3814
Registration of In Vivo MR images to Volumetric Histopathology1Biomedical Engineering, University of Utah, Salt Lake City, UT, United States, 2Department of Surgery, University of Utah, Salt Lake City, UT, United States, 3Department of Radiology and Imaging Sciences, University of Utah, Salt Lake City, UT, United States
Synopsis
As MR guided focused ultrasound (MRgFUS) treatments evolve to treat oncological diseases, the ability to accurately assess the efficacy of treatment is critical. Although there are several MR metrics proposed for assessing MRgFUS treatments, they have not been rigorously validated against gold standard histopathology treatment assessment. Current validation studies that register MR to histopathology do not comprehensively account for all deformations during histological processing. We present a rigorous MR to histopathology registration pipeline that estimates deformation at every step that can be used to accurately validate the efficacy of oncological MRgFUS treatment.
Introduction
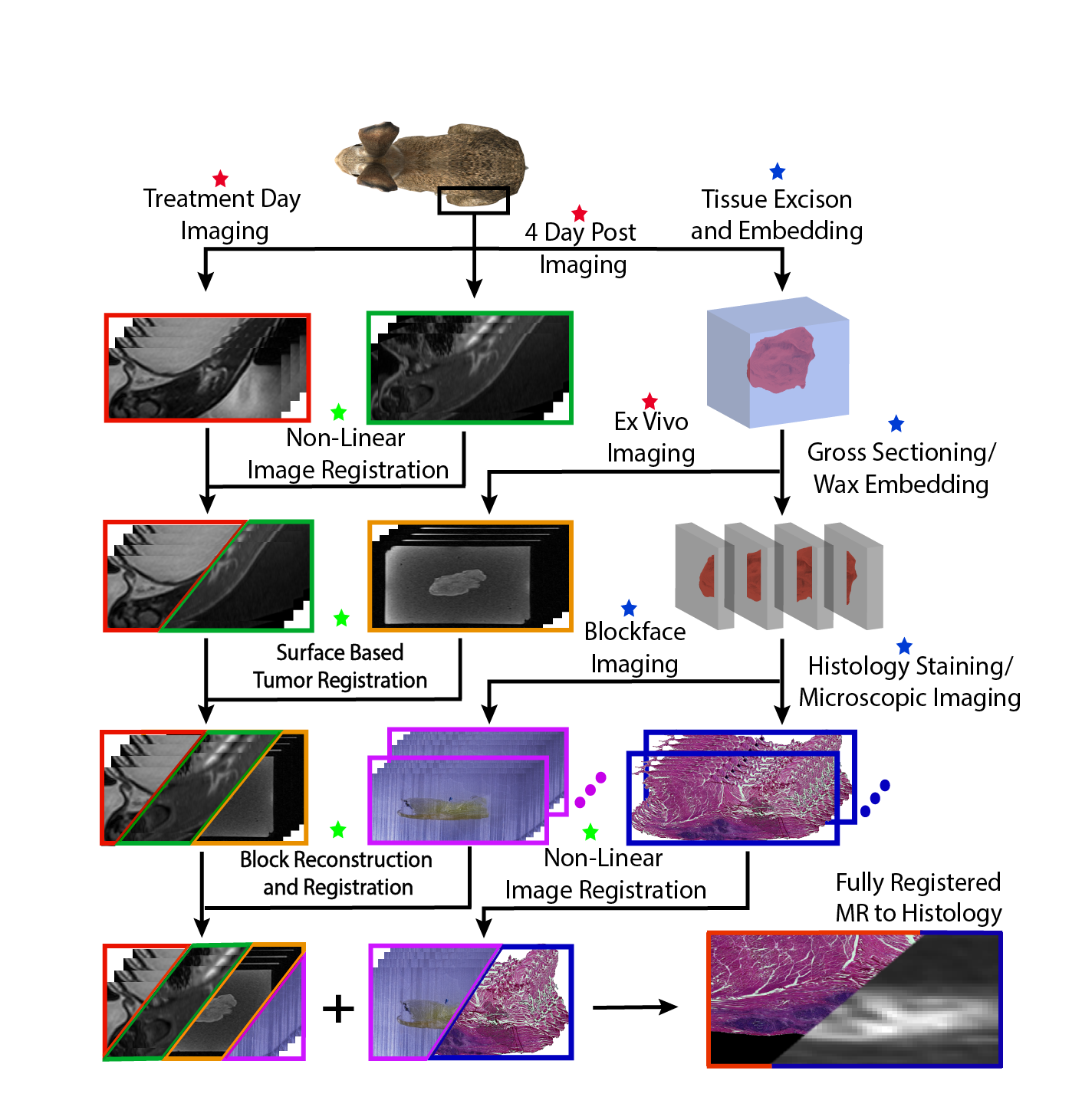
Non-invasive MR-guided focused ultrasound (MRgFUS) treatments have become increasingly popular for treatment of many clinical indications. MR guidance provides anatomical information for treatment planning, real-time monitoring, and multi-parametric acquisitions for treatment assessment. As MRgFUS continues to expand to include more oncological targets, the ability to accurately evaluate tumor viability immediately after the MRgFUS procedure is critical to determine treatment efficacy. Histopathology is the gold standard for evaluating tumor viability or margin status after any cancer therapy. In clinical MRgFUS treatments, contrast enhanced (CE) T1w images are used to determine the resulting non-perfused volume (NPV). However, the acute NPV doesn’t always predict the tumor viability as seen in histopathology images. In addition to CE-T1w imaging, several MR metrics have demonstrated sensitivity to changes in tissue properties following MRgFUS,1 but these metrics have not been rigorously validated against histopathology. This presents a need for an end-to-end pipeline for volumetric MR to histopathology registration that would validate quantitative MR metrics for assessing MRgFUS treatments, ensuring complete destruction of targeted tumor cells. While several studies have been performed to register volumetric histopathology to MR images,2, 3 these studies do not comprehensively account for all tissue deformation during histological processing, such as orientation loss during tissue extraction, shrinkage from tissue fixation, and shearing/stretching from microscopic sectioning. In this work, we present a rigorous in vivo MRI to volumetric histopathology registration pipeline that estimates the deformation at every step (Figure 1).Methods
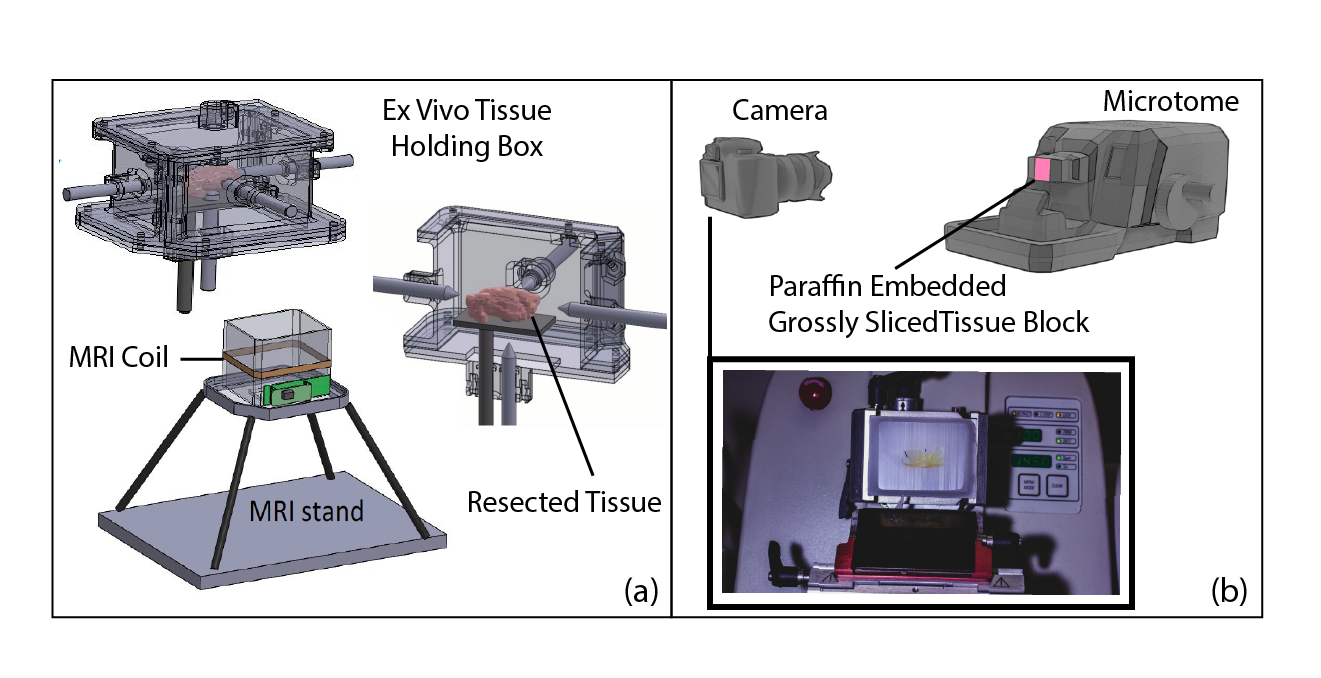
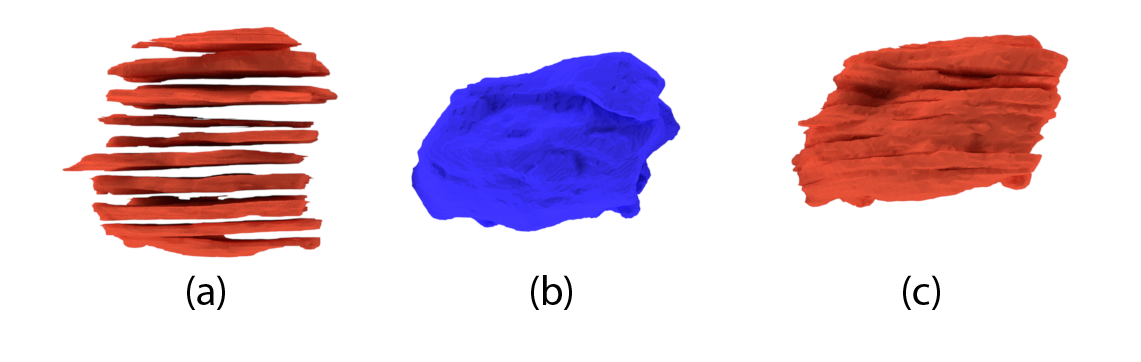
We demonstrate the feasibility of this novel registration pipeline in a rabbit VX2 tumor model. A 3 kg female white New Zealand rabbit (Charles River Laboratory) was injected with approximately 1 × 106 VX2 tumor cells in the belly of both quadriceps. MRgFUS ablation was performed 13 days after injection using a preclinical MRgFUS system (Image Guided Therapy, Inc.) in a 3T MRI scanner (MAGNETOM PrismaFIT, Siemens). The MR sequences used during treatment are shown in Table 1. Post-treatment imaging was performed four days after ablation, the animal was euthanized, and the treated tumor and surrounding tissue were excised. During excision, fixation, and embedding, the in vivo imaging orientation was maintained with tissue inking and a specialized tissue processing box (Figure 2a). The box had an integrated MR coil to facilitate high-resolution ex vivo MR imaging after embedding. The ex vivo imaging generated 3D models 1) of the tumor and ablation regions after extraction and fixation to register to in vivo 3D models and 2) of the resected tissue before gross tissue slicing that served as a target when assembling all the volumes of the grossly sliced tissue (Figure 3b). To register 3D models, each model was considered an unlabeled point set (triangulated surface) and prior mathematical formulations4–6 were used to register the surfaces. This formulation allowed for iterative optimization of the affine transformation between in vivo and ex vivo 3D models to estimate the deformation from tissue excision and fixation. The ex vivo tissue was grossly sliced and each slice was embedded in paraffin wax for microscopic sectioning. During sectioning of each block, digital block face images were acquired (Figure 2b) every 50 μm. Digital images were stacked to form 3D volumes of the tissue in each grossly sliced block (Figure 3a). Affine registration simultaneously optimized a transformation between each 3D model of grossly sliced tissue and the ex vivo 3D tissue model to restore the morphology before gross sectioning (Figure 3c). Finally, each histopathology section was non-linearly registered in 2D to the digital block face image that was acquired immediately before that histological section was taken. This registration estimated shearing/stretching from microscopic sectioning and restored the morphology to before sectioning occurred.Results
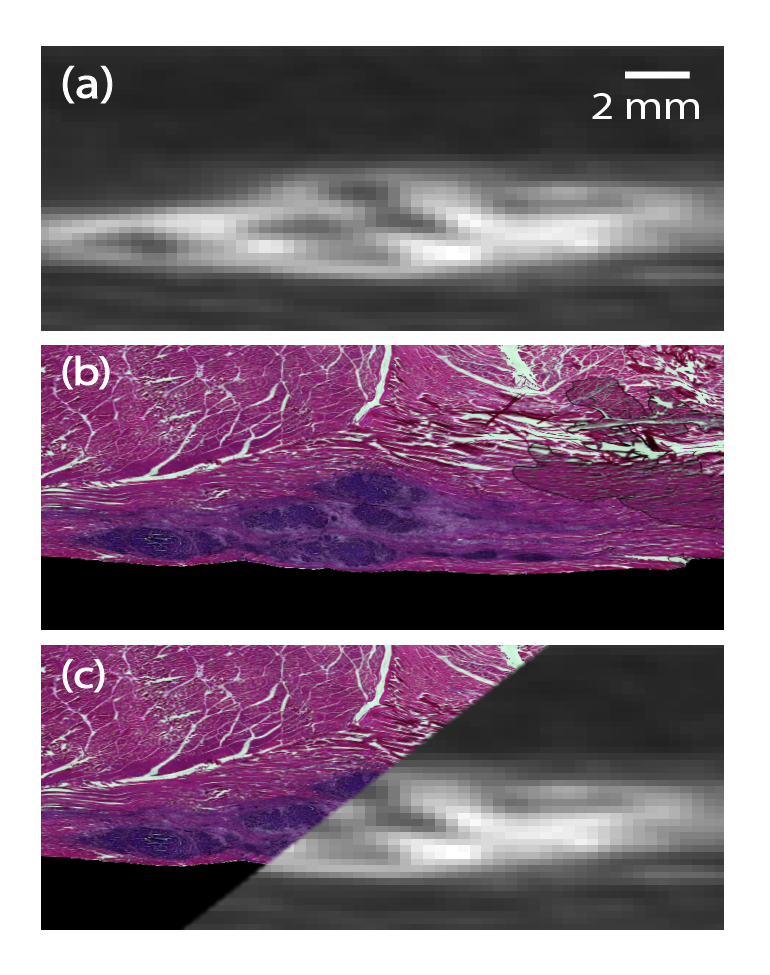
The described registration pipeline accounts for orientation and shrinkage from excision and fixation, loss of morphology from gross slicing, and shearing/stretching from microscopic sectioning. The result of transforming MR to histology images can be seen in Figure 4. All described estimated deformations are invertible and were composed to volumetrically register histopathology to MR images, or MR images to each histopathology image. During this particular MRgFUS procedure, clear ablation is not apparent in the histopathology due to non-ablative temperatures; however, the results demonstrate the potential impact of histopathology to in vivo MRI registration. Further data analysis is ongoing.Conclusions
The developed algorithm provides detailed volumetric registration between acutely obtained multi-parametric, post-treatment MRgFUS MR images and ground truth histopathology images. The results will validate quantitative MR metrics of tissue specific response to MRgFUS treatments, providing a tool that can be used to validate the efficacy of oncological MRgFUS treatments.Acknowledgements
This work was funded by R37CA224141 and R03EB026132.References
1. Stefanie J.C.G. Hectors, Igor Jacobs, Chrit T.W. Moonen, Gustav J. Strijkers, and Klaas Nicolay. MRI methods for the evaluation of high intensity focused ultrasound tumor treatment: Current status and future needs. Magnetic Resonance in Medicine, 75(1):302–317, jan 2016.
2. Are Losnegard, Lars Reisæter, Ole J. Halvorsen, Christian Beisland, Aurea Castilho, Ludvig P. Muren, Jarle Rørvik, and Arvid Lundervold. Intensity-based volumetric registration of magnetic resonance images and whole-mount sections of the prostate. Computerized Medical Imaging and Graphics, 63:24–30, jan 2018.
3. Guy Nir, Ramin S. Sahebjavaher, P. Kozlowski, S. D. Chang, R. Sinkus, S. Larry Goldenberg, and Septimiu E. Salcudean. Model-based registration of ex vivo and in vivo MRI of the prostate using elastography. IEEE Transactions on Medical Imaging, 32(6):1068–1080, jun 2013.
4. Joan Alexis Glaunes, Paris Descartes, and Laurent Younes. L.: Diffeomorphic matching of distributions: A new approach for unlabelled point-sets and sub-manifolds matching Diffusion MRI tractography registration View project Entropy Pursuit View project. 2004.
5. Joan Alexis Glaunes, Sarang Joshi, and Joan Glaunes. Template estimation form unlabeled point set data and surfaces for Computational Anatomy Template estimation form unlabeled point set data and surfaces for Computational Anatomy. 1st MICCAI Workshop on Mathematical Foundations of Computa-tional Anatomy: Geometrical, Statistical and Registration Methods for Modeling Biological Shape Variability Template estima- tion form unlabeled point set data and surfaces for Computational Anatomy. Technical report.
6. Linh Ha, Marcel Prastawa, Guido Gerig, John H Gilmore, Claudio T Silva, and Sarang Joshi. Image registration driven by combined probabilistic and geometric descriptors. Medical image computing and computer-assisted intervention : MICCAI ... International Conference on Medical Image Computing and Computer-Assisted Intervention, 13(Pt 2):602–9, 2010.
Figures