3798
Abnormal local spontaneous brain activity revealed by resting-state fMRI as a biomarker for predicting radiation-induced neurocognitive dysfunction in patients with nasopharyngeal carcinoma1Department of Medical Imaging, Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China, Guangzhou, China, 2GE Healthcare, MR Research China, Beijing, China, 3Department of Radiology, The Third Affiliated Hospital of Guangzhou Medical University, Guangzhou, China
Synopsis
In this study, we hypothesize that radiation therapy induce longitudinal neurocognitive dysfunction in patients with nasopharyngeal carcinoma. To verify this hypothesis, resting-state functional magnetic resonance imaging (fMRI) was used to detect the local spontaneous brain activity in 38 patients with nasopharyngeal carcinoma 20 healthy controls at the baseline and follow-up examinations. The changes in brain activity at the early delayed stage after radiation therapy are then used to predict the brain functional impairment at a later stage. The results showed that radiation therapy may induce significant changes in reginal homogeneity in the brain, and such changes at early delayed stage may serve as a potential biomarker for predicting neurocognitive dysfunction at a later stage.
Purpose
Increasing evidence indicates that early radiation-induced subtle changes in the brain may be the precursors to long-term, permanent brain dysfunction at late delayed stage post radiation therapy (RT) (1) . This study aims to track the longitudinal changes in brain activity induced by RT in patients with nasopharyngeal carcinoma (NPC) and to determine whether early abnormal local spontaneous brain activity can predict late neurocognitive dysfunction after RT.
Materials and methods
Thirty-eight newly diagnosed, treatment-naive NPC patients (25 male/13female, aged 18–55 years old, 39.29 ± 8.89 years old) and 20 healthy controls (13 male/7female, aged 26–55 years old, 40.65 ± 9.76 years old) were included in this study. Each patient received 2~3 months’ RT treatment. All the patients underwent resting-state fMRI scanning and Montreal Cognitive Assessment (MoCA) test at three time points: baseline (prior to RT), early delayed stage (EDS, 1~3 months after RT completion) and late delayed stage (LDS, 6 months after the completion of RT). The healthy controls were followed up in parallel at baseline, 6 months and 9 months). Regional Homogeneity (ReHo) changes among three stages were estimated using a whole-brain voxel-wise one-way analysis of variance (ANOVA) with repeated measures. The mean ReHo values of each ROI that showed significant differences were extracted separately using the REST V1.8 software (2) and were used for a post hoc analysis. Multivariate logistic regression and receiver operating characteristic curve (ROC) analyses were used to test the efficacies of the mean ReHo at EDS and the clinical characteristics (age, gender and the irradiation dose on bilateral temporal lobe) alone or combined together in predicting the cognitive impairment at LDS.
Results
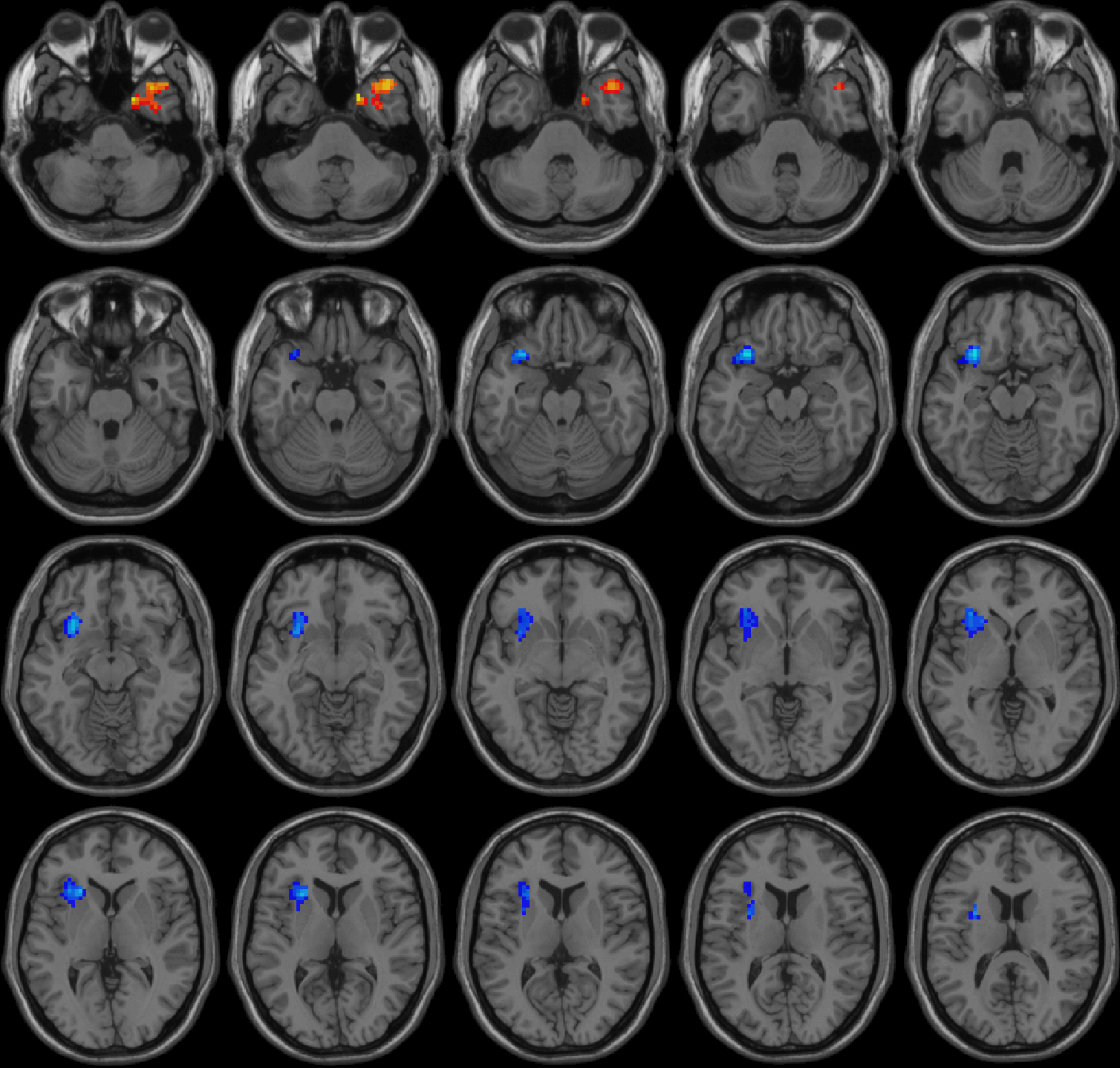
Table 1 shows the longitudinal whole-brain changes in ReHo pre- and post-RT. There were significantly increased ReHo in the bilateral cerebellum and the right inferior temporal gyrus in NPC patients at EDS compared to the pre-RT stage, as shown in Figure 1. Significantly increased ReHo F in the right temporal pole/middle temporal gyrus, and decreased ReHo in left Insula were found at LDS compared to pre-RT, as shown in Figure 2. The ReHo value was significantly lower in the right inferior temporal gyrus at LDS compared to EDS, as shown in Figure 3. In healthy controls, there were no significant ReHo changes among the three time points. All above results were reported at the significant level of a threshold of two-tailed voxel-wise p < 0.01 and cluster level p < 0.05 with Gaussian Random Field (GRF) correction. The multivariate regression analysis showed that the logistic regression model combining the three variables (mean ReHo, age and dose) has the highest diagnostic efficiency according to the area under the curve (AUC) score of the ROC curves (AUC=0.752, p=0.023), as shown in Figure 4.
Disscussion and Conclusions
Acknowledgements
This work was supported by the grants from the National Natural Science Foundation of China (81401399, 81201084, and 81560283), the Fundamental Research Funds for the Central Universities (15ykpy35), the Natural Scientific Foundation of Jiangxi Province, China (20151BAB205049), and the Medical Scientific Research Foundation of Guangdong Province (B2014162).References
1. Ding Z, Zhang H, Lv XF, et al. Radiation-induced brain structural and functional abnormalities in presymptomatic phase and outcome prediction. Hum Brain Mapp 2018; 39(1):407-427.
2. Song XW, Dong ZY, Long XY, et al. REST: a toolkit for resting-state functional magnetic resonance imaging data processing. Plos One 2011; 6(9):e25031.
Figures