3802
Disrupted functional connectivity strength in overactive bladder syndrome patients1Beijing Chaoyang Hospital, Beijing, China
Synopsis
A dysregulation of the brain-bladder control network has been revealed by the functional brain imaging studies. However, the brain functional connectivity strength (FCS) of OAB still remains unclear. Our study investigated the changes of intrinsic whole brain functional connectivity pattern in OAB using FCS. Patients with OAB have impaired pattern of FCS, which shows abnormal short-range and long-range FCS in brain regions associated with brain-bladder network. Behavioural treatments of the OAB based on fMRI may provide new sight into clinical practice.
INTRODUCTION
Overactive bladder syndrome (OAB) is defined as a symptom syndrome characterized by urgency, usually with urinary frequency and nocturia, with or without urgency incontinence. The etiology of OAB is multifactorial and thought to be a result of detrusor overactivity (DO), and altered peripheral and/or central nerve activity. A dysregulation of the brain-bladder control network has been revealed by the functional brain imaging studies. However, the brain functional connectivity strength (FCS) of OAB still remains unclear. As a data-driven approach, FCS was put forword for a large-scale, bias-free, and prior-hypothesis-free whole brain network analysis1. We hypothesize that OAB patients would show abnormal functional hubs and connections in brain regions associated with bladder-brain control network2.METHODS
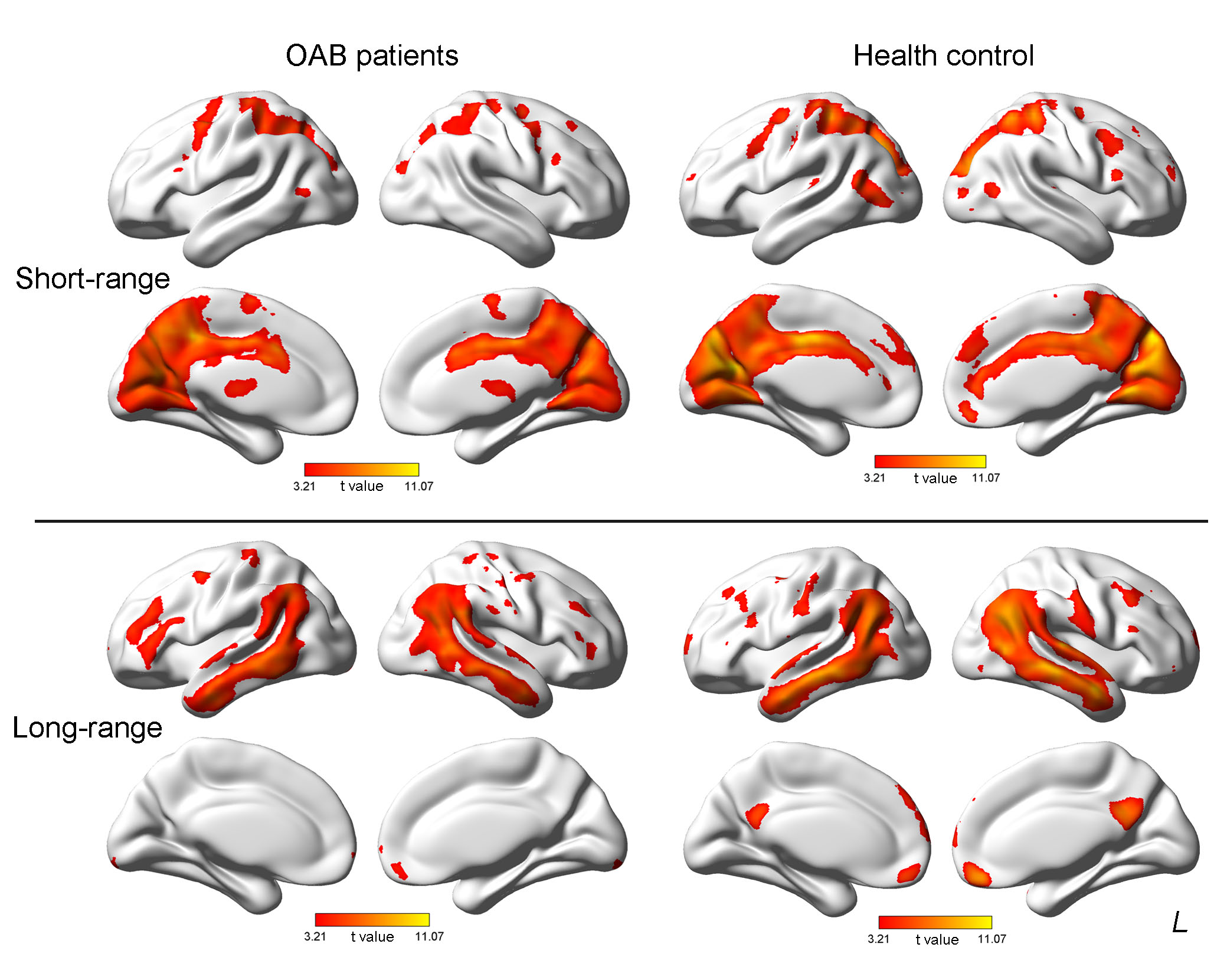
This study investigated the changes of intrinsic whole brain functional connectivity pattern in OAB using functional connectivity strength (FCS). The functional connectivity strength (FCS) metric is derived from degree centrality (DC) of a weighted network in graph theory, calculating DC of each voxel in whole-brain cortex and subcortical area3. We acquired resting-state functional magnetic resonance imaging (rsfMRI) data from twenty-six OAB patients and twenty-eight healthy controls. Briefly, Pearson’s correlation coefficients were computed between the time series of all pairs of gray matter voxels within a gray matter mask, and a whole-brain FC matrix was obtained for each participant. Individual correlationmatrices were then transformed into a z-score matrix using Fisher z-transformation to improve normality. The regional FCS of a voxel was computed as the sum of the connections (z values) between a given voxel and all other voxels. Then, we divided The short-range regional FCS of a voxel referred to the sum of those connections (Z-values) between the voxel and other GM voxels with anatomical distances less than 75 mm to the given voxel, whereas the long-range FCS of a voxel referred to the distances greater than 75 mm. Specifically, a FCS map was computed in each subject and the regions with higher FCS value were considered as functional network hubs. We employed one-sample t tests on FCS within groups to find regions as hubs. Further, two-sample t tests were performed to compare FCS between groups. The resulting statistical map was performed multiple comparisons using Gaussian Random Field (GRF) theory (voxel p value < 0.001, cluster p value < 0.05, corrected).RESULTS
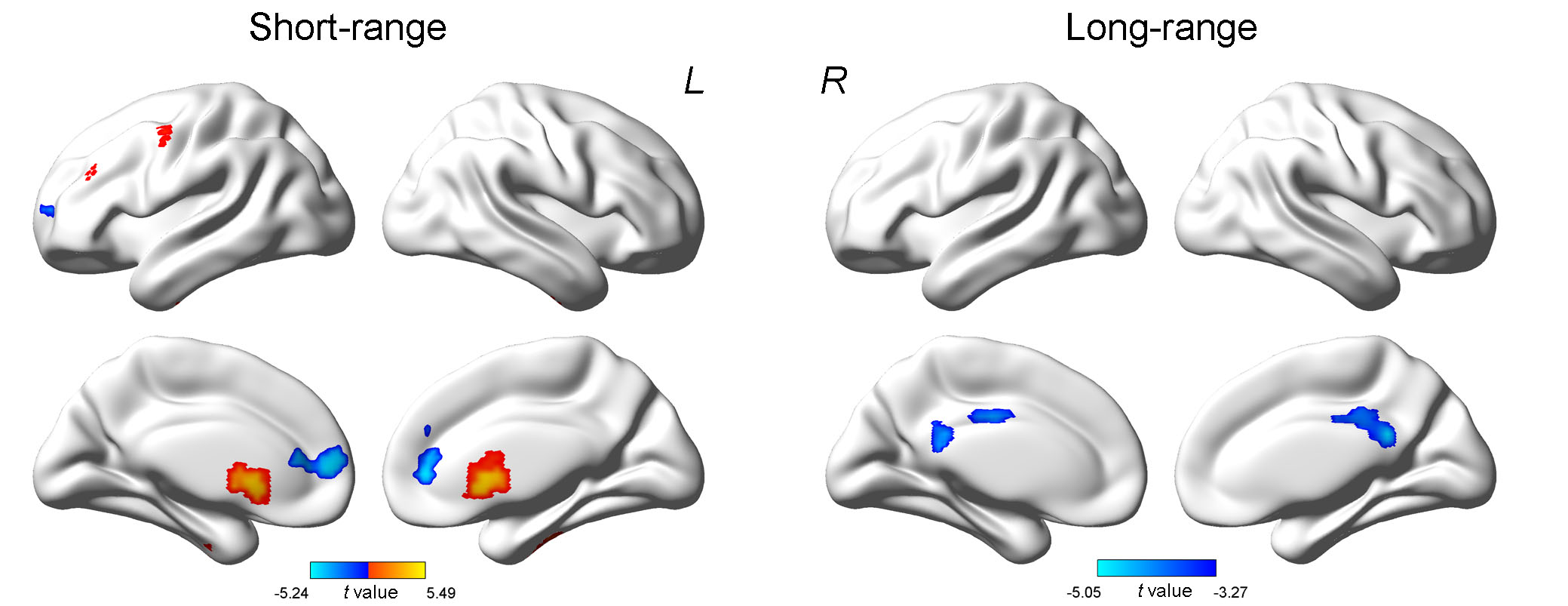
Compared with healthy control subjects, the OAB patients exhibited significantly decreased short-range FCS in the right medial superior frontal gyrus (SFGmed. R) and bilateral anterior cingulate gyrus (ACG), and increased short-range FCS in the middle frontal gyrus (MFG. R), the precentral gyrus (PreCG. R) and bilatteral caudate nucleus (CAU). In addition, Significantly decreased long-range FCS was found in bilateral middle cingulate gyurs (MCG) and posterior cingulate gyrus (PCG).DISCUSSION
Our resting-state FC analysis and found extensive FCS abnormalities in brain regions mainly involved in bladder-brain network. Indeed, the circuit 1 and the cirtuit 3 are part of the well-known DMN. Deactivation would be caused when the brain processes an event that requires attention, such as bladder filling, and DMN activity is suspended at the same time4. The altered function of the SFGmed leads to its connecting pathways, or an overall decrease in brain activation initiated by weakened bladder afferents. We make assumptions that the disordered DMN might disturb the two circuits of the working model. The Circuit 2 corresponds with another established brain network: the salience network. The SN contributes to a variety of complex brain functions, including selfawareness through the integration of sensory, emotional, and cognitive information5. The dACC can create the associated emotion—desire to void or urgency, the ‘salience’ of the bladder filling sensation. Speculatively, homeostasis (continence) seems to be maintained by two mechanisms that are driven by two wellknown neural networks.CONCLUSION
In conclusion, patients with OAB have impaired pattern of FCS, which shows abnormal short-range and long-range FCS in brain regions associated with brain-bladder network. Our study unveils complicated alterations of FCS in OAB patients and provide us with new insight into the underlying brain network topology of OAB.Acknowledgements
No acknowledgement found.References
1. Zuo XN, Ehmke R, Mennes M, et al.Network centrality in the human functional connectome. Cereb Cortex. 2012; 22(8):1862-75.
2. Kitta T, Mitsui T, Kanno Y, et al. Brain-bladdercontrol network: the unsolved 21st century urological mystery. Int J Urol. 2015; 22(4):342-8.
3. Buckner RL, Sepulcre J, Talukdar T, et al. Cortical hubs revealed by intrinsic functionalconnectivity: mapping, assessment of stability, and relation to Alzheimer'sdisease. J Neurosci. 2009;29(6):1860-73.
4. Griffiths D, Derbyshire S, Stenger A, et al. Brain control of normal andoveractive bladder. J Urol. 2005; 174(5):1862-7.
5. Gogolla N, Takesian AE, Feng G, et al. Sensory integration inmouse insular cortex reflects GABA circuit maturation. Neuron. 2014 20; 83(4):894-905.
Figures