3838
Ten Minutes for the Brain to Settle: an In-vivo Investigation of Positional Brain Shift1Computer Science and Informatics, Cardiff University, Cardiff, United Kingdom, 2School of Engineering, Cardiff University, Cardiff, United Kingdom, 3Cardiff University Brain Research Imaging Centre, Cardiff University, Cardiff, United Kingdom
Synopsis
Positional brain shift (BS), as the physiological sagging of the brain under the effect of gravity, has a magnitude that is comparable to the accuracy of neuronavigational systems. It is a complex interaction of gravity, anatomical boundaries and tissue mesostructure. A comprehensive investigation of such deformation is needed. This study aims to provide a rich set of volumetric measures to infer the pattern of deformation as well as the time evolution of positional BS. Results show that positional BS is a relatively fast process, stabilised in 10 minutes, with local variations strongly dependent on the variability of anatomical structures between different subjects.
Introduction
Image-guided neurosurgical systems (IGNS) are commonly used for treatments involving deep brain stimulation, local drug delivery and biopsy. Pre-operative planning is an essential element of IGNS. A key aspect is the accurate localisation of a target. Procedurally, this involves registering the pre-operative scans to the surgical space by estimating a rigid transformation1. However, being a soft tissue, the brain sags against the skull non-uniformly under the effect of gravity (positional brain shift (BS)). Such a non-linear deformation is not accounted for in current IGNS systems, making the location of the target structure differ from the one planned1-6,8,9,11-13. Mechanics-driven elastic registration can predict such complex deformation field, increasing target accuracy. To the best of our knowledge, there is no comprehensive study of positional BS on a volumetric scale. This information is critical for surgery to accurately deliver treatment to the target area. Furthermore, knowledge of BS time-course is hugely beneficial in routine neuroimaging studies, considering possible artefact caused by positional BS in particular when acquiring high-resolution MR images.
Method
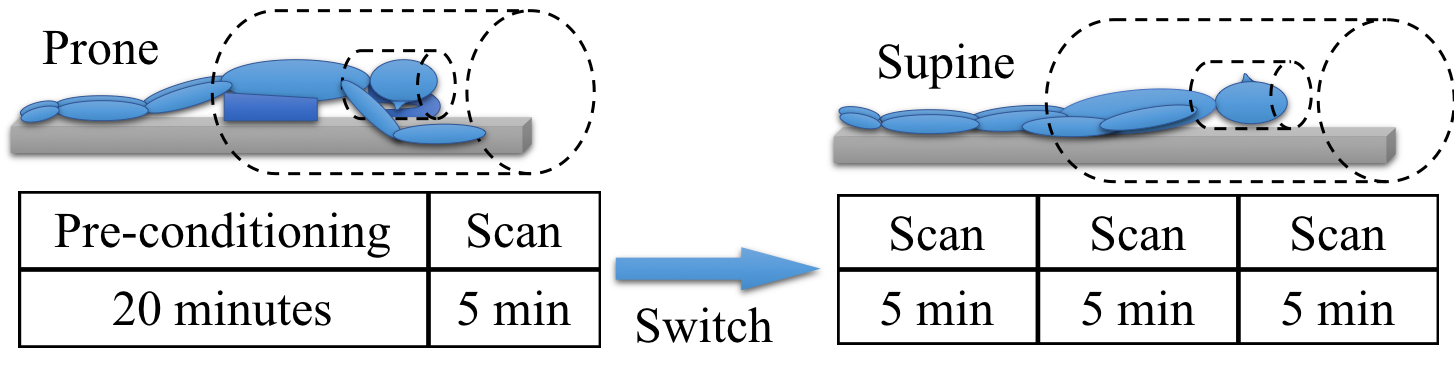
Eight healthy participants (5 male and 3 female, average age resulted 25 years) were scanned in supine and prone positions in order to measure the maximum BS. The scanning protocol, depicted in Figure 1, was defined in order to extract the time evolution of positional BS. Structural T1w scans were acquired from the same Siemens 7T MAGNETOM scanner (TE=2.93ms, TR=2200ms, FOV=256x318 over 242 slices, resolution=~0.83mm). Affine registration using FLIRT from FSL14 was used to align the skulls from all the scans of a subject, so that positional BS remained the only difference left in the scans. Elastic registration (DRAMMS10) of consecutive scans determined the overall deformation field and the time evolution of BS. Images were elastically registered to the MNI152 standard space15 for the group analysis, where each vector of the displacement field was reoriented accordingly. The Harvard Oxford16 and the ATAG7 labelled atlases were used to infer the deformation at the gray matter, white matter, ventricles and subthalamic nucleus.
Results
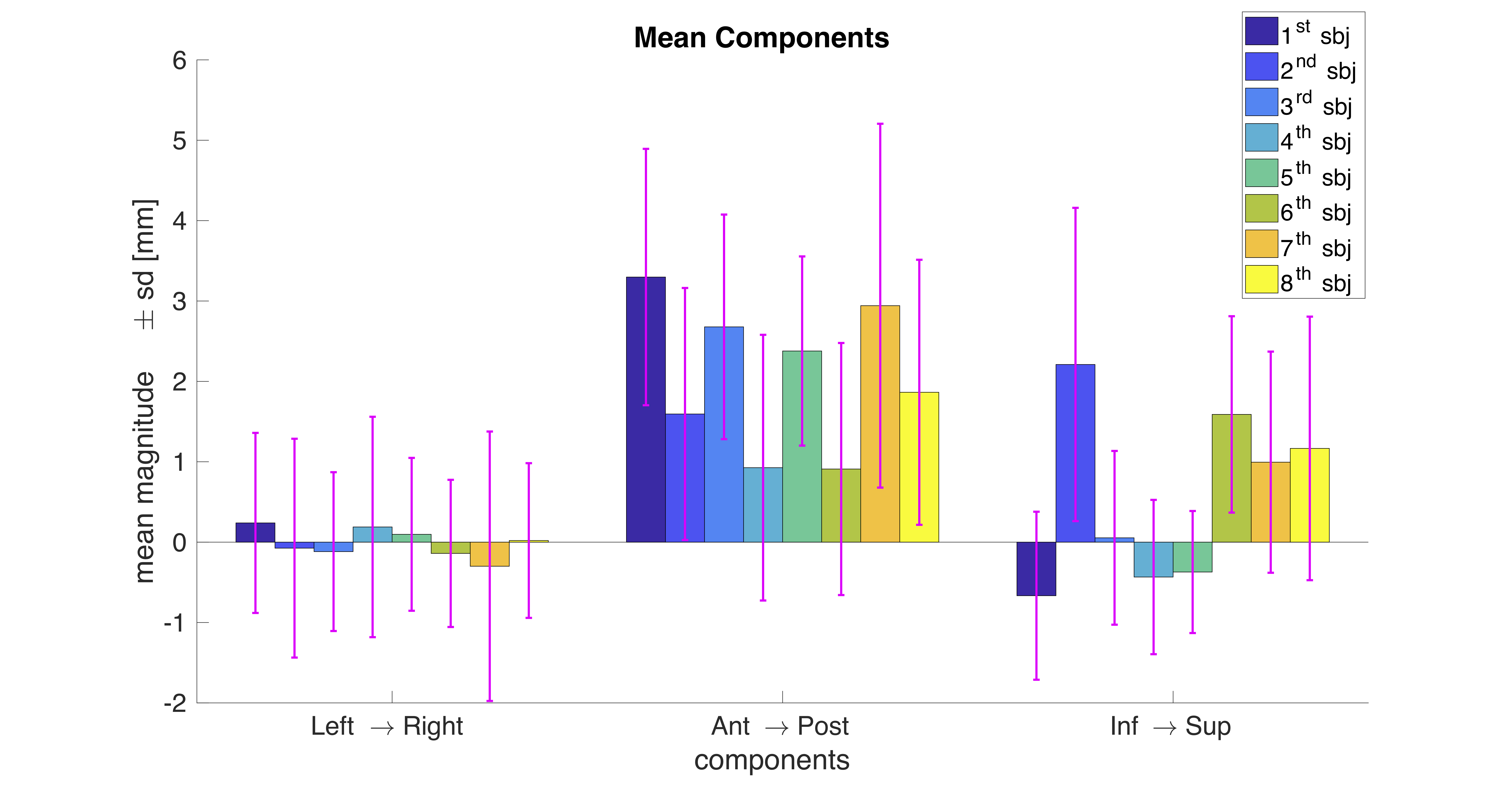
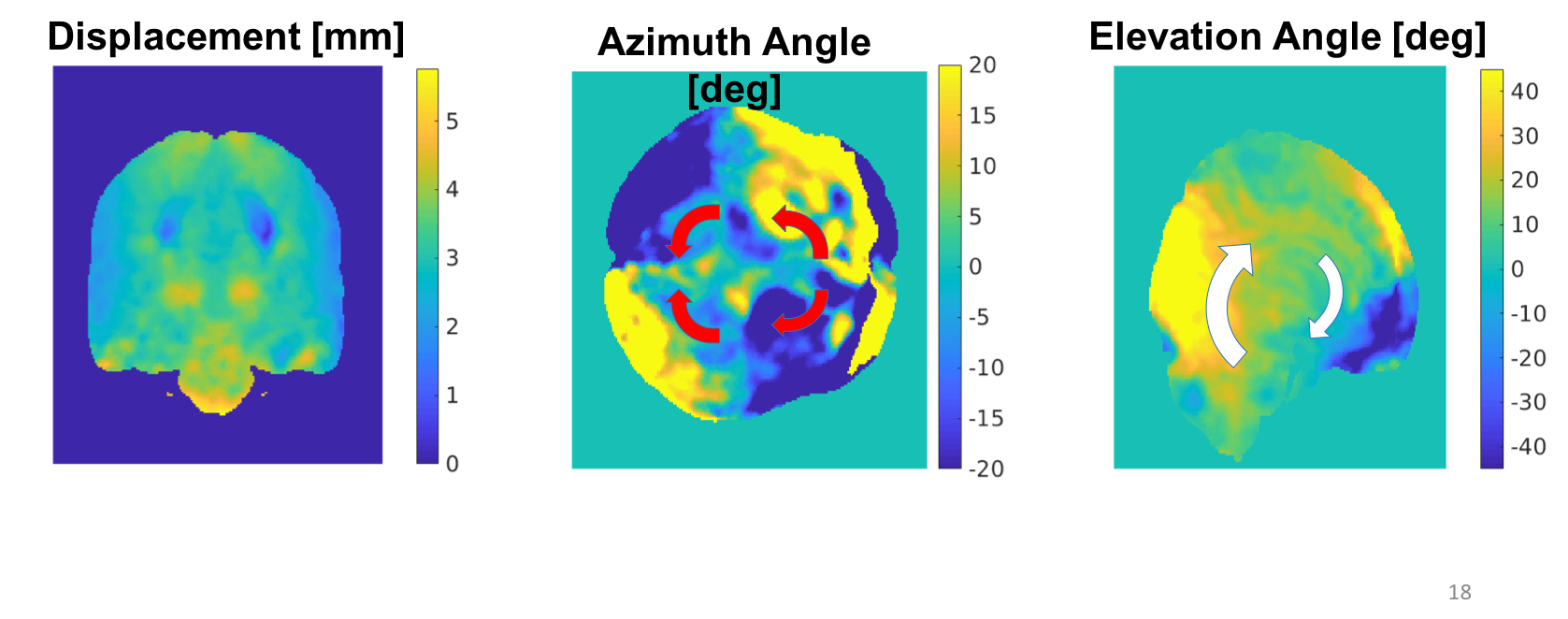
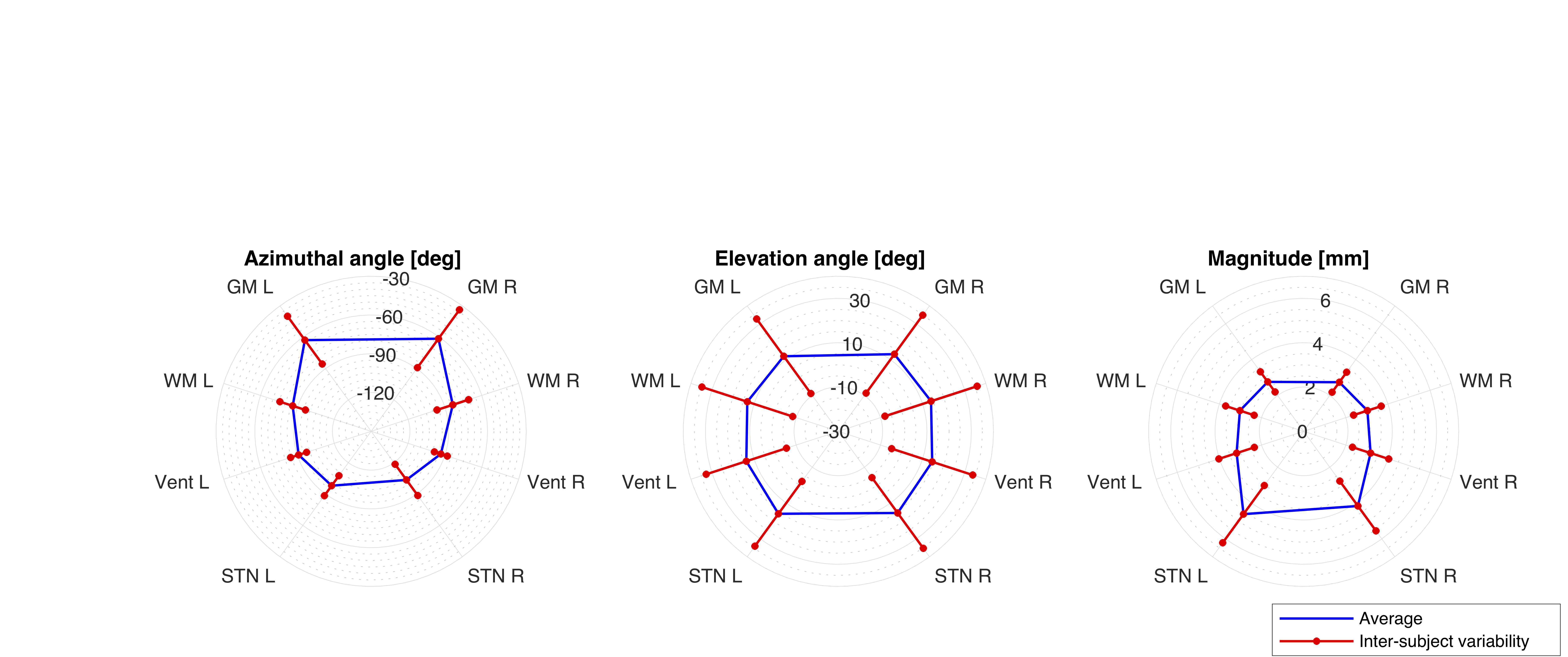
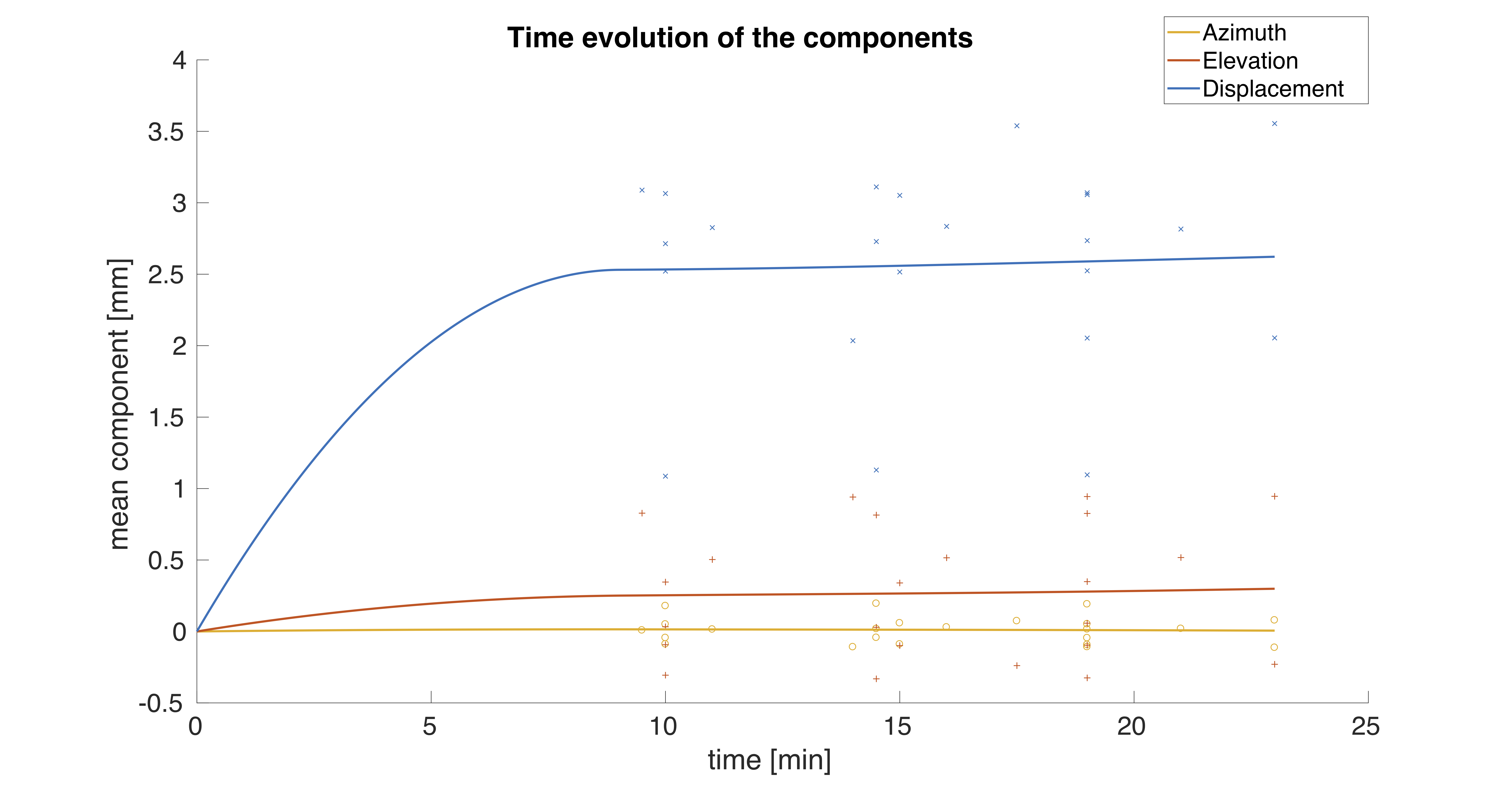
The protocol successfully quantified positional BS, finding an average magnitude around 1.6 mm over all subjects. The largest BS occurred along the anterior to posterior direction, as reported in Figure 4. High inter-subject variability was observed in the inferior-superior direction. The volumetric analysis showed numerous local variations, that resulted to be related to the local anatomy, as can be seen in the magnitude values reported in the coronal slice of Figure 3. On an axial plane, positional BS showed an outward deformation in the frontal lobes of the anterior cranial fossa, whereas an inward displacement was seen at the occipital lobes. On a sagittal plane, a general rotational component can be noted, with lower values near to deep structures of the brain. The ROI-analysis showed grater deformation of deeper structures, with displacement reaching approximately 4 mm at the subthalamic nucleus. Regarding the time evolution, positional BS stabilised in around 10 minutes, as can be seen in Figure 5. The time taken to perform shimming meant that no images could be acquired before 8 minutes.
Discussion
The measurements obtained here are consistent with previous studies in terms of average magnitude and pattern of deformation9,13. Greater displacement was observed in the internal structures of the brain (i.e. basal ganglia) where gravity has the greatest influence. On the other hand, the closer to the surface of the brain area, the greater the influence of anatomical boundaries, such as the skull, falx, tentorium and brainstem. These introduce a rotational component in particular on a sagittal plane3,9,12,13. Furthermore, their anatomical variability between subjects may explain the inter-subject variability of the inferior-superior component previously noted. The results about the time evolution indicate that, given that the head of the patient is kept in the same position as in the pre-operative scans, positional BS may not cause the target structure to displace from its planned position. However, when the head orientation differs from the one imaged, the displacement caused by positional BS may affect the accuracy of the surgical planning. Furthermore, the study shows the neuroimaging community the time needed for the brain to settle down and not cause any motion artefact (in the case of high resolution imaging systems).
Conclusion
The study has shown that positional BS is a complex interaction of gravity, anatomical boundaries and tissue mesostructure. Indeed, the dimension of positional BS was found to be comparable with the accuracy of IGNS systems, indicating that BS should be taken into account when the orientation of the patient's head on the surgical table differs from the one imaged. Indeed, the volumetric data extracted can be critical for an accurate validation of the mechanics-driven registration from BS prediction.Acknowledgements
We thank Dr. John Evans and all the MR staff at CUBRIC for their help with the setting up of the protocol and the following data acquisition.
The authors have no conflicts of interest to disclose.
References
1. Ian J. Gerard et al. Brain shift in neuronavigation of brain tumors: A review. 2017. doi: 10.1016/j.media.2016.08.007.
2. W Jeffrey Elias, Kai-Ming Fu and Robert C Frysinger. “Cortical and subcortical brain shift during stereotactic procedures.” In: Journal of neurosurgery 107.5 (2007), pp. 983–988. issn: 1933-0693. doi: 10.3171/jns.2007.107.5.983.
3. Y. Feng et al. “Relative brain displacement and deformation during constrained mild frontal head impact”. In: Journal of the Royal Society Interface 7.53 (2010), pp. 1677–1688. issn: 17425662. doi: 10.1098/rsif.2010.0210. url: http://rsif.royalsocietypublishing.org/content/7/53/1677.
4. Prashanth Dumpuri et al. “An atlas-based method to compensate for brain shift: Preliminary results”. In: Medical Image Analysis 11.2 (2007), pp. 128–145. issn: 13618415. doi: 10.1016/j.media.2006.11.002. arXiv: NIHMS150003.
5. Casey H. Halpern et al. “Brain shift during deep brain stimulation surgery for Parkinson’s disease”. In: Stereotactic and Functional Neurosurgery 86.1 (2007), pp. 37– 43. issn: 10116125. doi: 10.1159/000108587.
6. Derek L.G. G Hill et al. “Measurement of intraoperative brain surface deformation under a craniotomy”. In: Neurosurgery 43.3 (1998), pp. 514–526. issn: 0148396X. doi: 10.1097/00006123-199809000-00066.
7. Max C. Keuken and Birte U. Forstmann. “A probabilistic atlas of the basal ganglia using 7 T MRI”. In: Data in Brief 4 (2015), pp. 577–582. issn: 23523409. doi: 10.1016/j.dib.2015.07.028. url: http://dx.doi.org/10.1016/j.dib.2015. 07.028.
8. Michael I. Miga. “Computational Modeling for Enhancing Soft Tissue Image Guided Surgery: An Application in Neurosurgery”. In: Annals of Biomedical Engineering (2016). issn: 15739686. doi: 10.1007/s10439-015-1433-1.
9. Aida Georgeta Monea et al. “Assessment of relative brain-skull motion in quasistatic circumstances by magnetic resonance imaging.” In: Journal of neurotrauma 29.13 (2012), pp. 2305–17. issn: 1557-9042. doi: 10.1089/neu.2011.2271. url: http: //www.ncbi.nlm.nih.gov/pubmed/22663153.
10. Yangming Ou et al. “DRAMMS: Deformable registration via attribute matching and mutual-saliency weighting”. In: Medical Image Analysis 15.4 (2011), pp. 622– 639. issn: 13618415. doi: 10.1016/j.media.2010.07.002. arXiv: NIHMS150003. url: http://dx.doi.org/10.1016/j.media.2010.07.002.
11. M. H.T. Reinges et al. “Course of brain shift during microsurgical resection of supratentorial cerebral lesions: Limits of conventional neuronavigation”. In: Acta Neurochirurgica 146.4 (2004), pp. 369–377. issn: 00016268. doi: 10.1007/s00701- 003-0204-1.
12. Arash A. Sabet et al. “Deformation of the human brain induced by mild angular head acceleration”. In: Journal of Biomechanics 41.2 (2008), pp. 307–315. issn: 00219290. doi: 10.1016/j.jbiomech.2007.09.016. arXiv: NIHMS150003.
13. Sonja Schnaudigel et al. “Positional brain deformation visualized with magnetic resonance morphometry”. In: Neurosurgery 66.2 (2010), pp. 376–384. issn: 0148396X. doi: 10.1227/01.NEU.0000363704.74450.B4.
14. Steve Smith. FLIRT. 2013. url: https://fsl.fmrib.ox.ac.uk/fsl/fslwiki/ FLIRT (visited on 10/10/2018).
15. Neuroimage Technologies and Surgical Technologies Lab. MNI152. 2018. url: http://nist.mni.mcgill.ca/?page{\_}id=714 (visited on 27/08/2018).
16. Nikos Makris et al. "Decreased volume of left and total anterior insular lobule in schizophrenia". In: Schizophrenia Research, 83(2–3) (2006), pp. 155–171. https://doi.org/10.1016/j.schres.2005.11.020
Figures