3806
Sacroiliac joint ablation in a chronic swine model using MRgFUS1Radiology and Imaging Sciences, University of Utah, Salt Lake City, UT, United States, 2Orthopedic Surgery, University of California San Francisco, San Francisco, CA, United States, 3Radiology and Biomedical Imaging, University of California San Francisco, San Francisco, CA, United States
Synopsis
There is evidence that MRgFUS might be a very safe and effective minimally invasive technique to treat sacroiliac joint pain caused by arthritis and other degenerative changes. This study in a chronic swine model demonstrated safety and effectiveness of MRgFUS sacroiliac joint ablation and precise ablation of the posterior sacral nerve supply with MRgFUS.
Background
There is evidence that MRgFUS might be a safe and effective minimally invasive technique to treat sacroiliac (SI) joint pain caused by arthritis and other degenerative changes. Similar to radiofrequency ablation (RFA) it targets the lateral branches of the S1 to S4 nerve roots between the posterior sacral foramina and the SI joint. In contrast to RFA, MRgFUS is non-invasive, eliminates the risk of bleeding or infection, is radiation free, and can be repeated if necessary. Kaye et al.1 performed a preliminary sub-acute experiment in swine showing the feasibility of the procedure. In this study, we longitudinally evaluated the safety and effectiveness of MRgFUS ablation of the SI joint in a chronic swine model.Methods
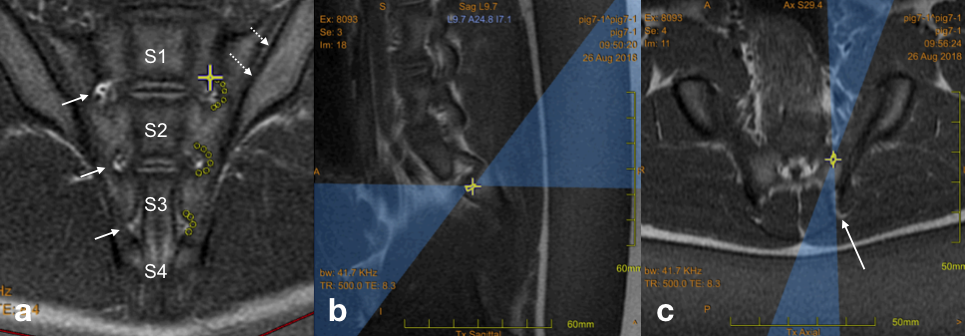
All animal procedures received approval from the Institutional Animal Care and Use Committee. Seven animals have undergone MRgFUS treatment with the Insightec Exablate 2000 (in-table) system in a 3T scanner using three energies (n = 3 with 700J, n = 3 with 1000J, n =1 with 1500J) at 1.35 MHz frequency. Sonication duration was 20 sec for all sonications. Sonications were planned in oblique coronal slices lateral and in a semicircle around the foramina (S1: 7 sonications, S2: 6 sonications, S3: 0-4 sonications) targeting the lateral branches of the nerve roots (Figure 1a). The beam was angled to achieve close to normal incidence onto the surface of the sacrum (Fig. 1b) and to avoid the posterior iliac spine (Fig. 1c). The left side of the animal was treated, the right side served as control.
After post-treatment imaging (baseline), the animals were recovered from anesthesia, assessed for pain, behavior, ambulation, and gait according to the following lameness score: Score 0: Rises immediately, moves freely with balanced weight on all limbs; Score 1: Rises immediately, but demonstrates reluctant movement or uneven weight distribution; Score 2: Moves slowly with short steps. Extended period of time with reduced weight or non-weight bearing on hind limbs; Score 3: Refuses to move from the ground.
The animals were then followed for 5 weeks and euthanized after an additional MR imaging session (follow-up). The sacrum was removed for histopathological analysis (gross histology, H&E, Neurofilament 200 antibody) and confirmation of the imaging results.
Results
Treatment dose and temperature rise were clearly seen on MR temperature imaging in all experiments showing that contiguous lesions along the left SI joint were achieved in all animals. The ablated region was well estimated by the thermal dose measurements. Treatment effects were ore pronounced on follow-up images than on baseline.
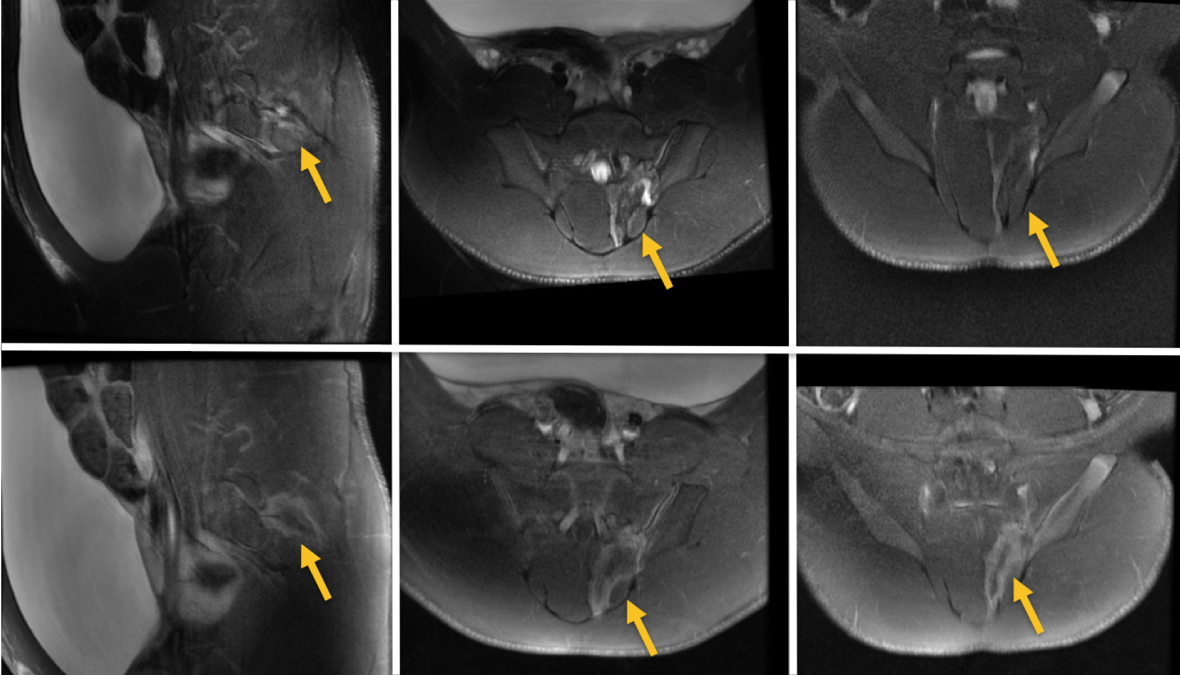
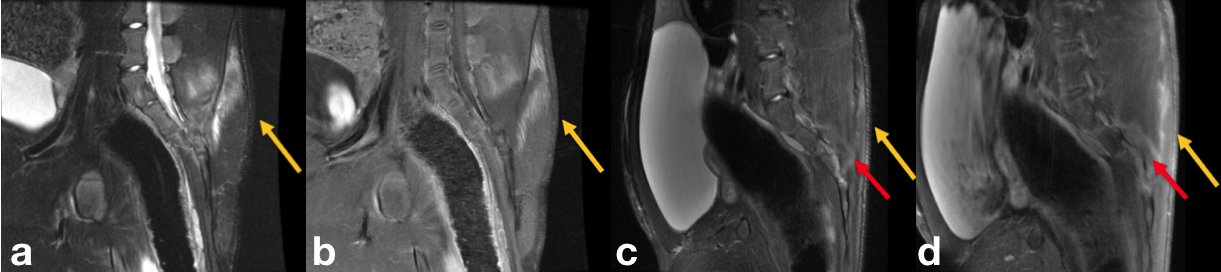
Assessment of behavior, ambulation and gait showed no signs of pain or impairment (lameness score 0 for all animals), and there were no changes in animal behavior or appetite. At 5 week follow-up, treatment effects were still visible in MR images and the extend of the lesion depended on the energy used (Figs. 2 and 3).
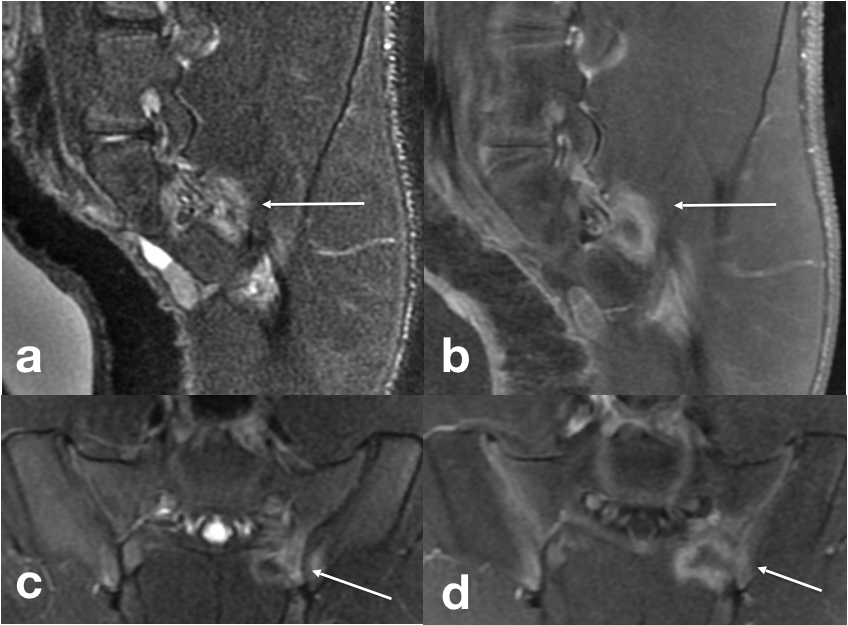
One animal (medium energy of 1000J) had a clearly visible and palpable swelling directly under the skin in the near-field after the procedure. The pig did not appear to have pain in that region, and the swelling subsided within one week. MR images of baseline and follow-up of this animal are shown in Fig. 4.
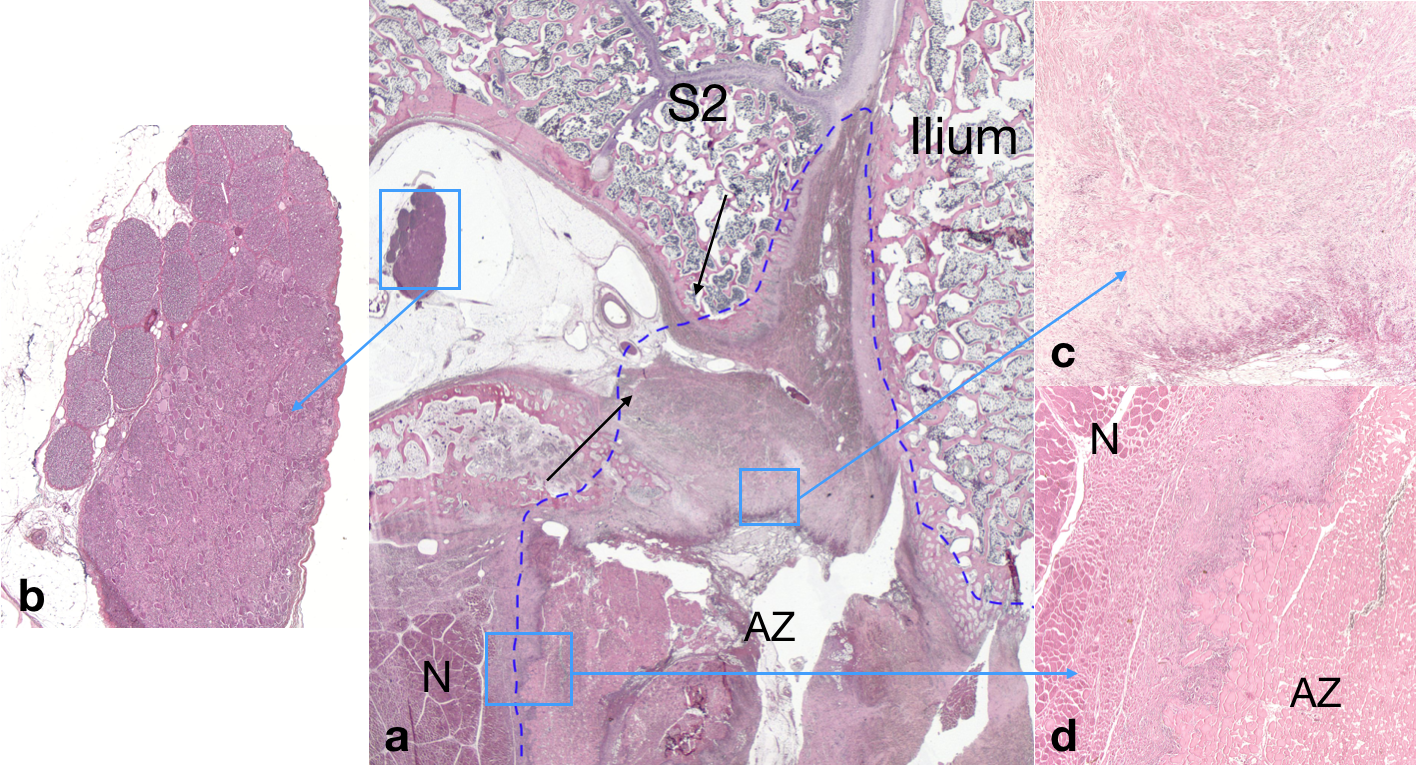
Gross histology showed ablation of the targeted area. The ablated muscle tissue posterior to the sacrum appeared pale with surrounding hemorrhage presenting as a brown rim. The depth of the lesions in muscle increased with increasing energy. H&E images clearly shows the ablated area within the targeted region (Fig. 5).
Discussion
Through longitudinal assessment of the animal's behavior and ambulation, the study demonstrated the safety of MRgFUS sacroiliac joint ablation using energies of up to 1500J per sonication. MR temperature and thermal dose images allowed to estimate the ablated area, which was important as post-treatment images (T2w and CE T1w) did not show a treatment effect immediately after the procedure in some animals. It appears that pressure from the animal's body weight and lying in the same position for the duration of the procedure influences the amount of perfusion and uptake of contrast agent in the treatment region. Histology results show that nerves in the targeted area are successfully ablated, indicating effectiveness of the procedure.Conclusion
This study in a chronic swine model showed safety and effectiveness of MRgFUS sacroiliac joint ablation. It demonstrated that SI joint ablation using MRgFUS is a safe treatment and histological results showed treatment effectiveness through successful nerve ablation in the targeted area. The results of this study will be paramount for obtaining regulatory approval for a clinical trial for this promising alternative to RFA.Acknowledgements
This work was funded by the Focused Ultrasound Foundation (FUS464) and a UCSF Department of Radiology and Biomedical Imaging Seed Grant.References
1) Kaye EA, Maybody M, Monette S, Solomon SB, Gulati A. Ablation of the sacroiliac joint using MR-guided hight intensity focused ultrasound: a preliminary experiment in a swine model. Journal of Therapeutic Ultrasound (2017) 5:17, p.1-10.Figures