3674
The prognostic value of detailed MRI reports in predicting the progress-free survival of patients with nasopharyngeal carcinoma1Department of Radiology, Sun Yat-sen University Cancer Center, Guangzhou, China
Synopsis
To evaluate the prognostic value of detailed MRI reports for progress-free survivals (PFS) of patients with Nasopharyngeal Carcinoma (NPC) who underwent intensity modulated radiation therapy (IMRT), we used Cox regression to analyze all the variables of detailed MRI reports and to build a new nomogram for PFS. Our results demonstrated that the new nomogram was more efficient than the American Joint Committee on Cancer (AJCC) 8th staging system. These results indicated that detailed MRI reports could play a more important role in predicting PFS, and some significant factors may be added to improve the current staging system.
Introduction
The properties of a tumor itself were considered the main factors determining the PFS of patients with NPC treated with IMRT1. However, currently the NPC tumor was mainly evaluated by the AJCC staging system, which did not take in all the detailed anatomical structures related to NPC and had an unsatisfactory performance in prognostic prediction. This study aimed to investigate the prognostic value of the detailed MRI reports based on anatomy and morphology, and to determine whether these parameters could help to improve the current staging system.Materials and methods
Participants 792 consecutive patients with histologically proved, newly diagnosed NPC without distance metastasis were recruited respectively. These patients were placed in two groups of Training (525) and Validation (267) by the time of the first treatment. All of them were followed up for more than 5 years.
Variables 468 variables acquired via detailed MRI reports were involved. Among them, 223 variables were related to the primary tumor. The other were correlated with the properties of regional lymph nodes. Two radiologists specializing in head and neck cancers evaluated the MR images independently.
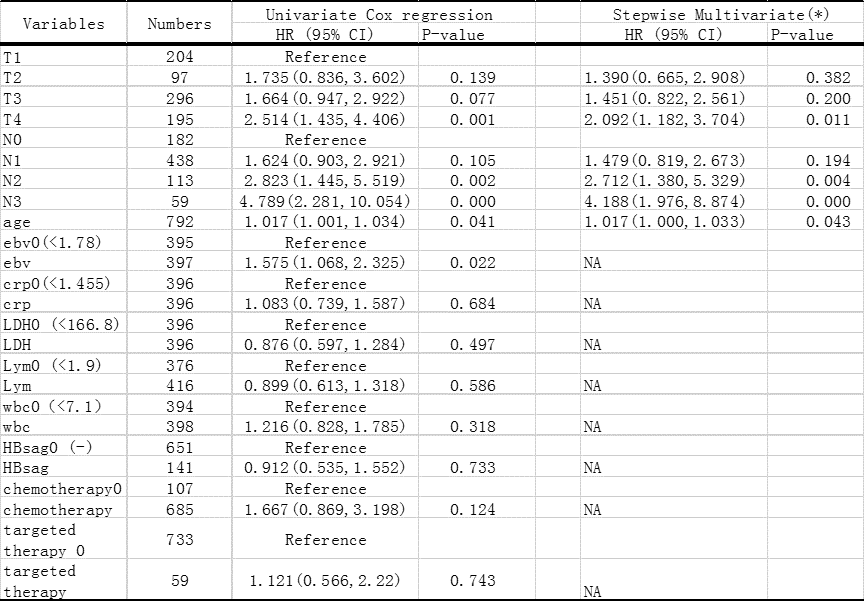
Statistical Analysis Firstly, Single-factor Cox regressing model and 10-fold cross-validation (LASSO) were applied for features reduction. Subsequently, Stepwise Cox regressing is used to build the nomogram model for PFS. The predictive accuracy and discriminative ability of the model was determined by c-index and calibration curve. And the nomogram from AJCC 8th TN Staging and age, which was the significant clinic feature selected by univariate and stepwise multivariate Cox regression (Figure 1), was used as control.
Results
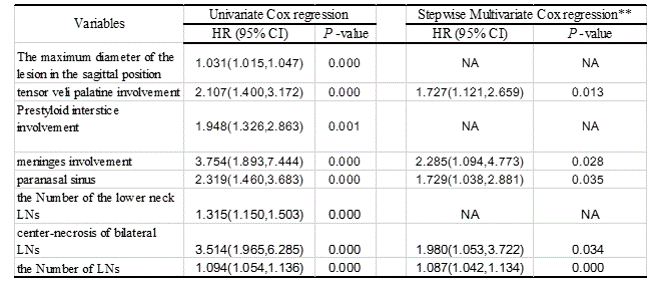
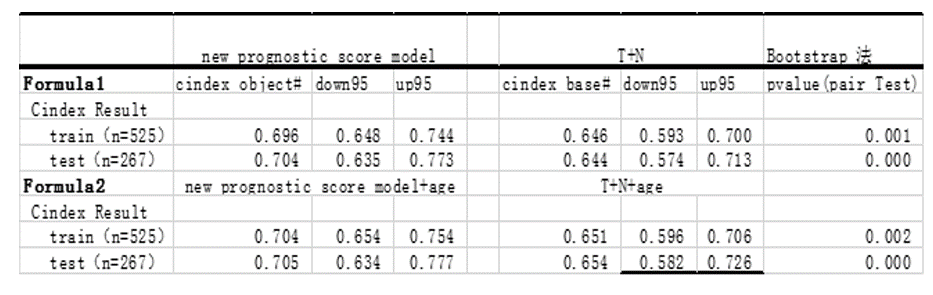
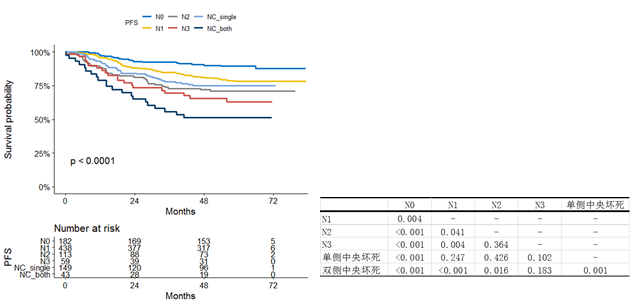
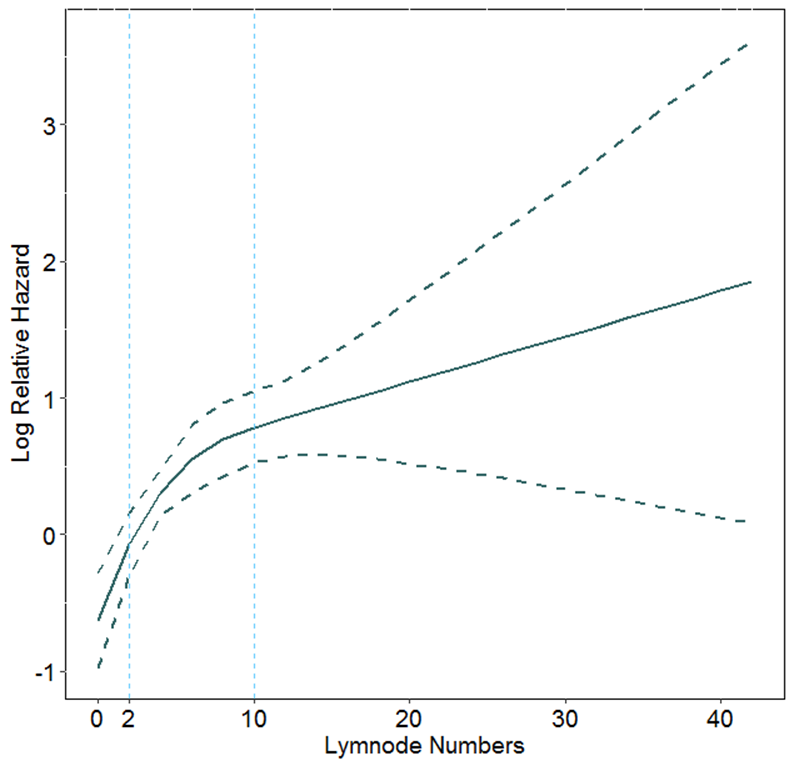
PFS was found mainly affected (P<.05) by tensor veli palatini involvement (TVPI), meninges involvement (MI), paranasal sinus (PS), center-necrosis of bilateral LNs (CNBL) and the Number of metastatic LNs (LNs) (Figure 2). These variables could be used to build the new prognostic nomogram for PFS. The new nomogram had a bootstrap-corrected C-index which was significantly(P <.001)higher than that of AJCC 8th TN classification with or without age in both the training and validation cohort (Figure 3). CNBL and NL were singled out for further study because of being not included in AJCC 8th TN Staging. The K-M analysis showed that there was no significant difference between the PFS curves of the CNBL and N3 stage (P=.183) (Figure 4). RCS data showed that the increase of Hazard ratio were followed by LNs. Moreover, when the LNs was over than 10, the growing rate became slower (Figure 5).Discussion
The current staging system is based on the anatomical extension of the tumor and the location of regional metastatic lymph nodes. However, it does not take in all the detailed anatomical structures related to NPC and the features and number of the regional metastatic lymph nodes.As far as know, this is the first study to expound the foundation and validation of a prognostic nomogram with all the data of detailed MRI reports to predict PFS for NPC patients. According to our findings, the C-index of the new nomogram was higher than the current staging system in the primary and validation cohorts, and the method is more convenient because of less variables. More to the point, new factors were proposed in this study which were significant for prognosis of NPC patients. Cervical nodal necrosis had been considered as a negative prognostic factor in patients with HNSCC (including NPC) in previous papers2-4. Our study focused on the laterality of cervical center-necrosis LNs and find that the survival outcome was similar to those in patients with N3 stage. Therefore, it may be worth considering whether CNBL should be incorporated into the current staging system for NPC. Furthermore, the number of metastatic LNs was also found as a critical prognostic factor for NPC, similar to findings for oropharyngeal, hypopharyngeal, and laryngeal cancers 5-6. This study showed that the cutoff point of 10 would be significant for NPC’s prognosis, and further research could be done to clarify the relation to current N staging.Conclusion
This study validated a novel and simple prognostic nomogram based on detailed MRI reports for predicting PFS of patients with NPC. Our data demonstrated that CNBL and LNs were independent risk factors in predicting PFS. CNBL could be an additional factor in N3 stage. Counting the number of metastatic LNs could be very important in predicting the PFS, particularly when the number was more than 10.Acknowledgements
No acknowledgement found.References
1. Qiu S, Lin S, Tham IW, Pan J, et al. Intensity-modulated radiation therapy in the salvage of locally recurrent nasopharyngeal carcinoma. Int J Radiat Oncol Biol Phys. 2012; 83:676–83.
2. Zoumalan RA, Kleinberger AJ, Morris LG, et al. Lymph node central necrosis on computed tomography as predictor of extracapsular extracapsular spread in metastatic head and neck squamous cell carcinoma: pilot study. J Laryngol Otol. 2010; 124(12):1284–1288.
3. Randall DR, Lysack JT, Hudon ME, et al. Diagnostic utility of central node necrosis in predicting extracapsular spread among oral cavity squamous cell carcinoma. Head Neck. 2015; 37(1):92–96.
4. Puri SK, Fan CY, Hanna E. Significance of extracapsular lymph node metastases in patients with head and neck squamous cell carcinoma. Curr Opin Otolaryngol Head Neck Surg. 2003; 11(2):119–123.
5. Ho AS, Kim S, Tighiouart M, et al. Metastatic Lymph Node Burden and Survival in Oral Cavity Cancer. J Clin Oncol. 2017; 35(31):3601-3609.
6. Sinha P, Kallogjeri D, Gay H, et al. High metastatic node number, not extracapsular spread or N-classification is a node-related prognosticator in transorally-resected, neck-dissected p16-positive oropharynx cancer. Oral Oncol 2015; 51(5):514-20.
Figures