3833
A simple freehand technique for MRI-guided needle localization of suspicious breast lesions1radiology, Renji Hospital, Medical College of Shanghai Jiao Tong University, shanghai, China
Synopsis
A total of 273 patients who received needle localization with a bare-hand technique for suspicious breast lesions by using 1.5 T MR-guided were included in our study. The puncture method was similar to CT-guided needle localization of lung nodule. The success rate of localization was 100% (273/273). Procedure time of all the cases ranged from 5 to 30 min (mean, 14.3 min). Our MRI-guided bare-hand needle localization of suspicious breast lesions is a handy, safe, rapid, and accurate interventional method. The lesions that are located at axillary region of breast,areola area, and the special area near the chest wall can all be precisely localized.
INTRODUCTION
Magnetic resonance imaging of the breast has become increasingly useful in the detection1,2, diagnosis and treatment of breast cancer. Clinical studies have demonstrated that MRI can detect lesions that are both mammographically and sonographically occult3,4. Breast MRI has a high sensitivity approaching 100% of detection for invasive breast carcinoma5. When the histopathological examination of suspicious lesions is required, MRI-guided biopsies or surgical biopsies after needle localization are two most important methods. In these years, lots of techniques have been proposed for preoperative localization, including stereotaxic or freehand6,7. Most previousstudies focused on the stereotaxic method whereas the freehand technique has only been used in a small study population7. Both of the two techniques have their own advantages and disadvantages. The freehand technique is a simple and versatile method that is similar to the localization under ultrasound (US) or computed tomography (CT). In this study, we aimed to evaluate the clinical application of MRI-guided needle localization of suspicious breast lesions for surgical biopsy using a simple freehand technique.METHODS
A total of 273 patients who received needle localization with a bare-handed technique for suspicious breast lesions by using 1.5 T MR-guided were included in this study. The puncture method was similar to CT-guided needle localization of lung nodule,. The clinical data were retrospectively analyzed. The accuracy of localization and time spent for the procedure were compared between two independent radiologists with different levels of experience.RESULTS
A total of 273 lesions were analyzed. Overall lesion size ranged from 2.0 to 35.0 mm (mean 10.4 mm). The success rate of MRI-guided localization was 100% in both radiologists (273/273). After surgery resection, the pathological diagnoses were as follows: 36 (13.2%) malignant lesions, 46 (16.8%) high-risk lesions, and 191 (70%) benign lesions. Procedure time of all the cases ranged from 5 to 30 min (mean, 14.3 min). Procedure time of radiologist with high level of experience was from 5 to 27 min (mean, 12.98±3.77 min), and radiologist with low level of experience ranged from 7 to 30 min (average 17.11±5.07 min). There was statistically significant difference in the puncture time between the two radiologists (p value <0.001). Only a small number of patients had a slight hematoma after puncture (n=7, 2.6%), other common complications were not observed.DISCUSSION
Due to the superior sensitivity of breast MRI approaching 100% of detection for invasive breast carcinoma, MRI-guided needle localization breast biopsy is a very useful method for the pathological diagnosis of these occult lesions6-8. In our study we reported the results of MRI-guided needle localization of suspicious breast lesions by using a convenient bare-handed technique. As for the time required to perform MRI-guided needle localization, on average, overall 14.3 min in our study, which are obviously shorter than previously reported median procedure times for MRI-guided needle localization of 20–62 minutes7,9, and the time required for MRI-guided core needle biopsy (38-70 minutes)8,10-11. Furthermore, our research shows that with the increase of radiologists' experience, the puncture time will be shorten and need fewer adjustment times. In the study of Nicole Berger et al6, they performed the localization of the lesion without contrast-agent application using diffusion-weighted imaging. Of the 273 patients in our study, 34 patients successful performed the localization without the application of contrast media, which cases procedure time average 11.06 min (range from 5 to 19 min), shorter than other cases in this study. However, because of fewer cases in that, it is not known whether there is statistical significance. Most studies have demonstrated that localization were used a technique with a gird. In contrast to these techniques using gird, bare-handed localization allowed us freely choose the insertion angle. The lesions that are located at axillary region of breast and areola area, as well as at the special area near the chest wall can be precisely localized. The bare-handed technique also enable localization in patients with silicone implants. In the study of M. A. A. J. van den Bosch et al7, they consider freehand technique localization only could perform in an open MRI system, but in our study we used usual MRI system.CONCLUSION
MRI-guided bare-hand needle localization is a handy, safe, rapid, and highly accurate diagnostic method for small mammographically and sonographically occult breast cancers. Our method is easy to perform, and the time spent for the procedure is extremely short. The lesions that are located at axillary region of breast and areola area, as well as at the special area near the chest wall can be precisely localized. MRI-guided needle localization can be applied to improve early diagnosis and treatment.Acknowledgements
This study has received funding from Shanghai Shenkang Project (16CR3024A) and Shanghai Science and Technology Committee (17441902700).References
1. Iacconi C, Galman L, Zheng J, et al. Multicentric cancer detected at breast MR imaging and not at mammography: important or not?[J]. Radiology, 2015;279:378-384.
2. Woitek R, Spick C, Schernthaner M, et al. A simple classification system(the Tree flowchart) for breast MRI can reduce the number of unnecessary biopsies in MRI-only lesions[J]. Eur Radiol, 2017;27:3799-3809.
3. Raikhlin A, Curpen B, Warner E, et al. Breast MRI as an adjunct to mammography for breast cancer screening in high-risk patients: retrospective review[J]. AJR Am J Roentgenol, 2015;204:889-897.
4. Huzarski T, Gorecka-Szyld B, Huzarska J, et al. Screening with magnetic resonance imaging, mammography and ultrasound in women at average and intermediate risk of breast cancer [J]. Hered Cancer Clin Pract, 2017;15:4.
5. Hata T, Takahashi H, Watanabe K et al, Magnetic resonance imaging for preoperative evaluation of breast can- cer: a comparative study with mammography and ultrasonography. J Am Coll Surg 2004;198:190–197.
6. Nicole Berger, Zsuzsanna Varga, Thomas Frauenfelder et al, MRI-guided breast vacuum biopsy: Localization of the lesion without contrast-agent application using diffusion-weighted imaging. Magnetic Resonance Imaging 2017;38:1–5.
7. van den Bosch MA, Daniel BL, Pal S, et al. MRI-guided needle localization of suspicious breast lesions: results of a freehand technique[J]. Eur Radiol, 2006;16:1811-1817.
8. Wang HY, Zhao YN, Wu JZ, et al. MRI-guided wire localization open biopsy is safe and effective for suspicious cancer on breast MRI[J]. Asian Pac J Cancer Prev, 2015;16:1715-1718.
9. Causer PA, Piron CA, Jong RA, et al. MR imaging-guided breast localization system with medial or lateral access. Radiology 2006;240:369–379.
10. Lehman CD, Deperi ER, Peacock S, McDonough MD, Demartini WB, Shook J. Clinical experience with MRI-guided vacuum-assisted breast biopsy. AJR 2005;184:1782–1787.
11. Perlet C, Heywang-Köbrunner SH, Heinig A, et al. Magnetic resonance-guided, vacuum-assisted breast biopsy: results from a European multicenter study of 538 lesions. Cancer 2006;106:982–990 .
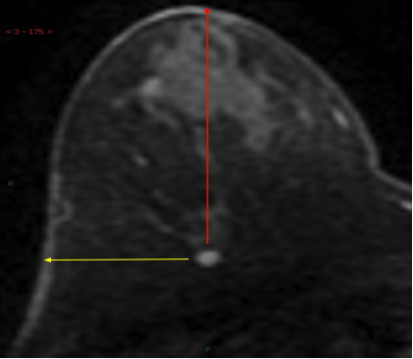
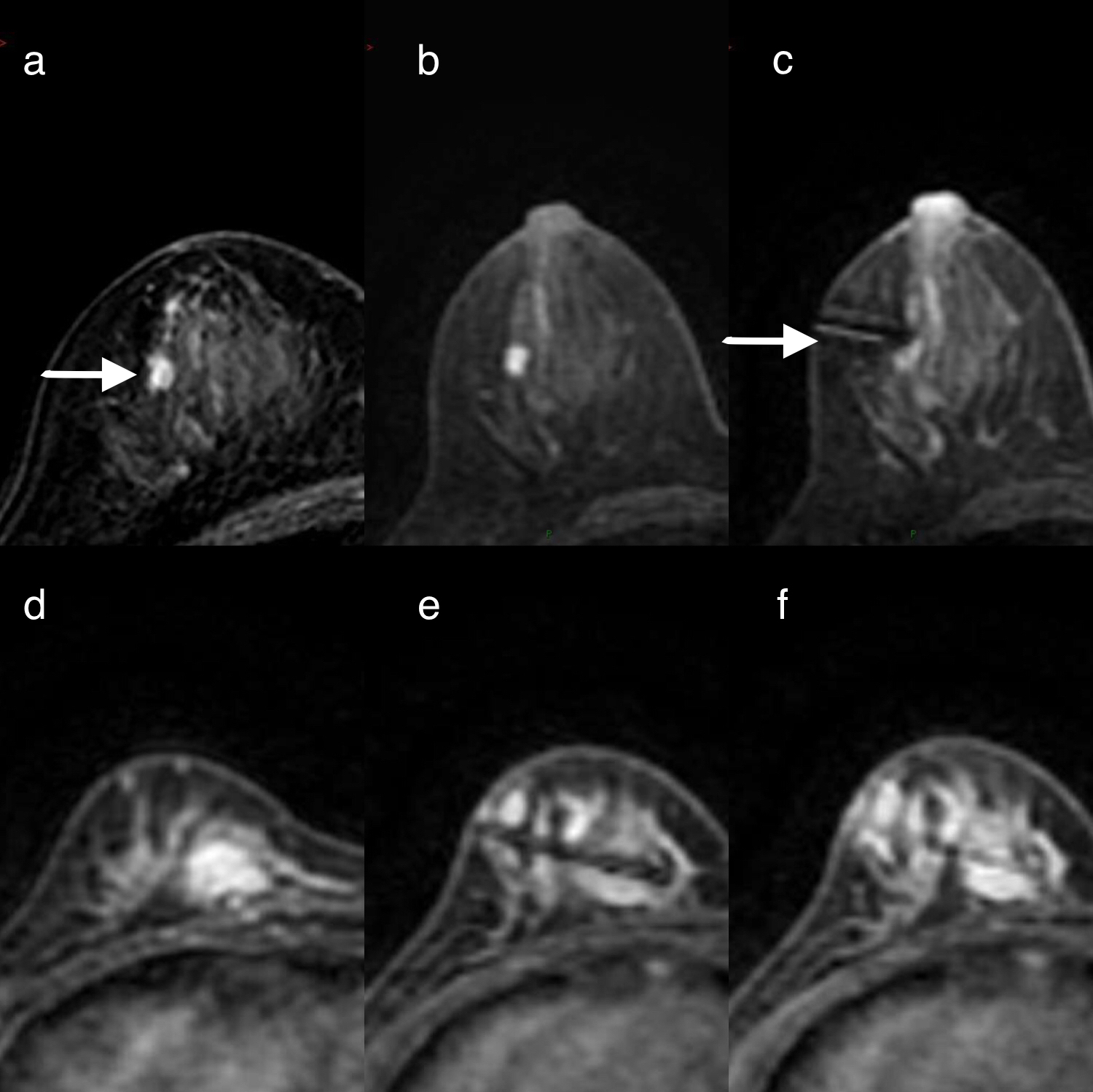
Figures