3818
A Principal Component Analysis based Multi-baseline Phase Correction Method for PRF Thermometry1Siemens Medical Solutions USA Inc., Malvern, PA, United States, 2Siemens Healthcare GmbH, Erlangen, Germany, 3Department of Radiology and Imaging Sciences, University of Utah, Salt Lake City, UT, United States, 4Division of Intramural Research, National Heart Lung and Blood Institute, National Institutes of Health, Bethesda, MD, United States
Synopsis
The use of Proton Resonance Frequency (PRF) based thermometry with thermal therapy procedures is indispensable. Variation in background phase due to motion related changes in B0 is a major source of inaccuracy in PRF thermometry. In this work we propose a novel Principal Component Analysis (PCA) based multi-baseline phase correction approach. We compare this approach with two existing methods using in-vivo human brain and heart data, and demonstrate significant reduction in bias as well as variance of temperature difference estimates. The proposed approach may increase the accuracy of PRF thermometry in or near moving organs, and hence result in improved clinical outcome.
Introduction
Proton Resonance Frequency (PRF) thermometry is a widely used Magnetic Resonance Imaging (MRI) based technique to monitor changes in tissue temperature in response to thermal therapy1. PRF thermometry relies on phase difference between the acquired images, and therefore motion related B0 changes in organs of interest and background adversely affect the accuracy of temperature difference estimates, even when registration-based motion correction is performed to correct for displacements2. In this abstract, we present a novel approach to correct motion related B0 changes in PRF thermometry, and compare our results with some existing approaches.Methods
Data Acquisition:
All human imaging protocols were approved by local Institutional Review Board. One healthy volunteer was imaged on a 3T scanner (MAGNETOM Prisma fit, Siemens Healthcare, Erlangen, Germany) using a prototype 3D segmented EPI sequence3 with following parameters: TR 45ms, TE 23ms, 1.25x2.5x2.5 mm3 resolution, 192x96x12 matrix, EPI factor 9, 100 repetitions. We also acquired a series of navigated, single shot EPI cardiac images from one volunteer with following parameters: One short axis slice, 2x2x4 mm3 resolution, GRAPPA factor 2, saturation slabs parallel to the slice for blood suppression4, 100 repetitions.
Preprocessing:
Each image was registered to the first image in the series. First NB images were chosen as baseline images (referred to as baseline series). The remaining images (referred to as therm series) were used to compute temperature difference maps.
Background phase removal and ΔT estimation: We developed a PCA based algorithm to remove motion related phase changes. The method consists of two steps:
- Computation of basis images: Complex mean of the baseline images BAve is obtained. Principal Component Analysis (PCA) is performed over a signal to noise ratio (SNR) based spatial mask on the series consisting of complex phase difference between baseline images and BAve. First NPC of the resultant eigen-images are retained as basis images for correcting the therm series.
- Baseline removal from therm series: Complex phase difference is computed between each therm image and the corresponding previous image. BAve is used as the image previous to the first therm image. Baseline correction is performed by removing the projection of each difference image onto the subspace spanned by the basis images. Temporal cumulative sum of the resultant series is obtained.
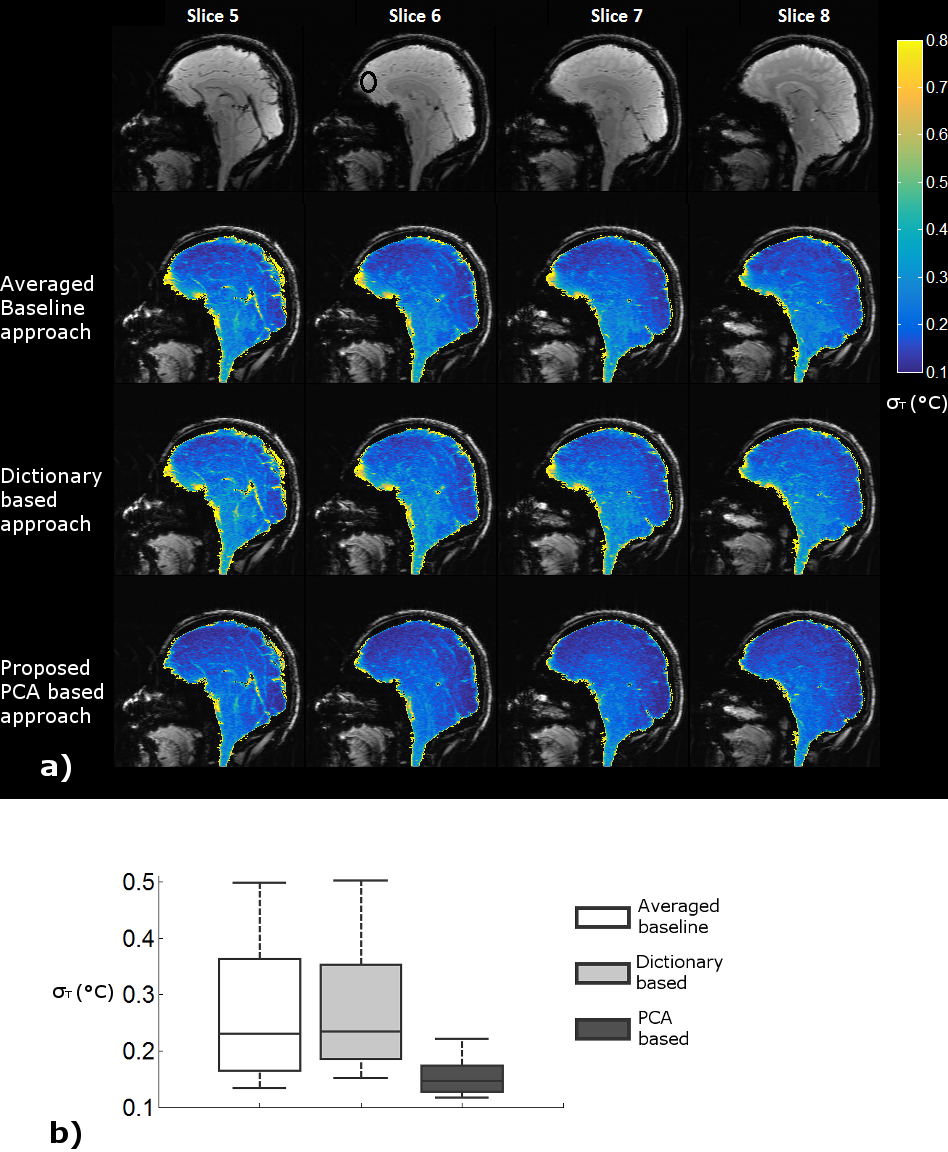
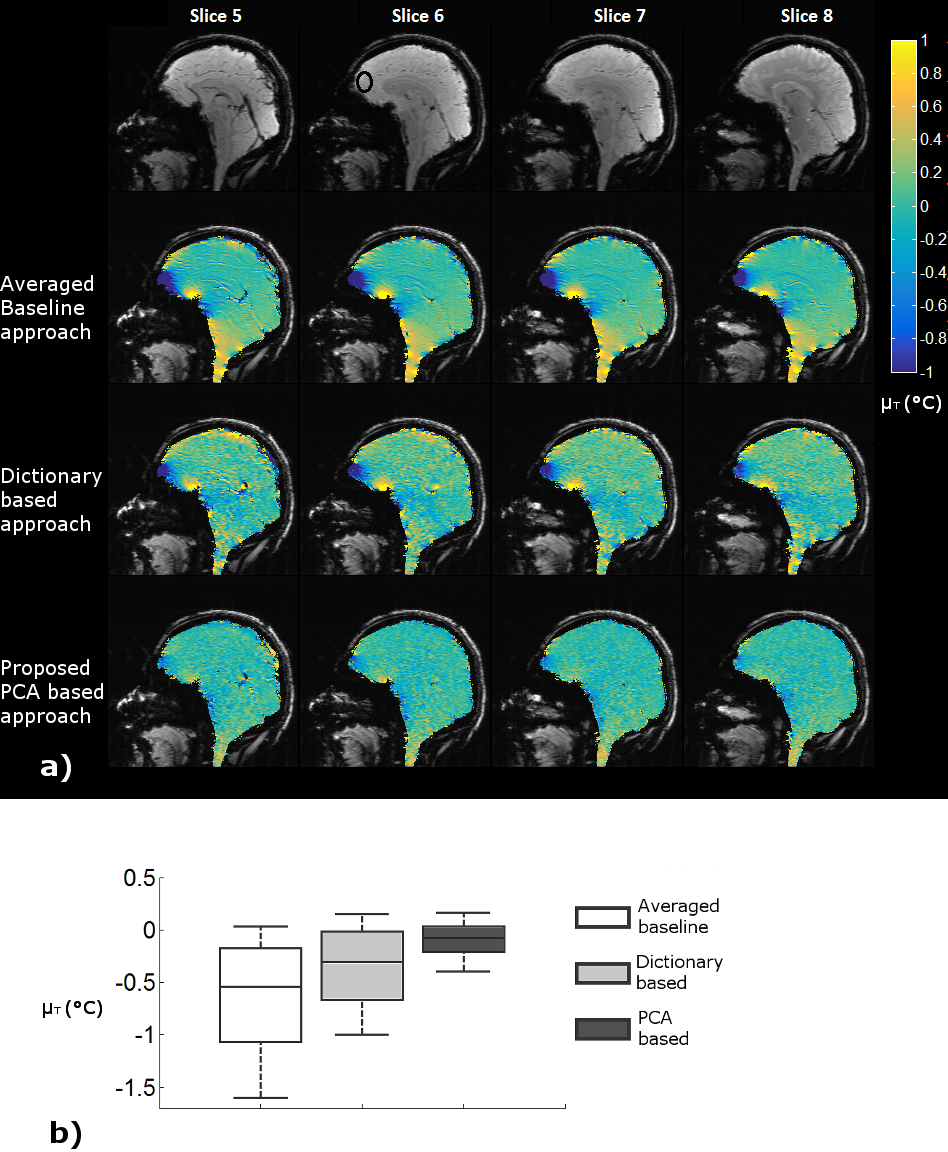
We compared the proposed PCA based approach with two existing approaches: 1) Averaged baseline approach, where BAve is used as reference for phase difference5, and 2) Dictionary based approach, where the best matching baseline image is looked up for each therm image2. For all three approaches, average phase over the aforementioned SNR based mask was removed after baseline correction to eliminate global phase drift. Resultant phase difference images were scaled by (-γ.B0.TE×0.01ppm/°C)-1 to estimate temperature difference relative to the first acquisition. Since the expected temperature change was 0 in absence of external heating, we used temporal mean (µT) and standard deviation (σT) of the estimated ΔT series to assess estimation bias and variability.
Results
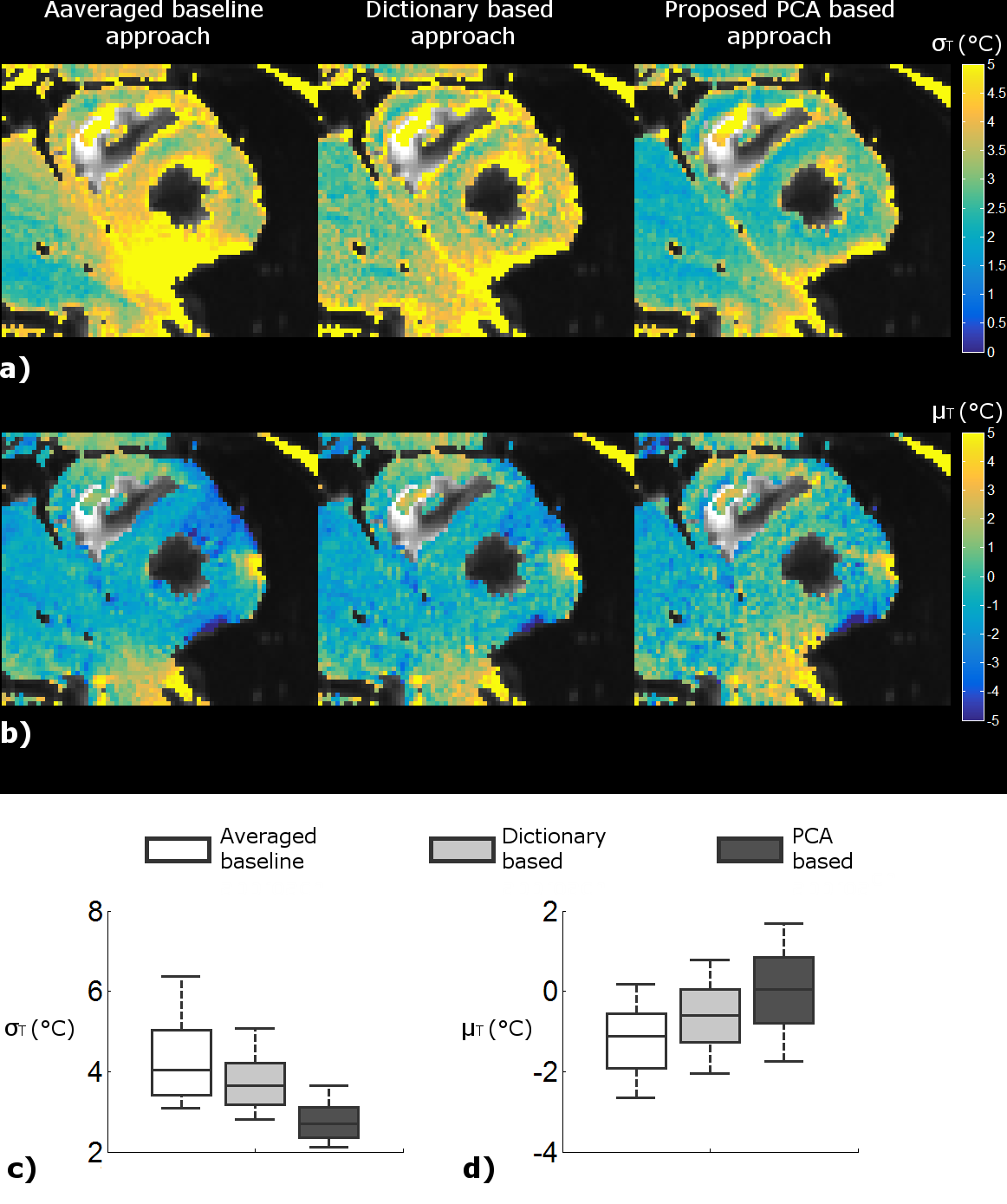
Averaged baseline approach results in elevated σT and |µT| in brain regions affected by susceptibility related B0 changes, such as orbitofrontal cortex and brain stem (Figures 1 and 2). The proposed PCA approach results in a substantial improvement in σT as well as |µT| compared with the averaged baseline and dictionary based approaches (Figure 1 and 2). Similar results are observed for cardiac data (Figure 3).Discussion
The proposed PCA based method outperforms the averaged baseline and dictionary based approaches in the regions prone to motion related B0 changes. This can be attributed to two reasons: 1) PCA bases can be combined to “interpolate” motion states that fall between those captured by the baseline images, and therefore are not exactly represented by any baseline image, and 2) PCA bases have reduced noise as compared with individual baseline images, since incoherent noise is pushed to the bases corresponding to smaller eigenvalues.
Improvement in PRF thermometry technique will play a vital role in more widespread clinical adoption of thermal therapy. The technique proposed in this abstract will add to the tools available to overcome the challenges of PRF thermometry, especially in moving organs. Future work will focus on evaluation on a larger sample and comparison with additional existing approaches.
Acknowledgements
No acknowledgement found.References
- Rieke, V. and Butts Pauly, K. (2008). MR thermometry. Journal of Magnetic Resonance Imaging, 27(2), 376-390.
- Roujol, S., et al. (2010). Real‐time MR‐thermometry and dosimetry for interventional guidance on abdominal organs. Magnetic Resonance in Medicine, 63(4), 1080-1087.
- Odéen, H., et al. (2014). Sampling strategies for subsampled segmented EPI PRF thermometry in MR guided high intensity focused ultrasound. Medical physics, 41(9)
- Toupin, S., et al. (2017). Feasibility of real-time MR thermal dose mapping for predicting radiofrequency ablation outcome in the myocardium in vivo. Journal of Cardiovascular Magnetic Resonance, 19(1), 14.
- Rieke, V., et al. (2013). Comparison of temperature processing methods for monitoring focused ultrasound ablation in the brain. Journal of Magnetic Resonance Imaging, 38(6), 1462-1471.
Figures