3834
Highly Undersampled Radial Passive Marker Tracking with Phase-only Cross-Correlation (POCC) for Real Time Image Guidance1Department of Radiology, Medical Physics, Medical Center ‐ University of Freiburg, Faculty of Medicine, University of Freiburg, Freiburg, Germany, 2Interventional Systems GmbH, Kitzbuehel, Austria
Synopsis
Marker tracking with phase-only cross correlation (POCC) is an efficient technique to localize instruments during percutaneous MR-guided interventions in closed-bore MR systems. Unfortunately, POCC is time-consuming, as additional marker images need to be continuously acquired. Here, we present a drastically accelerated POCC sequence that uses radially undersampled images to detect the passive marker. With a modified POCC algorithm this sequence can detect marker movements within less than 108ms thus providing a very fast position feedback. The precision of the POCC sequence was evaluated in phantom measurements, and a possible in vivo targeting scenario was demonstrated in a volunteer.
Introduction
In MR-guided percutaneous biopsies, passive needle guides with markers are used for instrument visualization. These markers can be detected automatically and reliably with a phase-only cross-correlation (POCC) algorithm1-3. With the POCC technique the marker is imaged in two tracking slices orthogonal to the marker’s symmetry axis and, subsequently, the position information is used to automatically align a targeting slice. This way, the sequence follows the marker and visualizes the theoretical needle trajectory so that it can be used for targeting of the needle pathway4,5.
POCC tracking images do not contain clinically relevant information, but their acquisition is time-consuming which reduces the achievable temporal resolution. We have shown recently that the marker can be detected much faster in highly undersampled radial data6. Here, we demonstrate the integration of undersampled radial imaging into the tracking sequence to substantially reduce the duration of one tracking/targeting cycle to be able to visualize moving structures during the targeting process. The targeting accuracy and duration of the modified tracking sequence was evaluated in phantom measurements during needle insertions. Additionally, the sequence was tested in vivo in a volunteer mimicking a liver biopsy scenario.
Methods
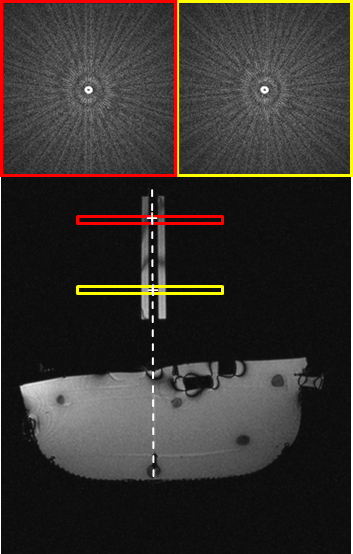
The radial POCC tracking sequence automatically detects the position of a cylindrical marker with a central opening for needle insertion that is filled with a contrast agent. The two parallel radial tracking images (T1-weighted FLASH) are oriented perpendicular to the marker’s symmetry axis and acquired with an adjustable number of radial projections Np. The images are reconstructed online with a Kaiser-Bessel regridding algorithm with a subsequent Fourier-Transform. In these images, the ring-like cross section of the marker is automatically detected with a modified POCC algorithm – the streaking artifacts in the highly undersampled images are accounted for by incorporating the radial point spread function of the marker6. The position information is then used to align a subsequent targeting image (bSSFP) in parallel to the marker axis, i.e. the theoretical needle trajectory. The acquisition of tracking and targeting images runs continuously to follow movements of the marker in real time (Fig. 1).
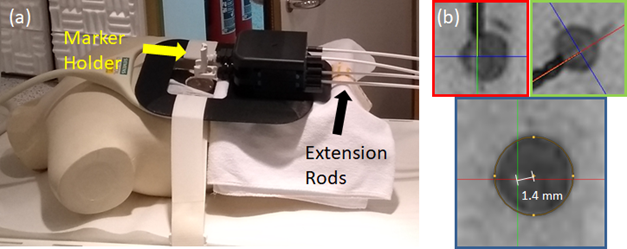
The tracking sequence with radially undersampled tracking images was implemented on a 1.5T whole body MR system (MAGNETOM Symphony, Siemens Healthcare, Erlangen, Germany). To assess the lateral needle targeting accuracy and duration, insertions were performed in a phantom with 15 embedded fiducial targets using the system’s loop coil for signal reception. The marker was manipulated with an in-bore assistance system (GantryMate, Interventional Systems, Kitzbühel, Austria) (cf. Fig. 2a) [7]. For each targeting and insertion maneuver, the marker was initially positioned in a neutral position. Then, the needle trajectory was aligned with the target under real time image guidance (TACycle=0.5s) with the radial POCC tracking sequence with only Np=15 projections. The other imaging parameters were: TR/TE=3.58/1.68ms, BW=965Hz/px, SLbSSFP=6mm, SLFLASH=10mm, FOV=300×243mm², matrix = 156x192, PF=6/8 resulting in an acquisition time for the 2 tracking slices of 2 x 53.7ms. After alignment, a 16G needle (Somatex GmbH, Teltow, Germany) was inserted and the distance of the needle from the target center was determined in reformatted multi-planar views of a 3D bSSFP data set (resolution: (0.67mm)³, Fig. 2b).
To demonstrate the advantage of the accelerated marker tracking, the POCC sequence was tested in a healthy volunteer. To simulate a liver biopsy the volunteer was placed in supine position, with the assistance system on the liver region (Fig.3a). A cross section of a hepatic blood vessel was defined as a target (Fig.3b), and the POCC sequence was used to track the marker during the respiratory motion of the liver. During a breathhold the theoretical needle trajectory (green) was then aligned with the target (Fig. 4).
Result
The integration of radial undersampling into the tracking sequence enabled substantially faster marker tracking than conventional POCC sequences, and Np=15 projections were sufficient to achieve reliable marker detection. In the phantom, all targets were successfully punctured with a mean targeting time of 126±80s (mean±standard deviation) and lateral targeting accuracy of 1.2±0.5mm. Proof-of-concept of the in vivo applicability of the sequence could be successfully demonstrated.Discussion & Conclusion
Our experiments demonstrate that highly undersampled radial imaging could be successfully integrated into the POCC tracking sequence for fast needle guide tracking. The measured accuracy in phantoms was comparable to previous studies indicating that accelerated marker tracking is possible without degrading the tracking accuracy. Further, implementation of parallel imaging technologies (e.g. GRAPPA) into the acquisition of the targeting image of the sequence would reduce the tracking cycle duration even more. The accelerated sequence might help to accelerate image-guided percutaneous interventions and even enable targeting of moving structures.Acknowledgements
This study was supported by a grant of the Tiroler Innovationsförderung (Projekt: GantryMate).References
[1] Beyersdorff, D. et al. MR Imaging–guided Prostate Biopsy with a Closed MR Unit at 1.5 T: Initial Results1. Radiology 234, 576–581 (2005).
[2] de Oliveira A, et al. Automatic passive tracking of an endorectal prostate biopsy device using phase-only cross-correlation. Magn Reson Med 59:1043–1050 (2008)
[3] Krafft AJ, et al. Passive marker tracking via phase-only cross correlation (POCC) for MR-guided needle interventions: Initial in vivo experience. Physica Medica 29:607-614 (2013)
[4] Zamecnik P, et al. Automated Real-time Needle-Guide Tracking for Fast 3-T MR-guided Transrectal Prostate Biopsy: A Feasibility Study. Radiology 273:879-886 (2014)
[5] Reichert A, et al. Simultaneous slice excitation for accelerated passive marker tracking via phase-only cross correlation (POCC) in MR-guided needle interventions. MAGMA (2018)
[6] Reichert A, et al. Passive Marker Tracking with Phase-Only Cross Correlation (POCC) in Highly Undersampled Radial Images: Improvements by Point-Spread-Function Considerations. Proc. Intl. Soc. Mag. Reson. Med. 26 (2018)
[7] Krafft AJ, et al. An MR-compatible Assistance System for MR-guided Needle Interventions: Initial Phantom Evaluation. Proc. Intl. Soc. Mag. Reson. Med. 24 (2016)
Figures