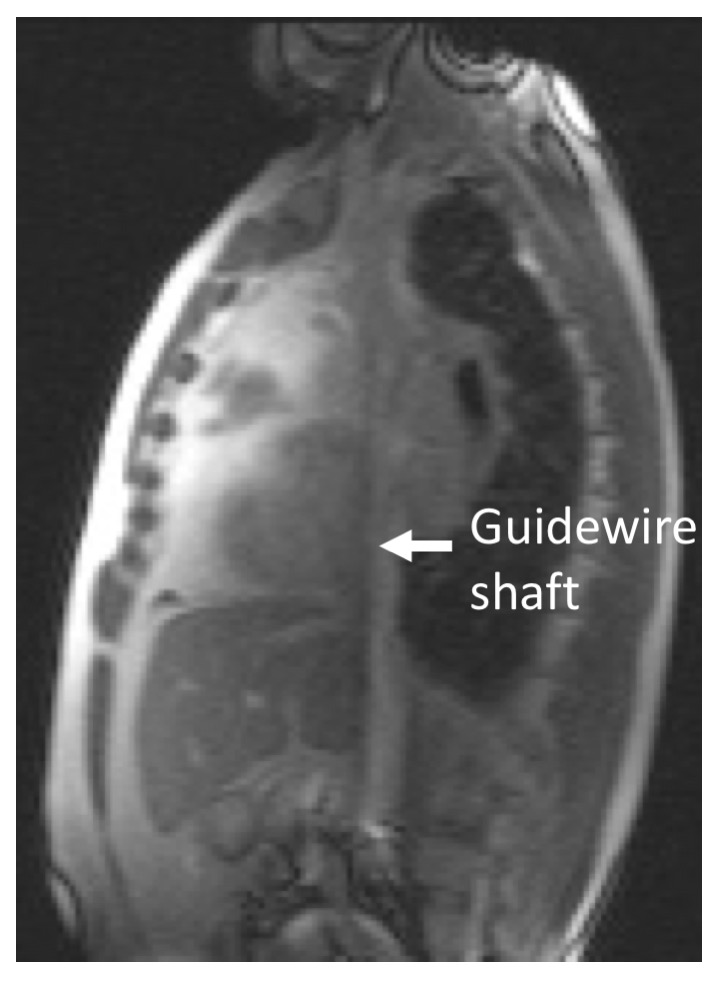
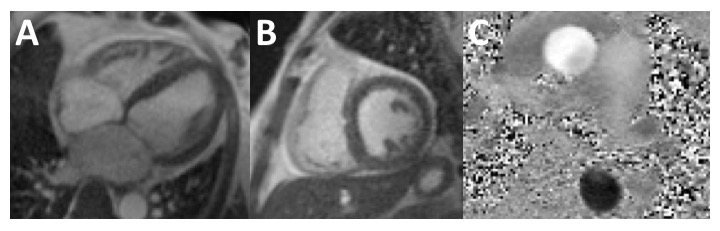
The MRI-guided right heart catheterization was successful in all patients (Figure 2) and there were no safety events in any subject. The guidewire imparted catheter stiffness that was useful for procedural navigation. When located within the catheter shaft, the guidewire generated some useful susceptibility artifact (Figure 3), but conspicuity was reduced when the guidewire exited the catheter shaft.
Despite lower field strength, cardiac image quality was sufficient, and in some cases superior, and allowed for the necessary intraprocedural measurements (Figure 3).
Discussion
Compared to our previous studies in which we modified our imaging parameters to lower RF power to enable the use of metallic tools for MRI procedures, in this study, we used a custom 0.55T MRI system such that a subset of metallic devices are inherently safe with standard real-time imaging. Some devices, for example long devices (260cm) and devices with exposed metallic tip, were found to be unsafe even at 0.55T, and careful safety testing will be required to catalog standard interventional devices at this field strength.
The maintained gradient performance of this custom 0.55T MRI system is critical for fast real-time imaging. The ability to use the commercially available catheterization tools commonly used in the X-Ray catheterization lab during MRI imaging without modification of imaging parameters is fundamentally enabling for MRI-guided cardiovascular procedures and may substantially increase the range of procedures possible under MRI guidance.
Conclusion
The transition to high-performance low field imaging could allow for an increased number of MRI-guidance of invasive procedures using metallic devices with standard imaging.Acknowledgements
This work was supported by the Division of Intramural Research, National Heart, Lung, and Blood Institute, National Institutes of Health, USA (Z01-HL005062, Z01-HL006061, Z1A-HL006213)References
- Rogers, T., et al., CMR fluoroscopy right heart catheterization for cardiac output and
pulmonary vascular resistance: results in 102 patients. J Cardiovasc Magn
Reson, 2017. 19(1): p. 54.
- Ratnayaka, K., et al., Radiation-free CMR diagnostic heart catheterization in children. J Cardiovasc Magn Reson, 2017. 19(1): p. 65.
- Pushparajah, K., A. Tzifa, and R. Razavi, Cardiac MRI catheterization: a 10-year single institution experience and review. Interventional Cardiology, 2014. 6(3).
- Razavi, R., et al., Cardiac catheterisation guided by MRI in children and adults with congenital heart disease. Lancet, 2003. 362(9399): p. 1877-82.
- Campbell-Washburn, A.E., et al., Right heart catheterization using metallic guidewires and low SAR cardiovascular magnetic resonance fluoroscopy at 1.5 Tesla: first in human experience. J Cardiovasc Magn Reson, 2018. 20(1): p. 41.
- Velasco Forte, M.N., et al., Improved passive catheter tracking with positive contrast for CMR-guided cardiac catheterization using partial saturation (pSAT). J Cardiovasc Magn Reson, 2017. 19(1): p. 60.
- Rogers, T., K. Ratnayaka, and R.J. Lederman, MRI catheterization in cardiopulmonary disease. Chest, 2014. 145(1): p. 30-6.
- Xue, H., et al., Distributed MRI reconstruction using gadgetron-based cloud computing. Magn Reson Med, 2014.
Figures