3661
Clinical Implementation of Fast Markerless Motion Correction in K-Space of Structural 3D MR-Images of the Brain1DTU Compute, Technical University of Denmark, Lyngby, Denmark, 2Tracinnovations, Ballerup, Denmark, 3Department of Clinical Physiology, Nuclear Medicine & PET, Rigshospitalet, Copenhagen, Denmark, 4CUBRIC School of Engineering, Cardiff University, Cardiff, United Kingdom
Synopsis
This work demonstrates retrospective motion correction using a markerless motion tracker to accommodate the needs in the clinical workflow. Motion degradation in neurological MRI imaging is a major concern and causes increased study time and cost due to repeated scans and the need for sedation or anesthesia. With retrospective motion correction of raw k-space data, both the corrected and non-corrected images can be reconstructed and presented for the radiologists within a few minutes. The external markerless motion tracker is sequence independent meaning that retrospective motion correction can be applied to clinical examination without sequence modification or added scan time.
Introduction
In medical brain MRI, corruption of image quality due to head motion is an ongoing concern, where sedation or anesthesia is often the only means for clinical pediatric studies, leading to increased patient risk, study time, and cost. While prospective Motion Correction (MoCo) offers real-time correction, it does not preserve the original (uncorrected) data and is therefore considered a more intrusive method, which may not be ready for clinical implementation1, 2. Retrospective MoCo is performed retrospectively to the data acquisition, making it non-destructive to the original images and is therefore more suitable for direct clinical implementation. Retrospective k-space correction has previously been demonstrated using motion information acquired using MRI-based navigators3, 4. Though MRI-based navigators are integrated in the scan sequence, they are not sequence independent and may increase total scan time. Additionally, external tracking systems are typically able to offer a much higher temporal resolution than navigator-based methods. An external markerless motion tracker has previously been used to demonstrate retrospective image space correction of an EPI timeseries5, but to our knowledge it has not previously been demonstrated for retrospective k-space correction of 3D structural scans. In this work, we demonstrate the combination of retrospective k-space correction using motion data recorded with an external markerless motion tracker to demonstrate its potential for clinical use. The markerless approach fits the clinical workflow well, as it requires no patient interaction and there are no tracking uncertainties due to marker dislocation.Methods
The markerless head motion tracking system “Tracoline” TCL 3.1 (TracInnovations)6,7 was set up on a Siemens mMR Biograph 3T scanner to give precise head motion estimates of a healthy volunteer who has given written informed consent for participation. Two 3D-MPRAGE scans of the volunteer’s head were acquired with a 16-channel head-coil using the scanner settings: TR=1900ms, TE=2.44ms, FOV=192x256x256mm, voxel size=0.48x0.48x1.00mm, GRAPPA acceleration factor=2. During the two 302 seconds scans, the volunteer was instructed to perform two different motion patterns: slow continuous head rotation, and fast stepwise rotation. Prior to MoCo, the motion estimates recorded with TCL were geometrically and temporally aligned to the scanner by matching a reference point cloud to the surface of the MPRAGE scan8 and by a network time synchronization. Retrospective correction was implemented using a freely available software package (RetroMoCoBox9) within MATLAB (The MathWorks, USA). Each line of raw k-space data was temporally matched to the nearest motion-estimate available from the TCL system (30 estimates per second). Rigid-body correction was applied by additional phase-ramps to account for translations and using a non-uniform FFT implementation (from the MIRT toolbox10) to account for rotations. This correction was applied separately for each of the 16 RF channels – after the GRAPPA parallel imaging reconstruction and before coil combination. To allow MoCo of skipped k-space lines the motion parameters were linearly interpolated to generate ‘pseudo’ motion-estimates, which allow preservation of k-space geometry.Results
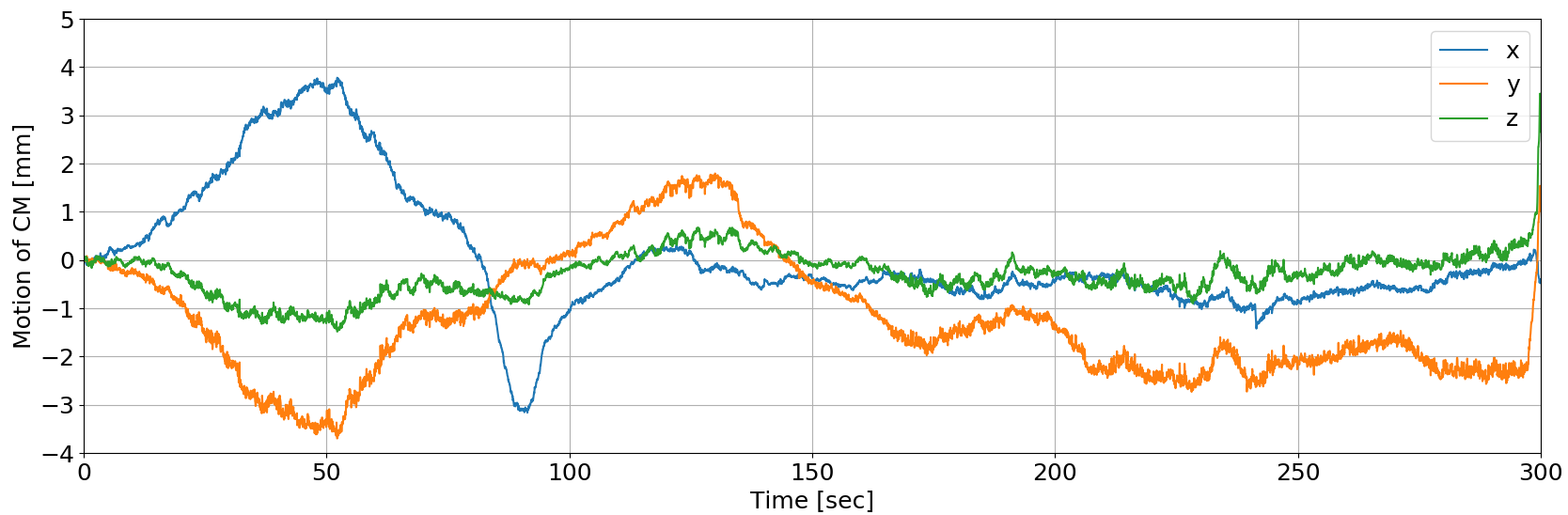
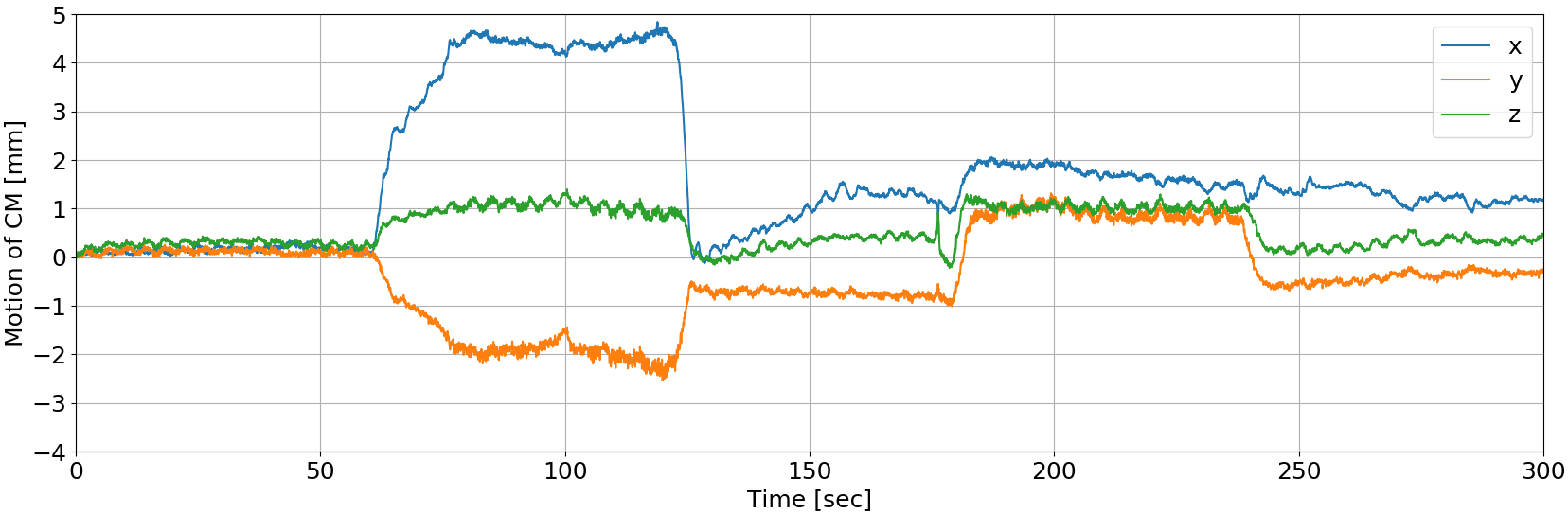
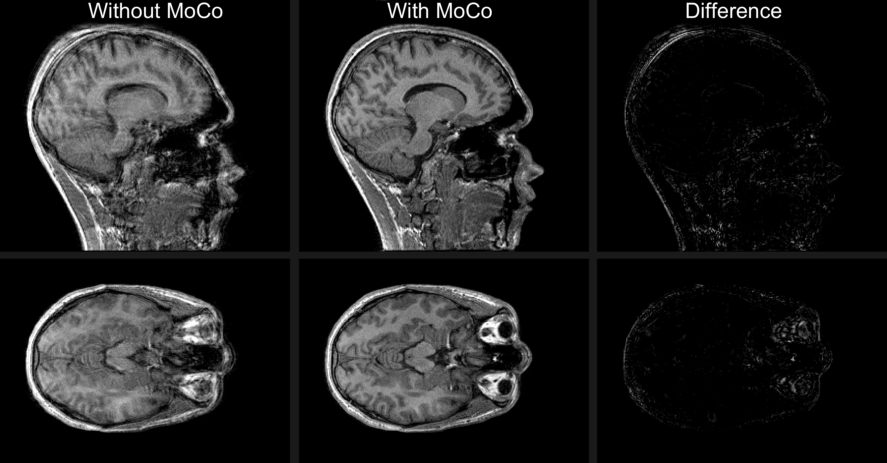
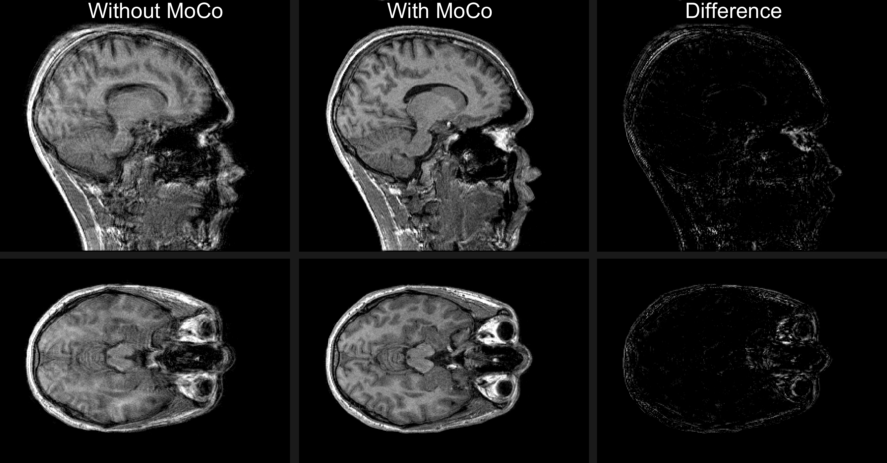
Figure 1 and 2 show the estimated head motion when the volunteer was performing slow continuous head rotation and fast stepwise rotation, respectively. Image reconstruction from the raw data with correction takes 2 minutes on a desktop PC with an Intel® Core™ i7-8700K running at 5GHz with 16GB RAM. The resulting images are shown in Figure 3 and 4, where the left and middle slices are reconstructed without and with MoCo, respectively. The images to the right show the difference between the original and corrected images.Discussion
As demonstrated in Figure 3 and 4, retrospective MoCo improves image quality based on motion inputs from the external markerless motion tracker. The ghosting artifacts are reduced in the corrected image for both cases and we see an improvement in contrast between gray and white matter. Using the external markerless motion tracker makes it possible to implement retrospective MoCo in the clinic without changing the existing protocols. The low reconstruction time of 2 minutes allows the radiologist to be presented with the motion corrected image in the scan session. Thus, the combination of the proposed retrospective MoCo pipeline and the external motion tracker makes clinical implementation possible. Improving the image quality using MoCo may also allow a reduced use of sedation and allow groups of patients that would otherwise not be feasible for an MRI exam.Conclusion
Fast retrospective MoCo in the k-space domain using an external markerless motion tracker significantly improved the quality of the structural 3D MR-images. The MoCo procedure was implemented on a clinical scanner without changing any existing pulse sequences or acquisition protocols.Acknowledgements
The authors would like to thank the Department of Clinical Physiology, Nuclear Medicine and PET, Rigshospitalet, University of Copenhagen, Denmark for general support and availability of clinical scanner facilities. They would also like to thank the John and Birthe Meyer Foundation for the generous donation of the mMR Biograph hybrid 3T PET/MRI scanner.References
[1] Maclaren et al. MRM, 69:621-636, 2013
[2] Frost et al. ISMRM 2018, p1167
[3] Gallichan et al. MRM 75(3):1030-1039, 2016
[4] Federau et al. PLOS ONE, 2016
[5] Jensen et al. ISMRM 2015
[6] Olesen et al. IEEE Trans. Med. 31(1), 2012
[7] Olesen et al. ISMRM 2014, p1303
[8] Benjaminsen et al. ISMRM 2016, p1860
[9] RetroMoCoBox Toolbox, https://github.com/dgallichan/retroMoCoBox
[10] MIRT Toolbox, https://web.eecs.umich.edu/~fessler/code/
Figures