3664
Single-breath-hold whole-heart-coverage accelerated 3D-cine cardiac MRI1Medical College of Wisconsin, Milwaukee, WI, United States
Synopsis
Conventional cine imaging consumes a large part of scan time due to the need to acquire a stack of short-axis and long-axis slices. In this study, we provide preliminary results about the feasibility of a single-breath-hold whole-heart-coverage accelerated 3D-cine acquisition in a fraction of this time using recent developments in acquisition and reconstruction techniques. The results shows significantly reduction of scan time by more than 90%. Despite encountered reduction in resolutions, SNR and CNR, sufficient image quality was maintained such that the resulting clinical measurements were not significantly different from those obtained using conventional cine acquisition.
INTRODUCTION
Cine imaging is an essential part of almost every cardiac MRI exam, which is used to evaluate heart function based on basic cardiovascular parameters such as ejection fraction (EF), myocardial mass, and wall thickening [1]. Nevertheless, conventional cine imaging requires long scan time due to the need to acquire a stack of short-axis slices (typically 12-16 slices) that covers the whole heart, in addition to other long-axis slices. As cine slices are typically acquired one slice per breath-hold, acquiring all cine images in this conventional fashion consumes a considerable amount of scan time. In this study, we provide preliminary results about the feasibility of whole-heart-coverage 3D-cine imaging in a fraction (10-20%) of this time using recent developments in acquisition and reconstruction techniques, and evaluate the effects of different imaging strategies on image quality and resulting clinical measurements.METHODS
An advanced 3D cine imaging technique is implemented, which includes a number of acquisition and reconstruction developments, including variable-density k-t sampling [2], kat ARC (Autocalibrating Reconstruction for Cartesian sampling with K- & Adaptive-T-space data synthesis; a spatiotemporal correlation-based auto-calibrating parallel imaging method) [3], and static tissue removal to reduce residual artifacts from chest wall signal before kat ARC unaliasing [4]. The technique allows for achieving an acceleration factor of 9 and whole-heart imaging in a single breath-hold.
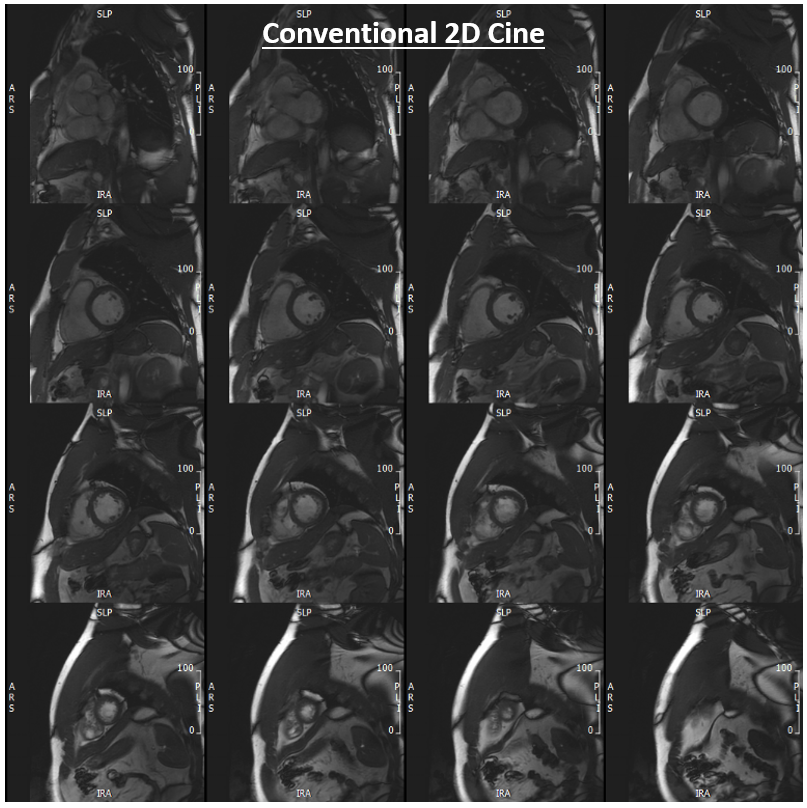
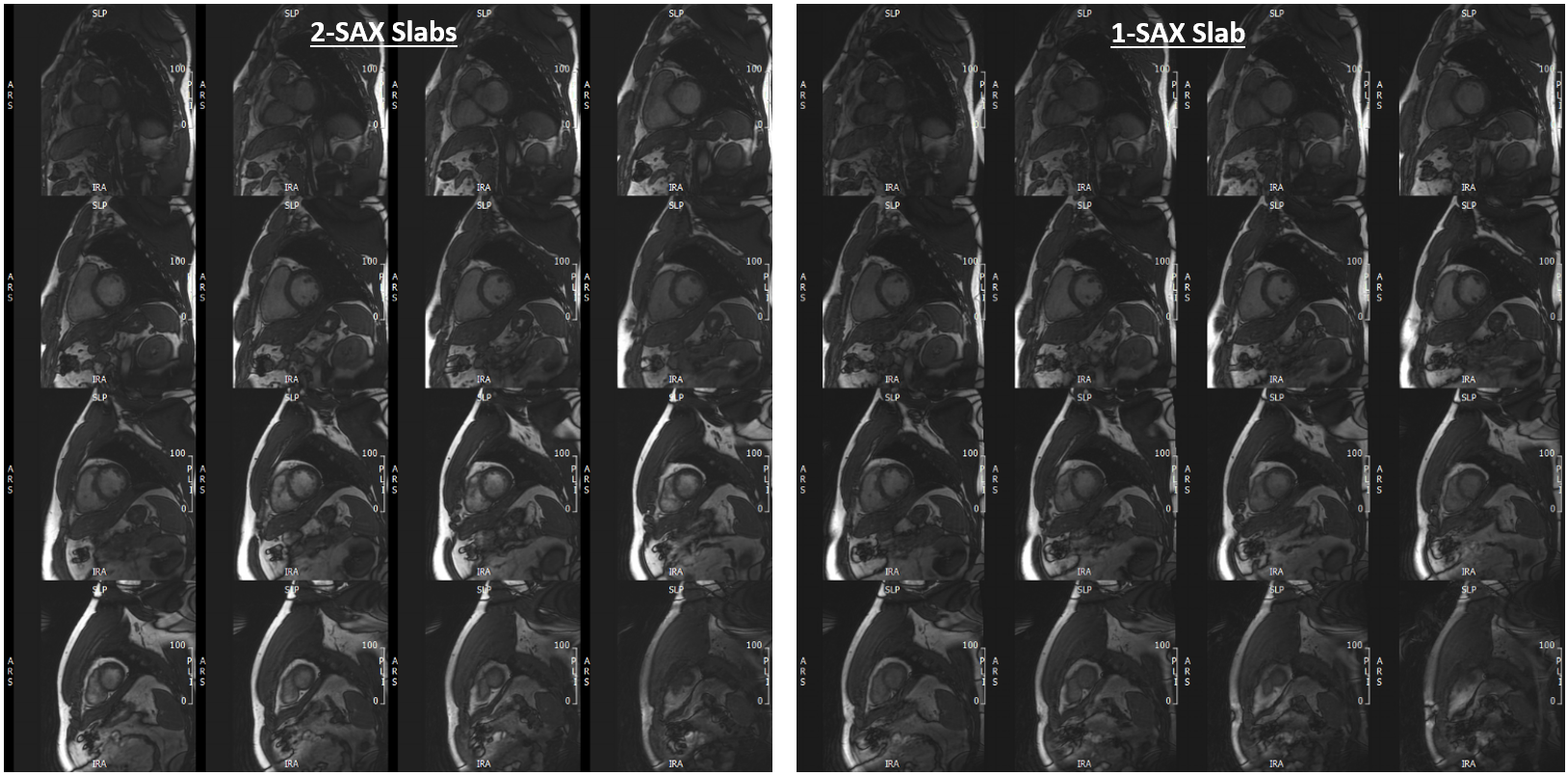
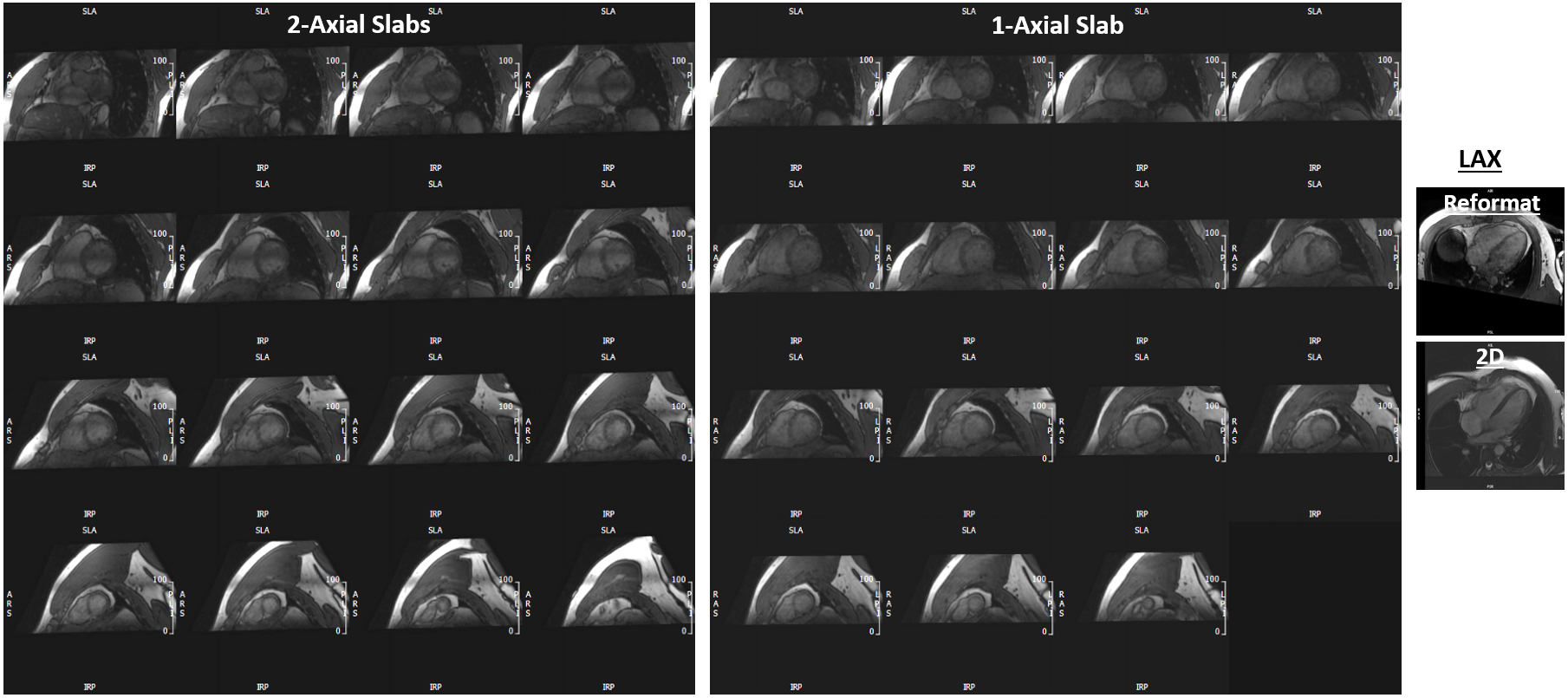
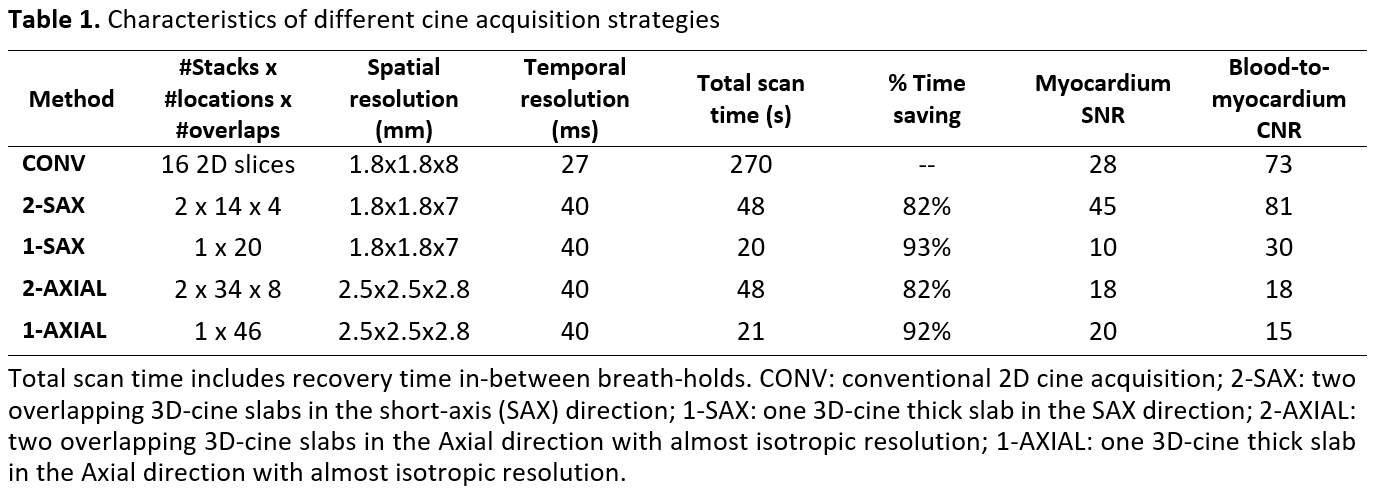
Two healthy subjects were scanned on a GE 3T Premier scanner using the following whole-heart-coverage acquisition scenarios (Table-1): 1) CONV: conventional 2D cine acquisition with short-axis slices acquired in separate breath-holds; 2) 2-SAX: two overlapping 3D-cine slabs acquired in the short-axis direction in two breath-holds; 3) 1-SAX: one 3D-cine thick slab acquired in the short-axis direction in a single breath-hold; 4) 2-AXIAL: two overlapping 3D-cine slabs acquired in the axial direction (with almost isotropic resolution) in two breath-holds; and 5) 1-AXIAL: one 3D-cine thick slab acquired in the axial direction (with almost isotropic resolution) in a single breath-hold.
Myocardium signal-to-noise ratio (SNR) was measured as the ratio between mean myocardial signal intensity and background standard deviation (SD). Blood-to-myocardium contrast-to-noise ratio (CNR) were measured as the ratio between the mean blood-to-myocardial signal intensity difference and background SD.
The images were processed using Circle cvi42 software. The AXIAL datasets were reformatted to generate a stack of short-axis and long-axis images. The short-axis and long-axis images from different acquisition scenarios were semi-automatically processed to measure EF, myocardial mass, and wall thickness of different heart segments based on the AHA 17-segment model. Statistical t-test was conducted to measure significance in measurements differences (p<.001 considered significant).
RESULTS
Figures 1-3 show results from the CONV, SAX, and AXIAL acquisitions, which show good agreement between short-axis images obtained in the same subject using different acquisition strategies. Table-1 summarizes scan time, SNR, and CNR results of different acquisitions.
The 2-SAX, 1-SAX, 2-AXIAL, and 1-AXIAL acquisitions resulted in 82%, 93%, 82%, and 92% savings in scan time, respectively, compared to CONV acquisition. SNR(CNR) increased for the 2-SAX acquisition, compared to CONV acquisition, by 86(24)%, while it decreased by 37.5(26.5)%, 49.5(78)%, and 29(77.9)% for the 1-SAX, 2-AXIAL, and 1-AXIAL acquisitions.
CONV acquisition resulted in EF(mass) of 60%(129g) and 61%(125g) for the first and second subjects, respectively. Average differences in EF(mass), compared to CONV acquisition, were -8%(5g), -4%(2g), -7%(3g), and -7%(1g) for the 2-SAX, 1-SAX, 2-AXIAL, and 1-AXIAL acquisitions, respectively. Average end-diastolic (end-systolic) percentage differences in segmental wall thickness, compared to CONV acquisition, were 1.6%, -0.7%, -5.3%, and 6.4% (-7.9%, 4.1%, -1.1%, and -8.9%) for the 2-SAX, 1-SAX, 2-AXIAL, and 1-AXIAL acquisitions, respectively, where all measurement differences were statistically insignificant.
DISCUSSION and CONCLUSION
Despite the limited number of studied subjects, preliminary results from this study show the capability of advanced accelerated 3D cine imaging with the proposed acquisition strategies of significantly reducing scan time by more than 90%.
Despite encountered reduction in spatial/temporal resolutions, SNR and CNR, sufficient image quality was maintained such that the resulting clinical measurements were not significantly different from those obtained using the conventional lengthy cine acquisition.
The proposed single-breath-hold acquisition would add to the patient’s comfort and avoid slice misregistration errors. Nevertheless, in patients with limited breath-holding capability, the single breath-hold can be split in 2 shorter breath-holds. AXIAL acquisitions save more time as no additional long-axis imaging is required and no experience is needed to prescribe certain slice positions.
In conclusion, the proposed techniques in this study have the potential to make cardiac MRI more cost effective and widely adopted in clinical practice.
Acknowledgements
No acknowledgement found.References
1. Kramer et al. JCMR 2013
2. Lai et al. ISMRM 2015
3. Lai et al. ISMRM 2009
4. Lai et al. ISMRM 2014
Figures