3688
Altered bilateral functional connectivity in rat brain under isoflurane and medetomidine anesthesia1CIBM-AIT, École polytechnique fédérale de Lausanne, Lausanne, Switzerland
Synopsis
Anesthetic agents are commonly used in rodent resting-state functional MRI. When anesthetized under different agents, brain functional connectivity can be altered. It has been shown that after isoflurane initiation, brain connectivity measured under medetomidine was extensively affected in a time-dependent manner. Here, we further compare the difference of resting-state networks detected under isoflurane and medetomidine anesthesia.
Introduction
Anesthetic agents are commonly used in rodent resting-state functional MRI (rs-fMRI). When anesthetized under different agents, brain functional connectivity can be altered. Medetomidine is one of the most widely used anesthetic, which preserves a robust and reproducible brain activity. To ensure a stable anesthesia, medetomidine is frequently applied after initial induction under isoflurane. However, both isoflurane and medetomidine can affect brain function, and show as time/dose dependent effects (1–3). A previous study demonstrated that after 60 minutes of isoflurane initiation, brain connectivity measured under medetomidine was extensively affected in a time-dependent manner (4). Here in this study, we further compare the difference of resting-state networks detected under isoflurane and medetomidine anesthesia.Methods
All animal experiments were approved by the local animal ethical committee and performed on a 14.1 T system. Seven Sprague-Dawley rats were anesthetized with isoflurane (mixed with air/oxygen of 70%/30%) at 4% for induction, and 2% for maintenance. After the first sets of rs-fMRI measurements, 0.1 mg/kg medetomidine was administered through a subcutaneous bolus injection; 10 minutes after bolus, isoflurane was discontinued; s.c. medetomidine infusion at a rate of 0.1 mg/kg/h started 15 minutes after the bolus. Rs-fMRI runs were performed during medetomidine infusion in three stages: 23-33 minutes, 70-75 minutes and 107-113 minutes after the bolus.
Anatomic scans were acquired using fast spin-echo sequence (0.14×0.15 mm2, 128×64 matrix, slice thickness=0.5mm, TR/TE=2500/20ms). Two-shot GRE-EPI sequence was used for rs-fMRI measures with a temporal resolution of 1.6 s (0.36×0.36mm2, 64×64 matrix, slice thickness=1 mm, 9 slices, TR/TE=800/10ms). A total of 370 volumes were acquired in 10 minutes. Two extra EPI runs (10 volumes) with opposite phase encoding direction were acquired for susceptibility distortion correction.
Resting-state fMRI data pre-processing included brain extraction, denoising (5), distortion correction in FSL (6), slice time correction, spatial smoothing (0.36mm kernel) and high-pass filtering of 0.02Hz. Anatomic and fMRI scans were co-registered to an atlas space, with atlas labels transformed back to each rs-fMRI data. Pre-processed rs-fMRI data was decomposed into 50 independent components (IC) using FSL’s MELODIC software (6), components related to respiration and cardiac noise were removed from rs-fMRI data. MELODIC cleaned data was used to calculated functional connectivity (FC) matrix from 30 bilateral brain regions. Kruskal-Wallis one-way ANOVA were performed to assess the difference of FC matrix under two anesthesia conditions. In addition, rs-fMRI data under the same anesthesia condition were concatenated and analyzed using group-ICA approach (30 components).
Results
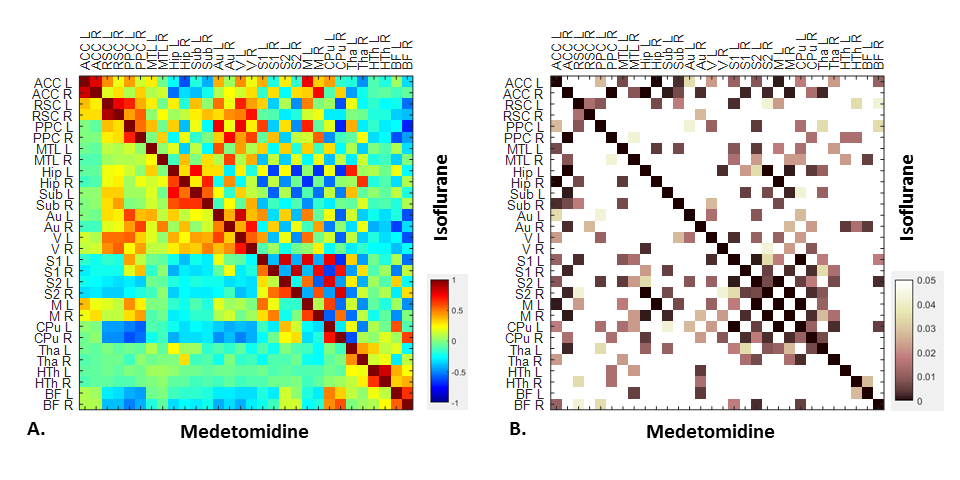
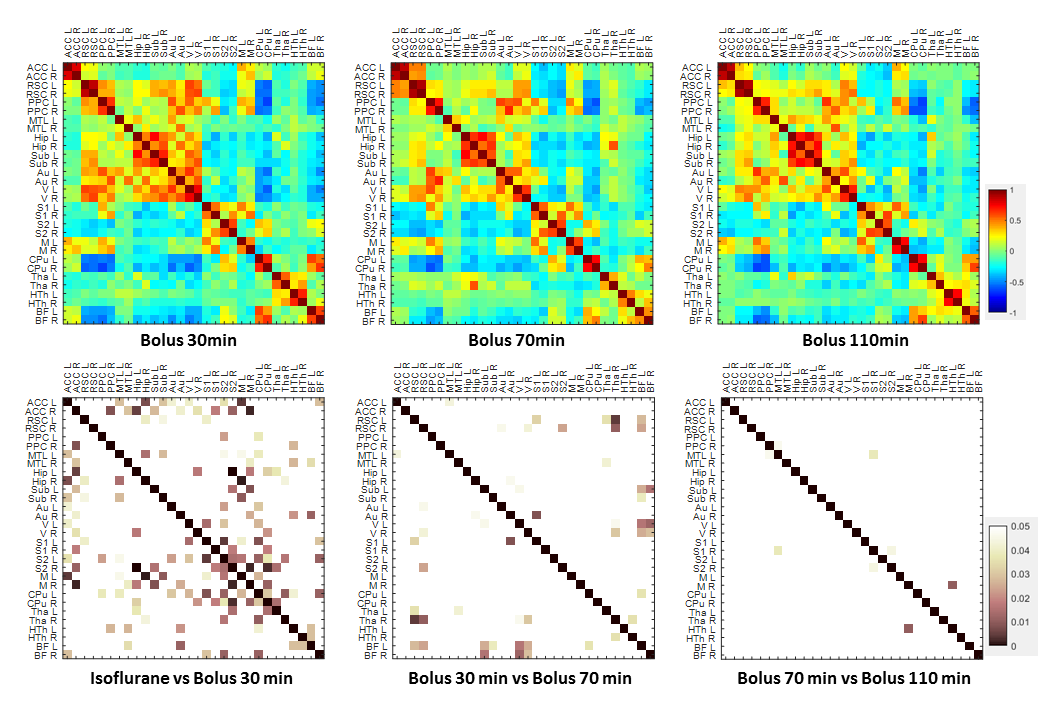
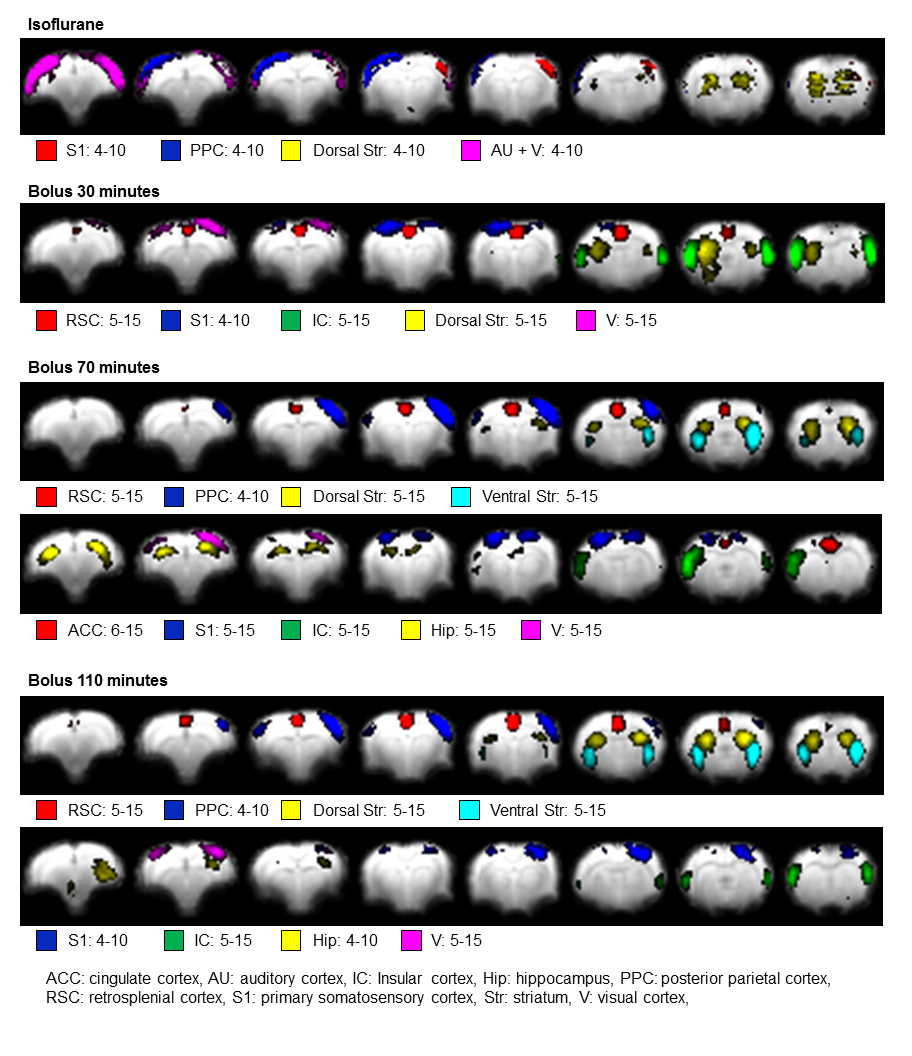
In general, compared to medetomidine, strong unilateral connectivity was observed in primary/secondary somatosensory cortex (S1/S2), motor cortex (M) and thalamus (Tha) regions under isoflurane anesthesia (Fig. 1, Fig. 2). Auditory and visual cortex function were persevered under isoflurane, while decreased function was detected in striatum, there was decreased connection between cingulate cortex (ACC) and retrosplenial cortex (RSC) as well (Fig. 2, Fig. 3). Around 30 minutes after medetomidine bolus injection, bilateral networks were recovered from somatosensory, motor cortex and thalamus as shown on the connectivity matrix. For ventral striatum, bilateral networks were visible one hour after bolus injection at the earliest (Fig. 2, Fig. 3). There were no significant differences between brain networks for durations longer than one hour since bolus.Discussion and conclusion
For rodent rs-fMRI research conducted under isoflurane and medetomidine anesthesia, the dose and timeline of anesthesia is highly important. To provide comparable and reliable brain connectivity, it is essential to control the timeline for data acquisition under different anesthetics. In most cases, animal preparations (induction, surgery, animal mobilization, scanner setups) were performed under isoflurane anesthesia, then switched to medetomidine for rs-fMRI acquisition. Here in this study, we demonstrated that most bilateral network was recovered after 30 minutes of medetomidine bolus injection. But to obtain more stable brain activities, it is recommended to measure rs-fMRI networks at least one hour after isoflurane being discontinued.Acknowledgements
The authors thank Analina da Silva, Mario Lepore and Stefan Mitrea for assistance with animal setup and monitoring. This work was supported by the Centre d’Imagerie BioMédicale (CIBM) of the UNIL, UNIGE, HUG, CHUV, EPFL and the Leenaardsand Louis-Jeantet Foundations.References
1. Bukhari Q, Schroeter A, Cole DM, Rudin M. Resting State fMRI in Mice Reveals Anesthesia Specific Signatures of Brain Functional Networks and Their Interactions. Front. Neural Circuits 2017;11:1–11.
2. Li Q, Li G, Wu D, et al. Resting-state functional MRI reveals altered brain connectivity and its correlation with motor dysfunction in a mouse model of Huntington’s disease. Sci. Rep. 2017;7:1–9.
3. Pawela CP, Biswal BB, Hudetz AG, et al. A protocol for use of medetomidine anesthesia in rats for extended studies using task-induced BOLD contrast and resting-state functional connectivity. Neuroimage 2009;46:1137–1147.
4. Makani P, Gruetter R, Jelescu IO. Anesthesia affects connectivity of default-mode sub-networks in the rat in a time-dependent and region-dependent manner. In: Proceedings of the 25th Annual Meeting of ISMRM. 2017; p. 2304.
5. Veraart J, Fieremans E, Novikov DS. Diffusion MRI noise mapping using random matrix theory. Magn. Reson. Med. 2016;76:1582–1593.
6. Beckmann CF, Smith SM. Probabilistic Independent Component Analysis for Functional Magnetic Resonance Imaging. IEEE Trans. Med. Imaging 2004;23:137–152.
Figures