3732
Distinct Patterns of Interhemispheric Connectivity in Patients with Early- and Late-Onset Alzheimer’s Disease1The 2nd Affiliated Hospital of Zhejiang University, School of Medicine, Hangzhou, China, 2GE Healthcare Shanghai, Shanghai, China
Synopsis
Early-onset Alzheimer’s disease (EOAD) presents a different clinical profile than late-onset Alzheimer’s disease (LOAD). We used voxel-mirrored homotopic connectivity (VMHC) to examine interhemispheric functional connectivity and tract-based spatial statistics (TBSS) to reflect the diffusion index. We found EOAD patients exhibited more widely disrupted interhemispheric functional and structural connectivity, which related to executive deficits. Our study suggested that different interhemispheric connectivity damage patterns may contribute to the distinctclinical profiles in EOAD and LOAD.
Introduction
Although sharing the same neuropathological hallmarks, Early-onset Alzheimer’s disease (EOAD) and late-onset Alzheimer’s disease (LOAD) features different clinical characteristics. Previous studies has proposed AD as a disconnection syndrome, to some extent, that features a potential decrease in interhemispheric connectivity1. Currently, voxel-mirrored homotopic connectivity (VMHC) is effective in assessing interhemispheric resting-state functional connectivity(RSFC) by quantifying the RSFC in one hemisphere andits mirrored counterpart in the other. Moreover, based on the hypothesis that there is a strong link between structural and functional connectivity, Diffusion indices, including fractional anisotropy (FA), mean diffusivity (MD), axialdiffusivity (AxD) and radial diffusivity (RD), were also used to assess interhemispheric structural connectivity2.
Method
According to the arbitrary cut-off age of 65, we included 22 EOAD patients,27 LOAD patients and 38 healthy controls (further divided into 21 relatively youngand 17 old controls). Participants underwent resting-state functional MRI, diffusiontensor imaging (DTI) and comprehensive neuropsychological assessments. We usedvoxel-mirrored homotopic connectivity (VMHC) to examine interhemispheric functionalconnectivity. Then, we calculated the diffusion index based on tract-based spatialstatistics (TBSS). Two-sample t-tests were used to assess the interhemisphericconnectivity differences between each patient group and its corresponding control group.Results
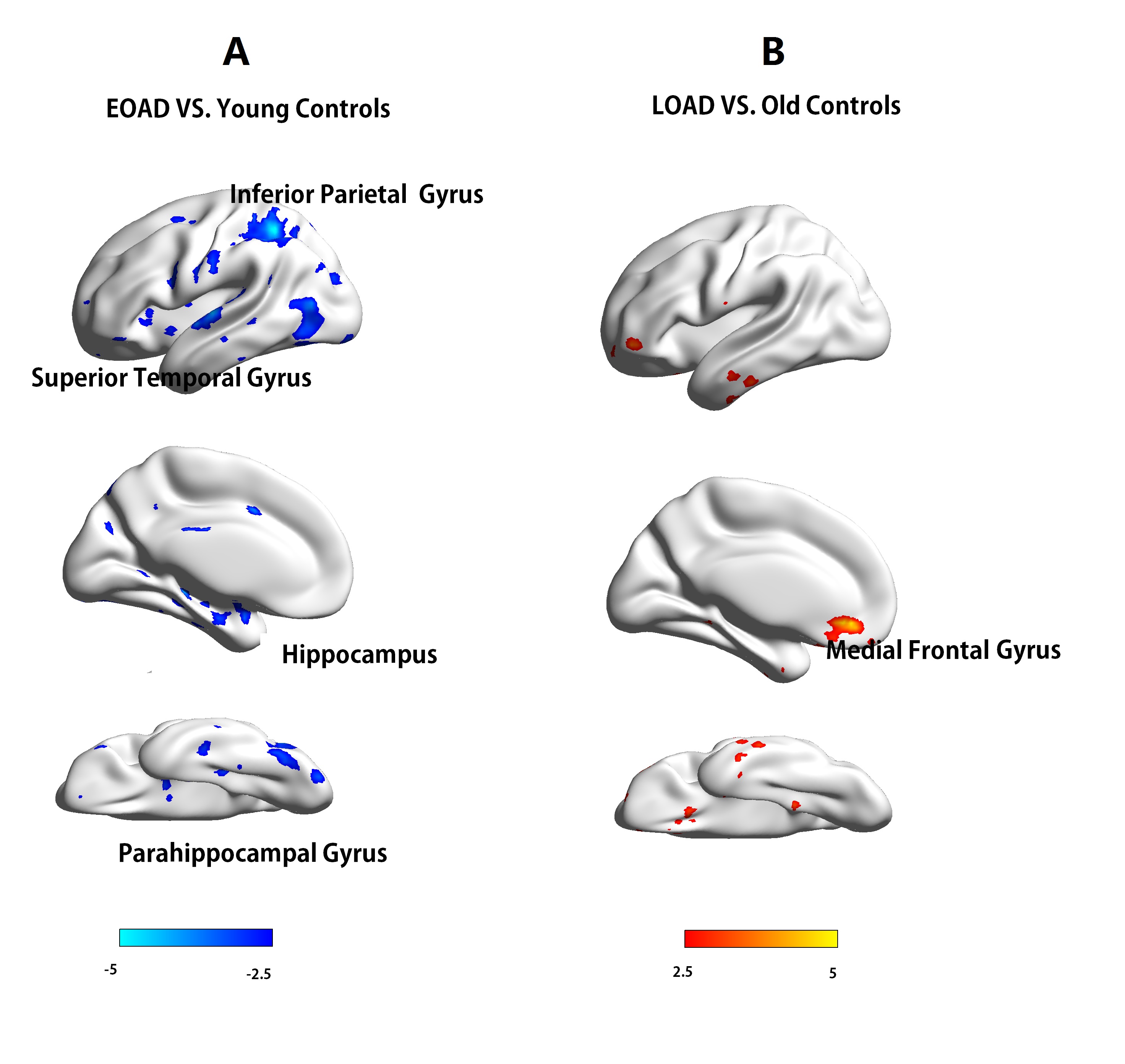
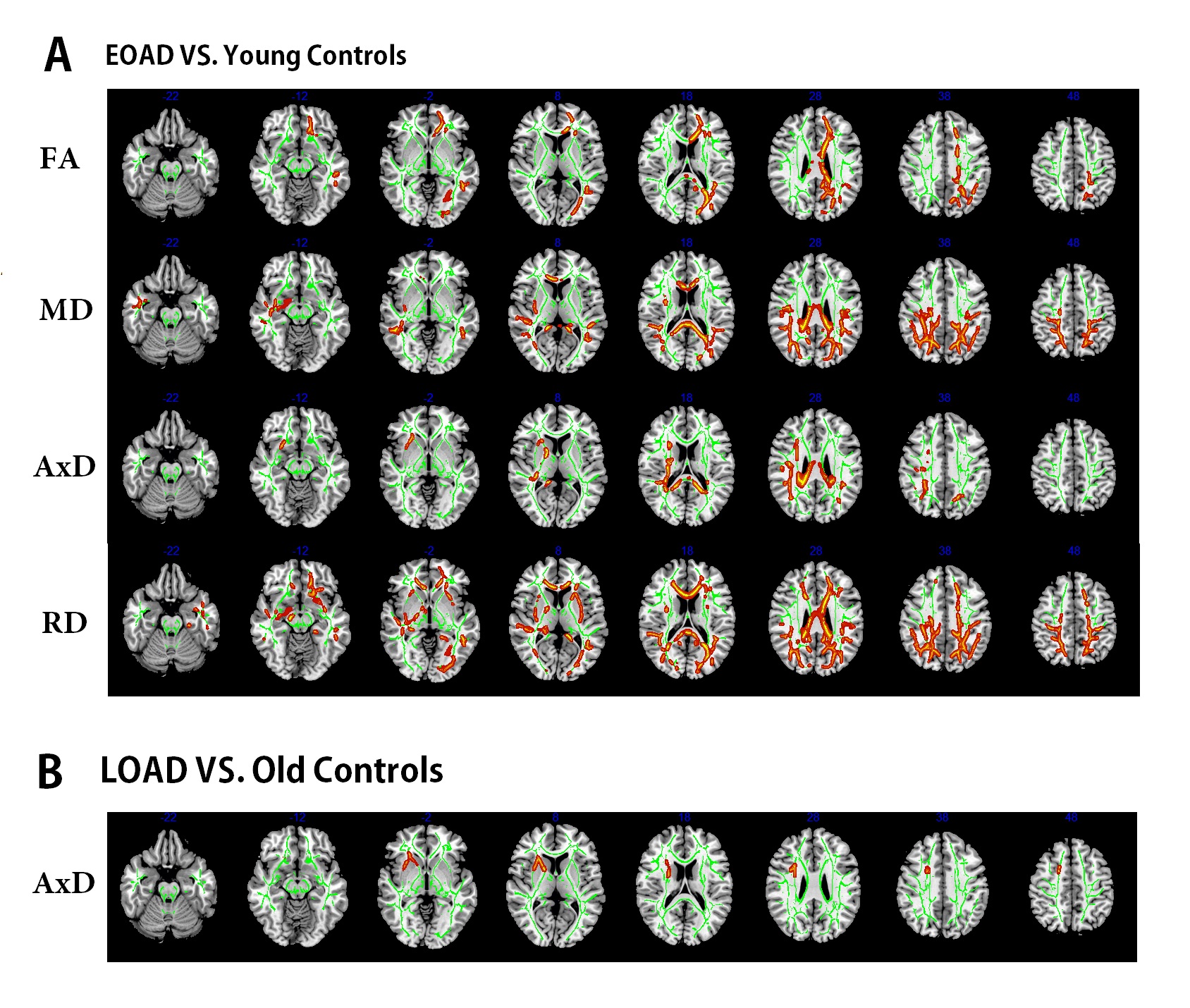
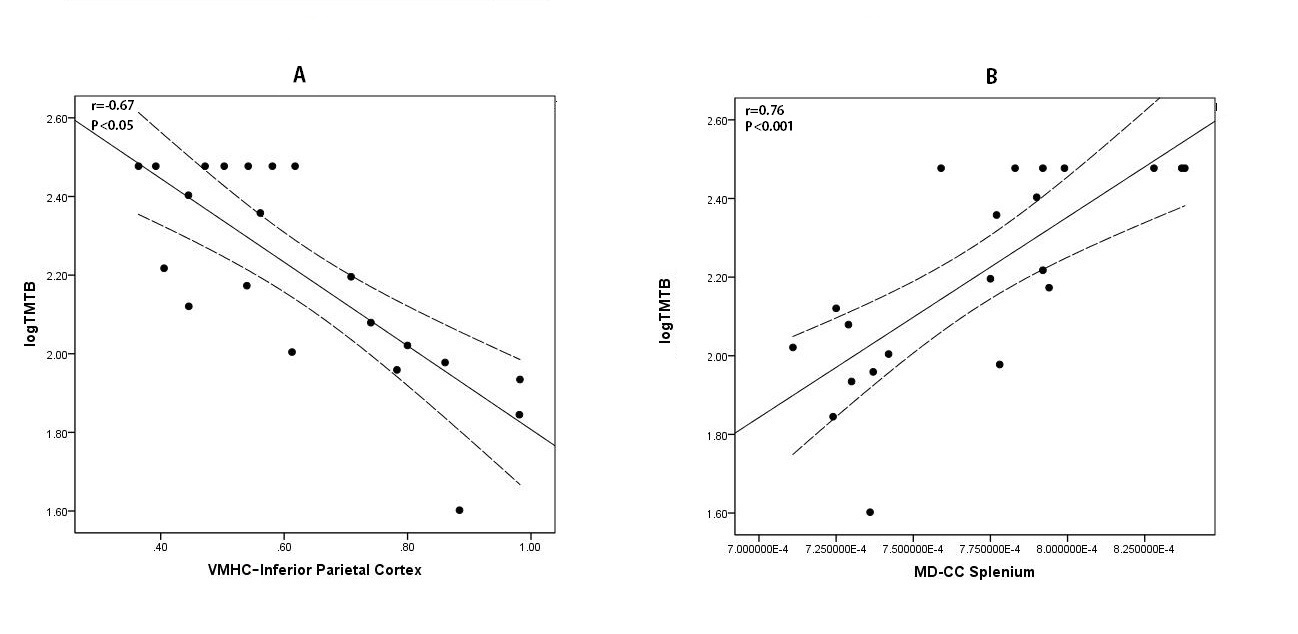
We found that the EOAD patients had lower VMHC in the hippocampus,parahippocampal gyrus (PHG), superior temporal gyrus (STG) and inferior parietal cortex(IPC) than did controls. Consistently, the EOAD patients exhibited white matter (WM) tract impairment in the posterior regions. On the other hand, the LOAD patients displayed increased VMHC and impaired WM tracts in the frontal region. Correlation analyses showed that VMHC in the IPC was related to executive function in the EOAD patients(r = -0.67, P < 0.05).Discussion
In this study, we observed decreased interhemispheric RSFC in the HP, PHG and IPG in the EOAD patients. Moreover, we also found widespread white matter changes in EOAD which had a good location match with VMHC impairments. And these structures are in charge of information encoding and convergence and are tightly associated with declarative memory.Our results extended previous rsfMRI studies that documented impaired functional connectivity in the HP and PHG in EOAD and further found interhemispheric functional connectivity impairments. And further analysis showed the white matter and functional connectivity in parietal region significantly correlates with executive function in EOAD. These results conclusively suggested that severe functional and structural connectivity impairment may be the key mechanism underlying EOAD. On the other hand, LOAD patients have showed relatively intact nterhemispheric functional connectivity which may be a compensatory changes based on the relatively intact white matter fibers. And the hippocampus atrophy but not the functional disconnection may be the main reason of memory loss in LOAD.
Conclusion
In contrast to the LOAD patients, patients with EOAD exhibited more widely disrupted interhemispheric functional and structural connectivity, which overlapped well across brain regions. In addition, for the EOAD patients, decreased interhemispheric connectivity related to executive deficits. Our study suggested that different interhemispheric connectivity damage patterns may contribute to the distinct clinical profiles in EOAD and LOAD.Acknowledgements
No acknowledgement found.References
1. Liu, Y., Yu, C., Zhang, X., Liu, J., Duan, Y., Alexander-Bloch, A. F.,et al. (2014). Impaired long distance functional connectivity and weightednetwork architecture in Alzheimer’s disease. Cereb. Cortex 24, 1422–1435.doi: 10.1093/cercor/bhs410
2.Li, H., Liang, Y., Chen, K., Li, X., Shu, N., Zhang, Z., et al. (2013). Differentpatterns of white matter disruption among amnestic mild cognitive impairmentsubtypes: relationship with neuropsychological performance. J. Alzheimers Dis.36, 365–376. doi: 10.3233/JAD-122023
Figures