3781
fMRI Mapping of Cognitive Brain Networks Involved in Perceptual Bias1Brain Networks & Neurophysiology Lab, Halifax, NS, Canada, 2Department of Research, Nova Scotia Health Authority, Halifax, NS, Canada, 3Biomedical Translational Imaging Centre, Halifax, NS, Canada, 4Department of Anesthesia, pain management, and perioperative medicine, Dalhousie University, Halifax, NS, Canada, 5Pain Management Unit, QEII Health Sciences Centre, Halifax, NS, Canada, 6School of Biomedical Engineering, Dalhousie University, Halifax, NS, Canada, 7Department of Physics and Atmospheric Science, Dalhousie University, Halifax, NS, Canada, 8Department of Diagnostic Radiology, Dalhousie University, Halifax, NS, Canada, 9Department of Medical Neuroscience, Dalhousie University, Halifax, NS, Canada
Synopsis
Prior expectations are critical in the formation of perceptions around phenomona such as pain. This study uses functional MRI to elucidate regions associated with both top-down and bottom-up aspects of pain perception, finding a network of higher-cortical regions for the former and primarily sensory regions for the latter. Additionally, bias towards cues rather than actual pain stimuli was both hypothesized and observed. The findings therefore shed light on the physiological basis of neural activation behind the complex and highly-biased formation of pain perceptions.
Introduction
Prior predictions are fundamental in organizing sensory inputs during perception. Thus, prior information has a significant influence on perceived pain intensity. Functional magnetic resonance imaging (fMRI) is used in this work to study how higher-order schemas influence pain perception through the mapping of brain networks that mediate perceptual bias in pain perception.
To do this, a novel cognitive paradigm was implemented for use with high temporal resolution multiband fMRI. This paradigm was designed to quantify the extent to which a schema can bias evaluations of heat pain stimuli, where numbers expressed magnitude of incoming pain to establish a linear schema. In a separate run, the schema was challenged by systematically increasing prediction error (difference of predicted stimulus to actual stimulus), and thus association between presented cue and stimulus magnitude was made non-linear. Brain activations to heat pain stimuli and with increasing prediction error were mapped using a whole brain General Linear Model (GLM) approach with the objective of identifying regions mediating perceptual bias towards pain. Additionally, we hypothesized that pain ratings would follow a linear relation biased towards visual cues.
Methods
Inside the scanner, participants (N=39) were presented with a visual cue followed by heat pain stimuli prior to rating the pain on a scale (0-100). In a matched condition (A), predictive cue values were drawn from numbers between 1–100 increased proportionately to stimulus intensity. In mismatch level-1 condition (B), predictive values ranging between 1–40 and 61–100 were paired with moderate and high stimuli respectively, introducing a first level of prediction error. In mismatch level-2 condition (C), predictive values ranging between 1–40 and 1–100 were paired with high stimuli only, creating the highest level of prediction error.
Structural and functional data were collected on a 3.0 T MRI scanner (Discovery MR750; General Electric Medical Systems, Waukesha, WI, USA). T1-weighted brain images were acquired with field of view = 224mm×224mm; in-plane resolution = 1mm×1mm; slice thickness = 1.0mm; TR/TE = 4.4/1.908msec; flip angle = 9°. fMRI data were acquired using a multi-band EPI sequence: field of view = 216 × 216 mm; isotropic voxel size = 3mm×3mmx3mm; TR/TE = 950/30 msec. Total number of volumes was 814 for the first matched functional scan and 624 for three other functional runs. Data was preprocessed using standard methods and activations were mapped using FLAME 1 at p<0.05 (FSL).
Results and Discussion
Brain regions mediating perceptual bias in pain towards top-down cues were mapped by comparing activations during painful stimulation between the highest and lowest level of prediction errors using whole brain correction at p< 0.05 (Flame 1) for the high stimulus. A network of multimodal cognitive brain regions was seen to track the predictive cue values (“top-down” regions), including the left ventrolateral prefrontal cortex (vlPFC), left dorsolateral prefrontal cortex (dlPFC), left inferior/superior parietal lobule (IPL/SPL), left lateral orbitofrontal cortex (lOFC) and right ventromedial prefrontal cortex (vmPFC)/medial OFC. For each region, brain activation (parameter estimates) were extracted for events at four levels of prediction error.
Opposite contrast mapped a set of pain processing regions (“bottom-up”): the secondary somatosensory cortex, dorsal posterior insula (S2/dpINS), middle insula (mINS), putamen, nucleus cuneiformis (NCF) of the right hemisphere.
As additionally hypothesized, pain ratings linearly followed cues in a matched condition (A) (P< 0.001). In condition (B), pain responses closely matched the linear schema, and the mean percentages of pain response informed by the cue for moderate and high stimuli were 92.1% and 95.9%, respectively. In condition (C), the mean percentages of pain response informed by the cue with high stimulus decreased to 77.8% but the effects of the linear schema on pain ratings persisted.
Importantly, fMRI demonstrated that when responses were ranked based on ascending cue values with constant stimulus temperature, all regions showed graded response corresponding with predictive values. Activations in the “top-down” system were highest for high prediction error events and less for low prediction error. “Bottom-up” regions showed attenuated responses to events in which prediction error was high, and were activated more when predictive cue values were higher.
Conclusions
Our findings describe brain regions implicated in modulation of expectations resulting from learned associative rules. Even when sensory inputs are significantly modified, perceived pain is modulated to fit established models. This offers new insight on the subjective nature of pain and demonstrate bias in pain perception towards top-down information. Brain systems mediating top-down effects are those involved in cognitive processing of working memory, learning, reward and motivation. In contrast, a set of sensory regions encodes alterations in perceived pain intensity.Acknowledgements
The authors would like to acknowledge funding from an NSERC Discovery grant, CIHR CRC Program, CFI, Nova Scotia Health Authority (NSHA) Establishment Grant, NSHA Fibromyalgia grant, Dalhousie start-up funds to J.A.Hashmi, Radiology Research Fund to S.Beyea, 2017R1A6A3A03003741 (Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Education) to M. Lim.References
Friston, K.J., Holmes, A.P., Worsley, K.J., Poline, J.P., Frith, C.D. and Frackowiak, R.S., 1994. Statistical parametric maps in functional imaging: a general linear approach. Human brain mapping, 2(4), pp.189-210.
Smith, S. M., Jenkinson, M., Woolrich, M. W., Beckmann, C. F., Behrens, T. E., Johansen-Berg, H., ... & Niazy, R. K. (2004). Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage, 23, S208-S219.
L. Y. Atlas, N. Bolger, M. A. Lindquist, T. D. Wager, Brain mediators of predictive cue effects on perceived pain. J Neurosci30, 12964-12977 (2010).
E. K. Miller, The prefrontal cortex and cognitive control. Nat Rev Neurosci1, 59-65 (2000)
Figures
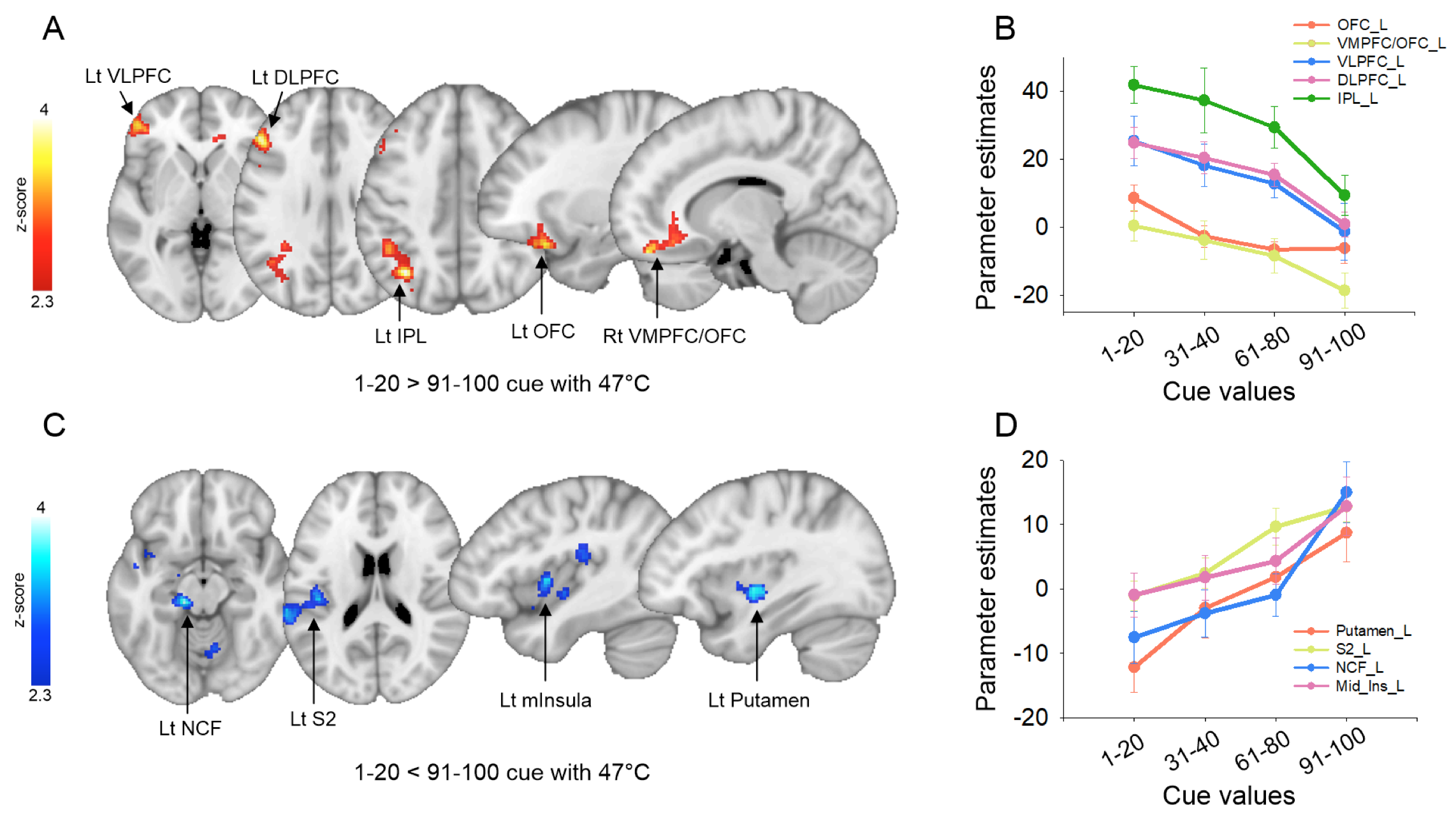
Figure 1 (A) Brain regions where low cue values have significantly higher activation than high cue values with high pain stimuli and, (B) parameter estimates of these regions. (C) Brain regions where high cue values have significantly higher activation than low cue values with high pain stimuli and (D) parameter estimates of these regions.