3680
HCC screening with abbreviated MRI: retrospective comparison of noncontrast, dynamic-contrast enhanced and hepatobiliary phase protocols post gadoxetic acid1Translational and Molecular Imaging Institute, Icahn School of Medicine at Mount Sinai, New York, NY, United States, 2Radiology, Icahn School of Medicine at Mount Sinai, New York, NY, United States, 3Icahn School of Medicine at Mount Sinai, New York, NY, United States, 4Columbia University, New York, NY, United States, 5Radiology, Albert Einstein College of Medicine, New York, NY, United States, 6Infectious diseases, Icahn School of Medicine at Mount Sinai, New York, NY, United States, 7Radiology, UC San Diego Medical Center, San Diego, CA, United States
Synopsis
In this study, we compare the performance of different abbreviated MRI (AMRI) protocols using 3 different sets: noncontrast, dynamic T1WI, and hepatobiliary phase (HBP) post gadoxetic acid for hepatocellular carcinoma (HCC) screening in 238 patients at risk. Our results showed that performance of noncontrast AMRI was low, while AMRI using dynamic T1WI and AMRI including HBP showed equivalent sensitivity for HCC detection with slightly better specificity for dynamic T1W. These results need verification in a larger study.
Introduction
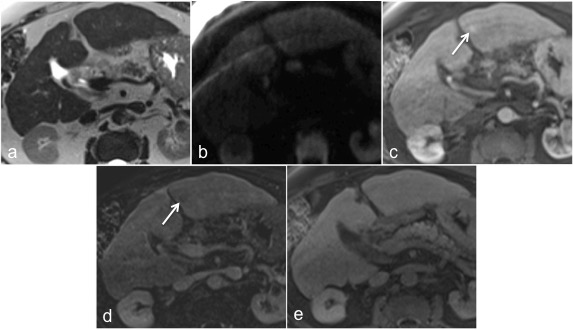
Current clinical practice guidelines recommend semi-annual surveillance with ultrasound (US) with/without serum AFP for patients at risk of hepatocellular carcinoma 1. Because of the low sensitivity of US for detecting HCC, many centers instead perform multiphasic contrast-enhanced (CE)-CT or CE-MRI. While these provide higher sensitivity than US, these are not optimal for surveillance2,3 because of higher cost, radiation exposure for CT4 and long exam duration for MRI (at least 30’). Motivated to provide a more sensitive method, novel abbreviated MRI (AMRI) surveillance strategies have been conceived. Based on preliminary data, AMRI can be performed at a lower cost than a complete CE-MRI exam, at only a slightly higher cost than an US exam, while providing up to 45% higher sensitivity at similar specificity4,5. The technique and the most accurate AMRI protocol still need to be validated. The aim of the present study was to compare the performance of different “virtual” AMRI protocols derived from a full gadoxetic acid-enhanced MRI using either noncontrast, dynamic-T1W or T1 HBP (hepatobiliary phase) sequences for HCC screening in at risk population.Methods
This initial retrospective study included 238 consecutive eligible patients (M/F 140/98, mean age 59 y) with chronic liver disease who underwent gadoxetic acid MRI in 2017 for HCC screening/surveillance in a single institution. Patients with history of HCC, liver transplantation, other malignancies, acute liver disease and non-cirrhotic HCV were excluded. Three “virtual” AMRI reading sets were extracted and assessed separately: noncontrast (NC)-AMRI (axial T2 HASTE+DWI), dynamic (Dyn)-AMRI (axial T2 HASTE+DWI+Dynamic contrast-enhanced T1W), EOB-AMRI (axial T2 HASTE+DWI+T1W HBP). Three radiologists reviewed one third of the data each while 45 MRIs were reviewed by all the radiologists for inter-reader analysis. All detected lesions were characterized using a composite scoring system for NC-AMRI and EOB-AMRI: negative (no observation), subthreshold (1 or more lesions <10mm), positive (1 or more ≥ 10mm nodules or distinctive area(s) of heterogeneity not attributable to cirrhosis, cysts or hemangiomas). The LI-RADS v2018 algorithm was used to score the lesions with Dyn-AMRI. LI-RADS 5 lesions were considered HCC on Dyn-AMRI. The reference standard was determined by two different radiologists that reviewed all available patient data, by classifying the patient with or without HCC. Per-patient sensitivity and specificity were calculated using Mc Nemar’s test. Inter-reader agreement was assessed using Cohen’s Kappa coefficient.Results
Reference standard demonstrated 13/238 patients (5.4%) with HCC (mean size 33.7±30mm, range: 10-120mm). Per-patient sensitivities were 53.8% for NC-AMRI (95%CIs: 25.1-80.7, 7/13 HCCs, mean size of missed lesions: 16mm, range: 10-19mm), 84.62% for Dyn-AMRI (95%CIs: 54.55-98.08, 11/13 HCCs, mean size of missed lesions: 16mm, range: 13-19) and 69.2% for EOB-AMRI (95% CIs: 38.5-90.9, 9/13 HCCs, mean size of missed lesions: 15mm, range: 10-19mm), with a significant difference between NC-AMRI and Dyn-AMRI as shown by NC-AMRI value not overlapping Dyn-AMRI 95%CIs. Per-patient specificities were 96.4% (95%CIs: 93.1-98.4, 217/225), 97.3% (95%CIs: 94.2-99.0, 219/225) and 93.7% (95%CIs: 89.7-96.5, 211/225), respectively, with a significant difference between EOB-AMRI and Dyn-AMRI. Inter-reader agreement was moderate for NC-AMRI and EOB-AMRI (k=0.56) and substantial for Dyn-AMRI (k=0.65).Discussion
Our results show a low sensitivity for HCC detection using NC-AMRI protocol, significantly lower than Dyn-AMRI, in line with ultrasound sensitivity2. The use of contrast is still needed in AMRI protocols4–9. Dyn-AMRI showed a better specificity and better inter-reader agreement, with equivalent sensitivity comparing to EOB-AMRI (9 vs. 11 HCC detected using EOB vs. Dyn-AMRI protocols, respectively). The study will be extended to a larger sample size to confirm these initial results.Conclusions
In this initial study, the diagnostic performance for HCC screening with AMRI seems to be slightly in favor of Dyn-AMRI. The study will be extended to a larger number of cases for further confirmation. The use of contrast in the AMRI protocol is required to achieve sufficient sensitivity.Acknowledgements
No acknowledgement found.References
1. Heimbach, J. K. et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatol. Baltim. Md 67, 358–380 (2018).
2. Colli, A. et al. Accuracy of ultrasonography, spiral CT, magnetic resonance, and alpha-fetoprotein in diagnosing hepatocellular carcinoma: a systematic review. Am. J. Gastroenterol. 101, 513–523 (2006). 3. Arguedas, M. R., Chen, V. K., Eloubeidi, M. A. & Fallon, M. B. Screening for hepatocellular carcinoma in patients with hepatitis C cirrhosis: a cost-utility analysis. Am. J. Gastroenterol. 98, 679–690 (2003).
4. Besa, C. et al. Hepatocellular carcinoma detection: diagnostic performance of a simulated abbreviated MRI protocol combining diffusion-weighted and T1-weighted imaging at the delayed phase post gadoxetic acid. Abdom. Radiol. N. Y. 42, 179–190 (2017).
5. Marks, R. M. et al. Diagnostic Per-Patient Accuracy of an Abbreviated Hepatobiliary Phase Gadoxetic Acid–Enhanced MRI for Hepatocellular Carcinoma Surveillance. Am. J. Roentgenol. 204, 527–535 (2015).
6. Tillman, B. G. et al. Diagnostic per-lesion performance of a simulated gadoxetate disodium-enhanced abbreviated MRI protocol for hepatocellular carcinoma screening. Clin. Radiol. 73, 485–493 (2018).
7. Lee, D. H. Imaging evaluation of non-alcoholic fatty liver disease: focused on quantification. Clin. Mol. Hepatol. 23, 290–301 (2017).
8. Goossens, N. et al. Cost-Effectiveness of Risk Score-Stratified Hepatocellular Carcinoma Screening in Patients with Cirrhosis. Clin. Transl. Gastroenterol. 8, e101 (2017).
9. Goossens, N., Bian, C. B. & Hoshida, Y. Tailored algorithms for hepatocellular carcinoma surveillance: Is one-size-fits-all strategy outdated? Curr. Hepatol. Rep. 16, 64–71 (2017).
Figures