3844
Real-time Automatic Tip Tracking of Gadolinium-filled Balloon Wedge Catheter during MR-guided Cardiac Catheterization1Biomedical Engineering Department, School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2MR Research Collaborations, Siemens Healthcare Limited, Frimley, United Kingdom
Synopsis
MRI-guided cardiac catheterisation procedures are commonly performed using balloon wedge catheters which are currently manually tracked. Furthermore, these procedures require frequent manual adjustment of the slice positioning during catheter navigation. In this study, we sought to develop a novel acquisition and reconstruction framework that enables automatic tracking of a gadolinium-filled balloon wedge catheter using (a) real-time partial saturation with increased spatial coverage, (b) automatic image-based estimation of the catheter balloon position, and (c) real-time slice tracking. The proposed framework is demonstrated during an MRI-guided cardiac catheterisation experiment in a 3D printed heart phantom.
Purpose
MRI is a promising alternative to X-ray fluoroscopy for the guidance of cardiac catheterization procedures as it provides high soft tissue contrast and superior hemodynamic data with the absence of ionizing radiation1-3. Current approaches commonly use a gadolinium (Gd)-filled catheter balloon and require frequent manual slice tracking to follow the catheter balloon during catheter navigation. In this study, we sought to develop a novel passive tracking sequence that enables automatic real-time catheter balloon tracking and slice tracking to ensure continuous balloon visibility of the Gd-filled catheter balloon during catheter navigation.Methods
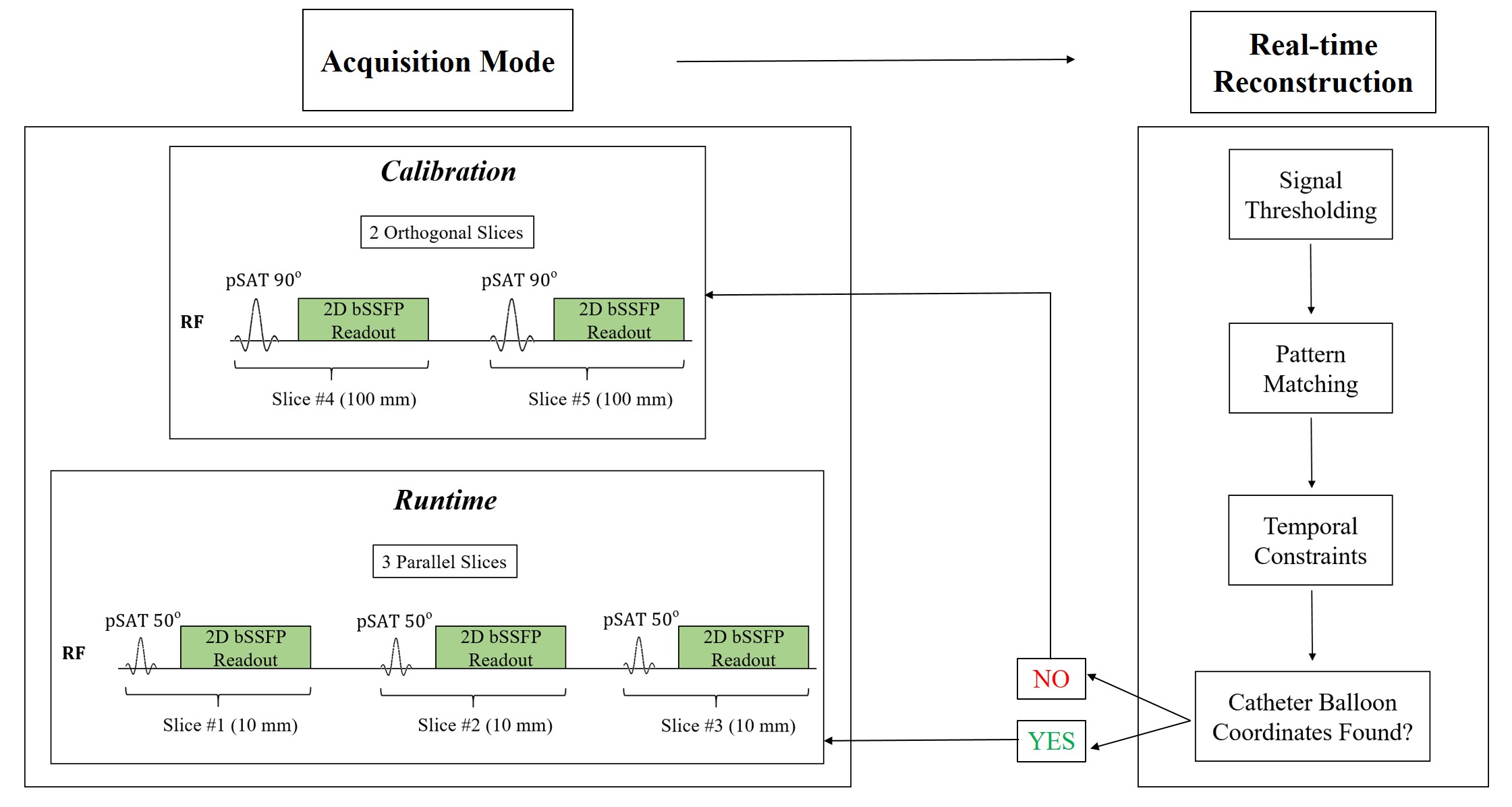
Proposed framework: The proposed prototype sequence (Figure 1) contains two imaging modes, denoted by Calibration and Runtime. In the Calibration mode, two thick orthogonal slices (100 mm) are used with a large pSAT angle to identify the catheter balloon coordinates within the entire field of view (FOV) using intensity thresholding and pattern matching. After the Calibration phase, the sequence automatically switches to the Runtime mode where three parallel slices of regular slice thickness (10mm) are continuously acquired using a lower pSAT angle of 30-50o to enable simultaneous visualisation of the catheter balloon and the cardiovascular anatomy4. The central slice is initially positioned based on the 3D balloon coordinates estimated from the Calibration phase. During the Runtime mode, the catheter balloon coordinates are estimated from the set of three images using signal intensity thresholding, pattern matching, and temporal constraints. The position of these three slices is automatically adjusted to always maintain the balloon in the central slice. The sequence switches back to the Calibration mode if the balloon is not detected during Runtime.
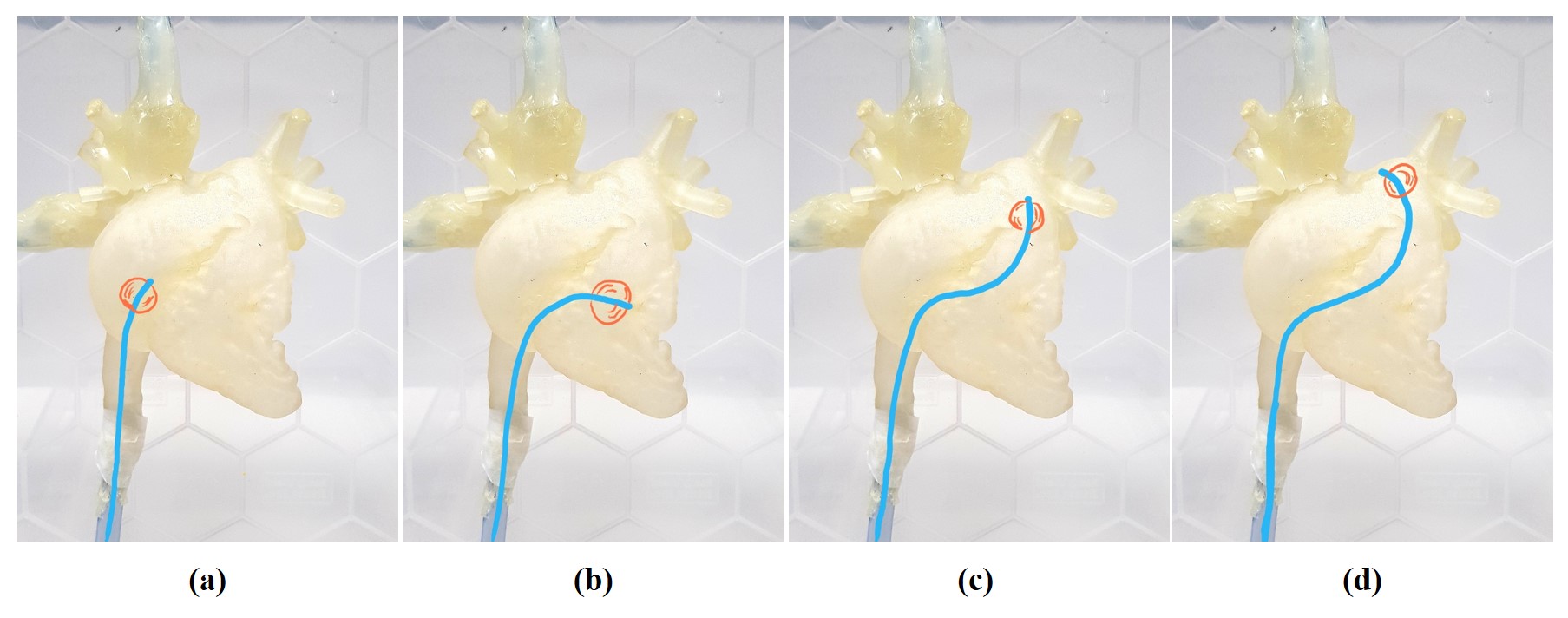
Experimental validation: Phantom experiments were conducted on a 1.5 T MRI scanner (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany). The proposed sequence employs a 2D single-shot acquisition with a balanced Steady State Free Precession (bSSFP) readout: TR/TE=2.6/1.36 ms, flip angle=67o, 300x300 mm2 FOV, 2.3x2.3 mm2 resolution, shot-length=191 ms, bandwidth=1000 Hz, GRAPPA factor=2, partial Fourier=0.62. 1% gadolinium (Dotarem®) was used to fill the balloon of the wedge catheter (Arrow®) for positive contrast visualization. The two orthogonal slices were prescribed in coronal and sagittal orientations and remained fixed during the procedure. To demonstrate the benefit/robustness of the proposed approach, the three Runtime slices were prescribed in the transverse orientation, which is subject to important through-plane catheter displacement during navigation. The entire setup was tested using a 3D-printed heart phantom (Figure 2), where a baseline catheterisation routine was performed (catheter navigation from the inferior vena cava (IVC) to the right atrium, right ventricle, and pulmonary artery).
Results
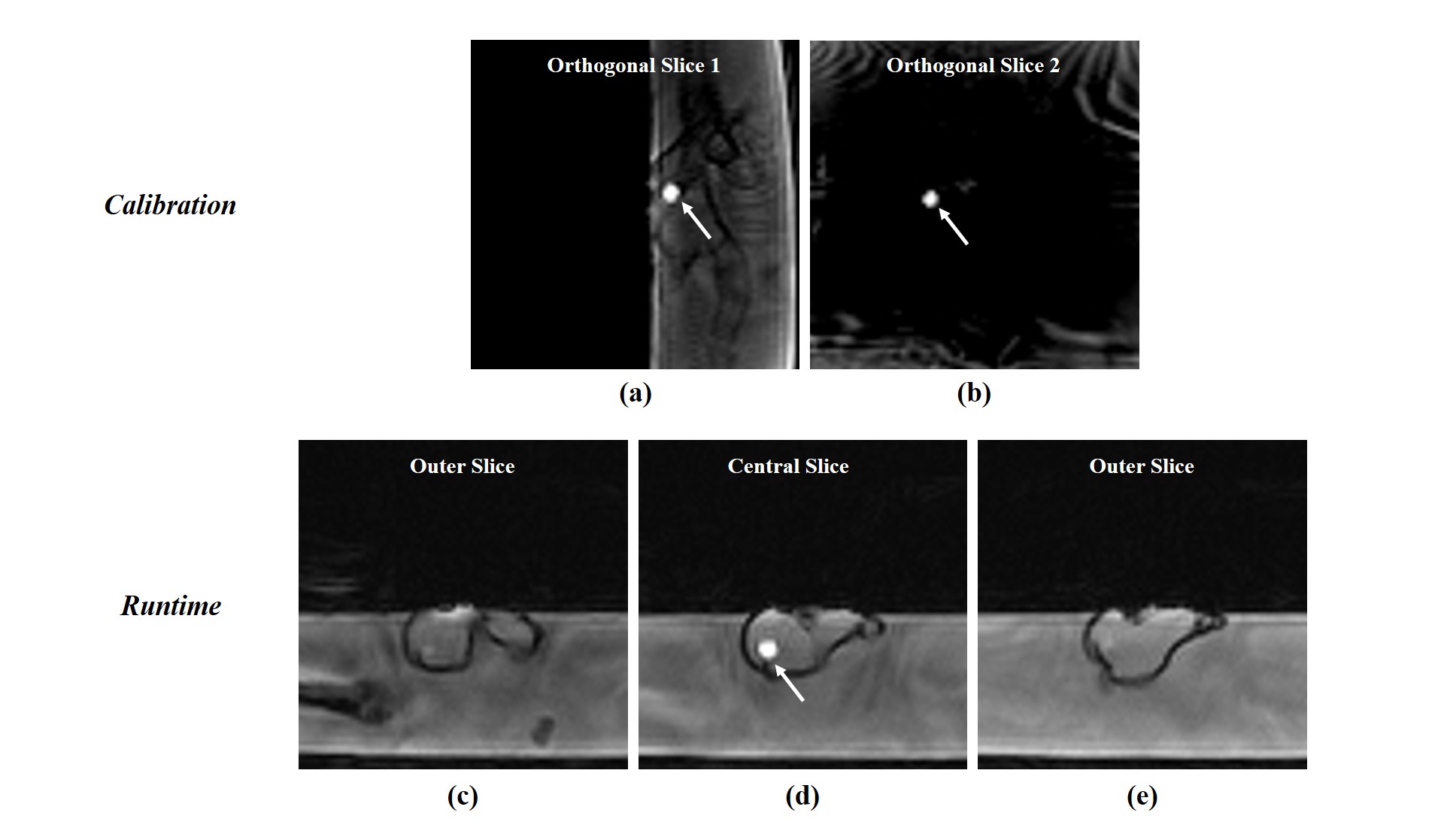
In Figure 3, the still frames show the catheter balloon position as it was moved through the 3D printed heart phantom. Figures 3(a) and (b) depict the two thick orthogonal slices from the Calibration mode in the sagittal and coronal orientations, respectively, that estimated the initial balloon location. Figures 3(c)-(e) show the three parallel slices acquired in the transversal plane during the Runtime mode as the catheter was moved by the operator.
Figure 4 depicts the animation of the proposed framework as the catheter was successfully tracked automatically from the IVC to the pulmonary branches via the route described earlier. Real-time slice tracking ensured continuous visibility of the catheter balloon. In some instances the balloon fell out of plane or could not be identified and an automatic switch between the Runtime and Calibration modes enabled an accurate re-estimation of the new balloon location. During this baseline catheterisation step, the sequence was in Runtime mode for 92.1% of the time and in Calibration mode for 7.9% of the time. The catheter was visible in 96.1% of all dynamics.
Discussion
Manually-controlled catheter navigation is operator-dependent and diverts the operator’s focus from driving the catheter to the targeted anatomies. The proposed automatic tracking framework may overcome these limitations and has the potential to offer a more robust guidance approach. Translation of this technique to in-vivo will require further developments to ensure robust estimation of the catheter balloon location in the presence of additional confounding bright signal (fat, artifacts, etc).Conclusion
A novel passive tracking sequence has been developed to ensure automatic and reliable tracking of a Gd-filled catheter balloon, while maintaining a high contrast balance between the catheter and the cardiovascular system.Acknowledgements
This work was supported by the EPSRC grant (EP/R010935/1) and the Health Innovation Challenge Fund (grant number HICF-R10-698), a parallel funding partnership between the Department of Health, and the Wellcome Trust. This work was also supported by the Wellcome EPSRC Centre for Medical Engineering at Kings College London (WT 203148/Z/16/Z) and by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health.References
1. Razavi R, Hill DL, KEEvil SF, et al. Cardiac catheterization guided by MRI in children and adults with congenital heart disease. Lancet. 2003;362(9399):1877-1882.
2. Pushparajah K, Chubb H, Razavi R. MR-guided Cardiac Interventions. Top Magn Reson Imaging. 2018;27(3):115-128.
3. Ratnayaka K, Faranesh AZ, Hansen MS, et al. Real-time MRI-guided right heart catheterization in adults using passive catheters. Eur Heart J. 2013;34(5):380-389.
4. Velasco Forte MN, Pushparajah K, Schaeffter T, et al. Improved passive catheter tracking with positive contrast for CMR-guided cardiac catheterization using partial saturation (pSAT). J Cardiovasc Magn Reson. 2017;19(1):60.
Figures