3679
A Dedicated Head-Only MRI Scanner for Point-of-Care ImagingAlex Panther1, Gilbert Thevathasen1, Ian R.O. Connell2, Yi Yao1, Curtis N Wiens1, Andrew T Curtis1, Geron A Bindseil1, Chad T Harris1, Philip J Beatty1, Jeff A Stainsby1, Charles H Cunningham3, B A Chronik2, and Cameron Piron1
1Synaptive Medical, Toronto, ON, Canada, 2Department of Physics and Astronomy, University of Western Ontario, London, ON, Canada, 3Department of Medical Biophysics, Physical Sciences, Sunnybrook Research Institute, Toronto, ON, Canada
Synopsis
A dedicated head-specific MRI is presented. The MRI is designed to address many of the siting and installation requirements to better allow the use of MRI in point-of-care imaging.
Introduction
The clinical value of MRI imaging has transformed healthcare, and the number of MRI exams performed grows yearly. The value of MRI can be further increased if MRI can be applied to areas outside the diagnostic imaging department. MRI could provide clinical value in point-of-care imaging, such as in the Emergency Department where acute stroke patients cannot tolerate transport time (1), or in the intensive care unit where critically ill patients are too ill for transport to the imaging department (2). Realizing the value of MRI in point-of-care contexts is impeded by many challenges. Here we examine how one might design a system to address common problems associated with expansion of MRI imaging outside of the diagnostic imaging department. Below we list many of the challenges alongside engineering choices to address them.Barriers to MRI installation
- Size: The large size of a whole-body MRI typically requires rigging and building modification for installation. The head-specific MRI system that we have developed measures 104 cm in length with a height of 7'0" (213 cm). Thus it can be installed through a typical loading dock and elevator without modification.
- Weight: MRIs often require building structural modifications due to their weight. Our dedicated head MRI weighs under 2500 lbs, enabling installation on typical concrete flooring. Also, this weight is typically acceptable for installation via elevator.
- Vibration: MRIs are sensitive to building vibrations, and thus at or below-grade installations are preferred. Vibration isolation has been directly integrated into our proposed design, allowing installation on upper floors where vibration specifications may exceed those typically required.
- Fringe Fields: Square footage in a hospital is always at a premium, and MRIs can have a large installation footprint due to their fringe fields. The American College of Radiology has defined a 4-zone MRI installation, with restricted access requirements for Zones III and IV, as stray magnetic fields often exist outside of Zone IV, the exam room. When energized, our proposed MRI has a 5 Gauss line measuring less than 1.03 m from the outer edge of the magnet enclosure, ensuring that no stray field is present outside of the exam room. When the system is not energized, no fringe fields exist. This allows installation of this system into areas of less than 300 square feet, including the equipment room and operator area.
- Venting of Cryogens: The requirement for a cryogen venting system can significantly increase the cost of an MRI installation. This MRI has been built as a closed conduction cooled system, such that no cryogen vent is required.
- Safety: In point-of-care MRI, imaging systems would be located outside of the traditional diagnostic imaging department, where MRI safety is an important concern. We have developed an MRI that can be rapidly ramped (in <15 minutes) when needed for imaging, and otherwise idle in a non-magnetic state.
Barriers to MRI being used at the point-of-care
- Device safety: The number of implanted medical devices is growing at a high rate. With a head-only MRI, gradient fields and RF fields drop significantly outside of the gradient and volume transmit coils, allowing safer imaging of patients with body implants. Due to the small fringe field, it is possible to image the brain while the lower body is in a field significantly less than the static main field B0. By working at mid-field (0.5 T), RF heating is significantly reduced compared to high-field MRI systems, as RF heating is proportional to the square of the field strength.
- Image quality: For MR imaging to be used at the point of care, in addition to mitigating the issues above, the images must be clinically relevant. To achieve that, we have built a system with the following features chosen to optimize image quality:
- High-performance gradients: Gradients with a peak gradient strength of 100 mT/m and a slew rate of 400 T/m/s can be used to reduce echo times in DWI and reduce gradient rewinder and prewinder times.
- Large peak B1+: Low RF heating at 0.5 T allows the head-only MRI system to achieve peak B1+ levels above 50 uT without exceeding patient heating limits. This B1+ can be leveraged for shorter echo trains and higher bandwidth RF pulses.
- Adjustable multi-channel receive-only head coil: Movable side and top panels allow optimal coil placement, and allow for intubated patients, patients with potential fixtures, bandaging, etc.
Conclusion
From the above design considerations, we have realized an MRI system capable of providing clinically relevant images in a manner tailored for point-of-care imaging.Acknowledgements
No acknowledgement found.References
[1] 2018 Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association, Powers et al., Stroke, Vol. 49, No. 3
[2] Complications during intrahospital transport of critically ill patients: Focus on risk identification and prevention, Knight et al., Int J Crit Illn Inj Sci. 2015 Oct-Dec; 5(4): 256–264.
Figures
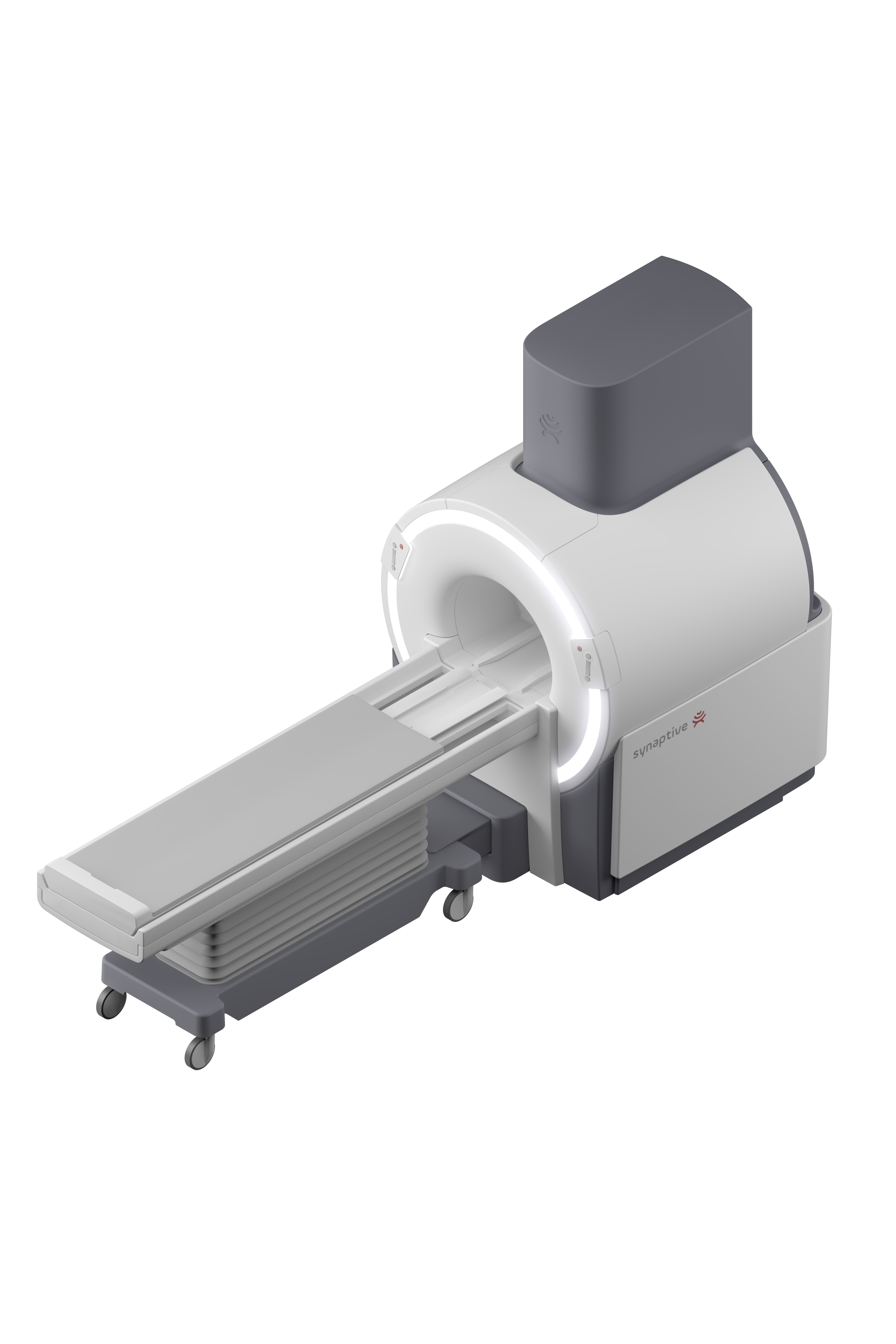
Isometric view of dedicated head-specific MRI scanner.

Plan view of dedicated head-specific MRI scanner showing extent of 5 Gauss line.

Sample T2 and T2-FLAIR images from the proposed MRI system.