3665
Hypovascular nodules detected on gadoxetic acid-enhanced MR imaging: Risk factors and appropriate treatments for hypervascular transformation1Department of Radiology, National Cancer Center/National Clinical Research Center for Cancer/ Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China., Beijing, China, 2Department of Radiology, National Cancer Center/National Clinical Research Center for Cancer/ Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, Beijing, China, 3GE Healthcare, MR Research China, Beijing, China, Beijing, China
Synopsis
Hypovascular hypointense nodules detected in the hepatobiliary phase (HBP) of gadoxetic acid-enhanced MRI have significant potential to transform into hypervascular hepatocellular carcinoma (HCC). This study aims to assess the risk factors for hypervascular transformation and to enable guiding the clinical treatment properly.
Purpose
To investigate clinical and imaging features of hypovascular hypointense nodules on hepatobiliary phase gadoxetic acid-enhanced MR images in patients with cirrhosis which may predict hypervascularization during follow-up and further guide the appropriate treatment.Introduction
Gadoxetic acid could increase the detection of borderline hepatic nodules with hypovascularity in the arterial phase and hypointensity at the hepatobiliary phase (HBP) for patients with chronic liver disease [1]. Borderline hepatic nodules are at the adjacent stage in the process of hepatocarcinogenesis and in the high risk of hypervascularization and thereby, it is important for these nodules to be early detected and appropriate managed [2].Material and Methods
This study enrolled 77 patients with liver cirrhosis and 224 hypovascular hypointense nodules detected at the hepatobiliary phase of gadoxetic acid-enhanced MR imaging. The effect of baseline clinical features, MR features and growth rate on subsequent hypervascularization were retrospectively evaluated. Moreover, the impact of different modalities of treatments of the hypervascularization of hypovascular hypointense nodules on the subsequent HCC recurrence were investigated.Results
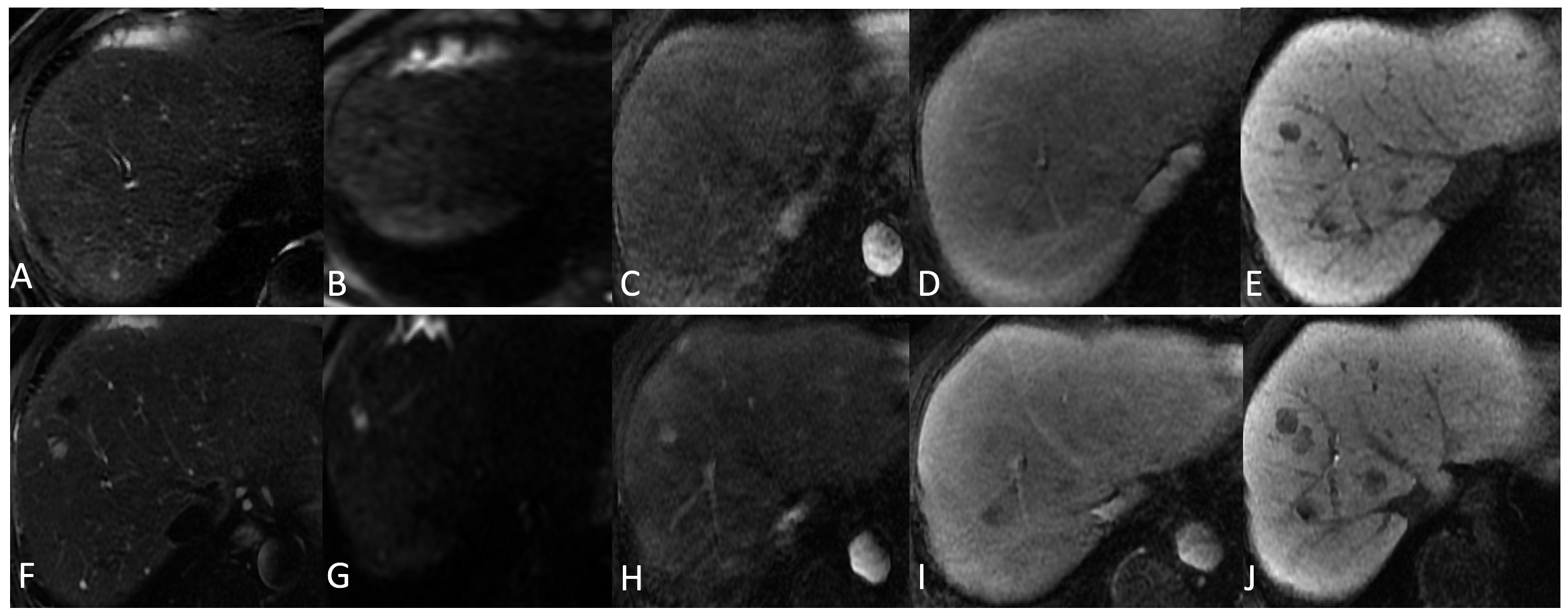
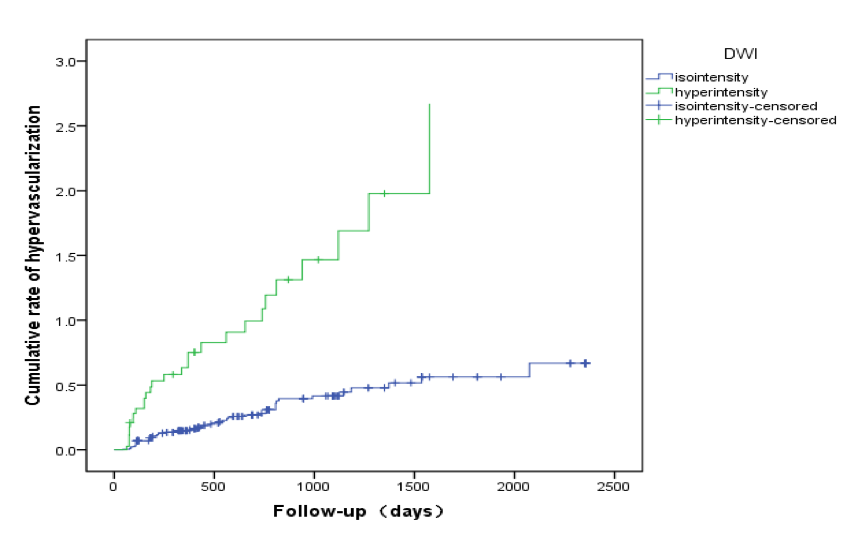
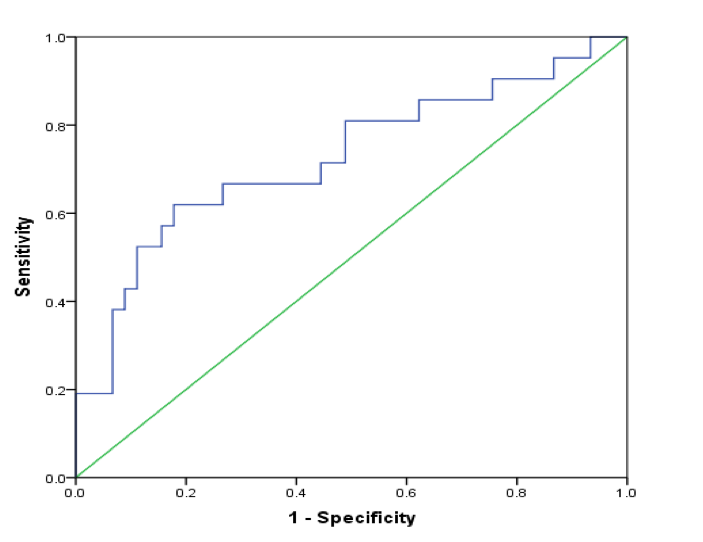
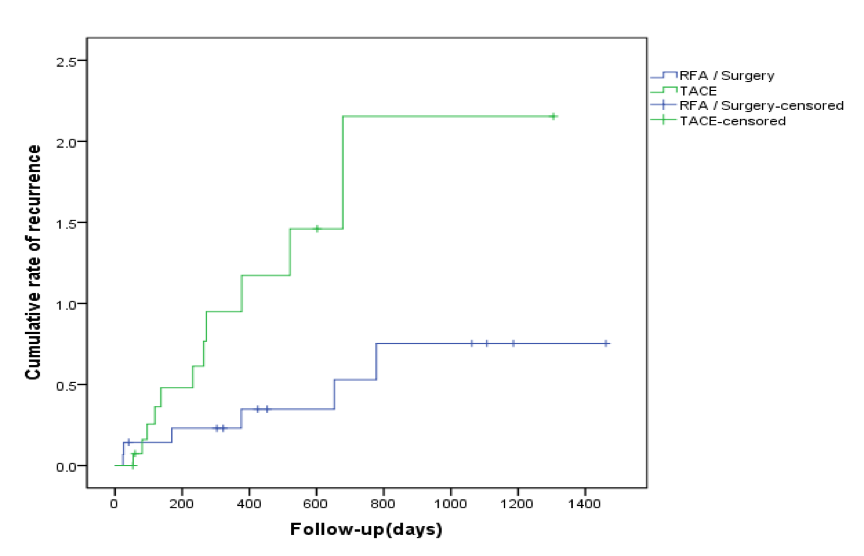
On follow-up contrast-enhanced MR or CT images, 160 nodules (65.5%) did not transform into hyervascularization (mean follow-up, 763 days), while 84 (34.4%) became hypervascular HCC (mean follow-up, 463 days) (Figure 1), with a cumulative rate of hypervascularization of 18.9%, 30.0%, 41.8% and 62.1% at 1, 2, 3, and 6 years respectively. Multivariable Cox analysis revealed that the hyperintensity on DW images (hazard ratio, 0.346; 95% CI: 0.183,0.655; P=0.001) and the most hypointensity (equal to or lower than that of the intrahepatic portal vein) on HBP images (hazard ratio, 0.291; 95% CI: 0.106,0.797; P=0.016) were significantly related to the development of hypervascularization (Table 1). Comparison of the rates of hypervascularization of hypovascular hypointense nodules between those with or without hyperintensity based on DW images indicates that the two subgroups was statistically significant (P=0.000) (Figure 2). The optimal growth rate cutoff point on the ROC curve was 2.92×10-3/days (Figure 3). The cumulative recurrence rate of transcatheter intra-arterial chemoembolization (TACE) for hypervascularization of hypovascular hypointense nodules was higher compared with the patients who performed radiofrequency ablation (RFA) or surgery (p=0.035) (Figure 4).Discussion and Conclusion
It is difficult to identify the exact stage of hepatocellular nodules in the gray area of hepatocarcinogenesis. During the process, OATP8 expression level decreases prior to complete neoangiogenesis. As a result, most borderline hepatic nodules present as iso- or hypovascularity, hypointensity in the hepatobiliary phase. Borderline hepatic nodules are at the high risk of hypervascularization during follow-up. So understanding of the fate and clinical implications of hypovascular hypointense nodules is important in guiding a proper management. Our study shows those nodules with an increased growth rate, and hyperintensity on initial DW images and the most hypointensity on HBP images in patients with cirrhosis can perform as predictive factors. The results correspond to several previous studies [3, 4]. To our best knowledge, previous studies did not mention whether additional survival benefits can be expected from the different options of the hypervascularization from the previous high risk nodules.In this study, the cumulative recurrence rate of TACE for the hypervascularization of hypovascular hypointense nodules was higher compared with patients who received RFA or surgery. It indicates that patients who performed with RFA or surgery for vascularization of the high risk nodules will get more survival benefits than patients who performed with TACE.
In conclusion, hypovascular hypointense nodules with an increased growth rate, and hyperintensity on initial DW images and the most hypointensity on HBP images in patients with cirrhosis as predictive factors and those nodules could be treated with RFA or surgery for improving survival expectancy and quality.
Acknowledgements
This study was supported by the National Natural Science Foundation of China (81671677).References
[1] Park H J, Choi B I, Lee E S, et al. How to differentiate borderline hepatic nodules in hepatocarcinogenesis: Emphasis on imaging diagnosis [J]. Liver Cancer, 2017, 6(3): 189-203.
[2] Suh C H, Kim K W, Pyo J, et al. Hypervascular transformation of hypovascular hypointense nodules in the hepatobiliary phase of Gadoxetic acid-enhanced MRI: A systematic review and meta-analysis[J]. American Journal of Roentgenology, 2017, 209(4): 781-789.
[3] Yang H J, Song J S, Choi E J, et al. Hypovascular hypointense nodules in hepatobiliary phase without T2 hyperintensity: Long-term outcomes and added value of DWI in predicting hypervascular transformation[J]. Clinical Imaging, 2018, 50: 123-129.
[4] Takara K, Saito K, Saguchi T, et al. Is diffusion-weighted imaging a significant indicator of the development of vascularization in hypovascular hepatocellular lesions?[J]. Clinical Imaging, 2014, 38(4): 458-463.
Figures