3658
A New Nodal Staging System for Nasopharyngeal Carcinoma Based on the Quantitation of Metastatic Lymph Nodes1radiology, Sun Yat-sen University Cancer Center, Guangzhou, China
Synopsis
We aimed to investigate whether the number of metastatic lymph nodes (LNs) is an independent prognostic factor for progression-free survival (PFS) in nasopharyngeal carcinoma (NPC) and to establish a new N staging system based on the number of positive LNs on magnetic resonance imaging. In 792 NPC patients, we found that the number of metastatic LNs was the only independent prognostic factor for PFS following multivariate analysis. We categorized the number of metastatic LNs into 4 groups to create a new N staging system which was more effective than the American Joint Committee on Cancer staging system for predicting PFS.
INTRODUCTION
The American Joint Committee on Cancer (AJCC) N staging system for NPC is defined according to the size, laterality, and location of metastatic lymph nodes (LNs) and may underestimate the cumulative effect of the metastatic nodal burden. This study examined whether the number of metastatic lymph nodes (LNs) is an independent prognostic factor for progression-free survival (PFS) in nasopharyngeal carcinoma (NPC) patients and established a new N staging system using the number of positive LNs on magnetic resonance imaging (MRI).METHODS
Patients with newly diagnosed, biopsy-proven, and non-metastatic NPC were enrolled. Number, size, laterality, and location of the metastatic LNs were assessed on MRI. Univariable and multivariable Cox regression models were constructed to assess the association between the number of metastatic LNs and PFS. Restricted cubic spline was used to determine the cutoff values of the number of LNs used for defining N stages. Kaplan-Meier methods with log-rank tests were used to compare PFS across our newly established N-stages and AJCC N stages. The predictive ability of the newly established N stages and AJCC N stages was determined and compared using a concordance index (c-index).RESULTS
Seven hundred and ninety-two patients comprised the training cohort and 433 patients comprised the validation cohort. In the training cohort, the number of metastatic LNs, laterality, and location were independent risk factors for disease progression after adjusting for age, T-stage, and chemotherapy (Table 1, model 1). However, after adding the number of metastatic LNs into the multivariable Cox regression model, the number of metastatic LNs was the only independent prognostic factor for PFS (P<0.001, Table 1, model 2 ). The number of MRI-positive LNs was subdivided into 4 groups (0, 1-2, 3-6, >6) to establish the new N staging system. The c-index of our new N staging system (0.659, 95% CI=0.656–0.662) for predicting PFS was higher than the AJCC N staging system (0.650, 95% CI=0.647–0.653, P<0.001).DISCUSSION
Consistent with findings of previous studies1-3, the location of metastatic LNs and laterality of cervical metastatic LNs were independent prognostic factors for disease progression in this study. However, after including the number of metastatic LNs in the multivariate analysis, neither were associated with PFS, indicating that the number of LNs is a proxy of these 2 variables. Our finding that the number of metastatic LN was strongly correlated with nodal location and laterality also suggested that the number of positive nodes was a better proxy of nodal location and laterality. We did not find that the size of LNs was an independent prognostic factor for disease failure in NPC patients. Similar to findings for oropharyngeal, hypopharyngeal, and laryngeal cancers 4-6, the number of metastatic LNs was a critical prognostic factor for NPC. We proposed a new nodal staging schema based the number of metastatic LNs. Compared with the AJCC 8th version of the N staging system, our new nodal staging system achieved better concordance between the predicted and observed progression of disease, although the absolute difference in c-indices was relatively modest. Since our new N staging system is only based on the number of metastatic LNs to define N stages, it is more concise and user friendly than the AJCC staging system, which used 3 variables (size, laterality, and location) to classify N stages.CONCLUSION
The number of metastatic LNs was an independent prognostic factor for NPC patients’ long-term survival. Our N staging system was concise and achieved better predictive ability than the AJCC system. It may inform more tailored treatment for NPC patients and is thus of great clinical potential.Acknowledgements
We thank the patients who participated in this study. We also thank all of the doctors in the Sun Yat-sen University Cancer Center for their contribution.References
1. Li WF, Sun Y, Mao YP, et al. Proposed lymph node staging system using the International Consensus Guidelines for lymph node levels is predictive for nasopharyngeal carcinoma patients from endemic areas treated with intensity modulated radiation therapy. Int J Radiat Oncol Biol Phys 2013;86(2):249-56.
2. Mao YP, Liang SB, Liu LZ, et al. The N staging system in nasopharyngeal carcinoma with radiation therapy oncology group guidelines for lymph node levels based on magnetic resonance imaging. Clin Cancer Res 2008;14(22):7497-503.
3. Heng DM, Wee J, Fong KW, et al. Prognostic factors in 677 patients in Singapore with nondisseminated nasopharyngeal carcinoma. Cancer 1999;86(10):1912-20.
4. Ho AS, Kim S, Tighiouart M, et al. Metastatic Lymph Node Burden and Survival in Oral Cavity Cancer. J Clin Oncol 2017;35(31):3601-3609.
5. Ho AS, Kim S, Tighiouart M, et al. Association of Quantitative Metastatic Lymph Node Burden With Survival in Hypopharyngeal and Laryngeal Cancer; 2017.
6. Sinha P, Kallogjeri D, Gay H, et al. High metastatic node number, not extracapsular spread or N-classification is a node-related prognosticator in transorally-resected, neck-dissected p16-positive oropharynx cancer. Oral Oncol 2015;51(5):514-20.
Figures
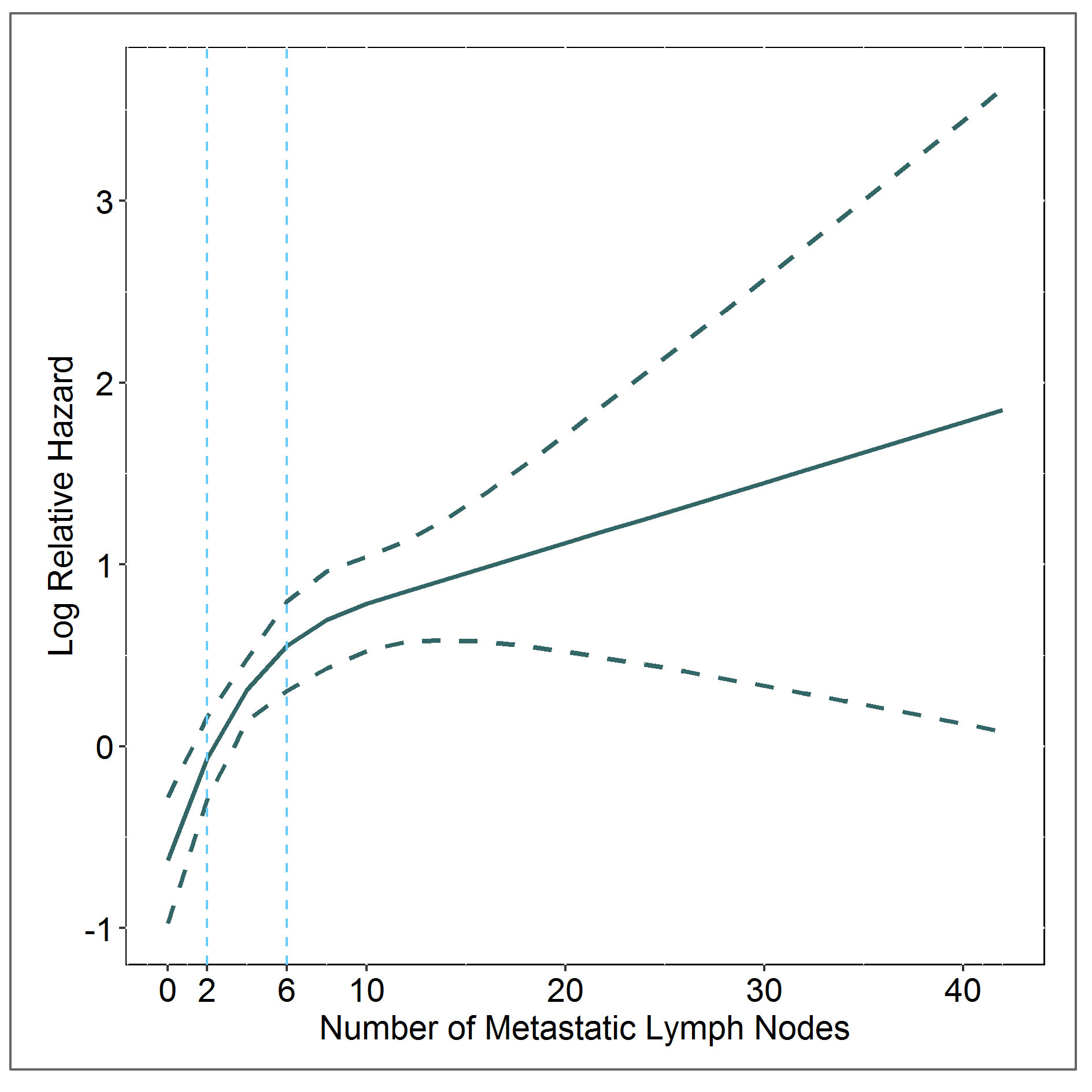
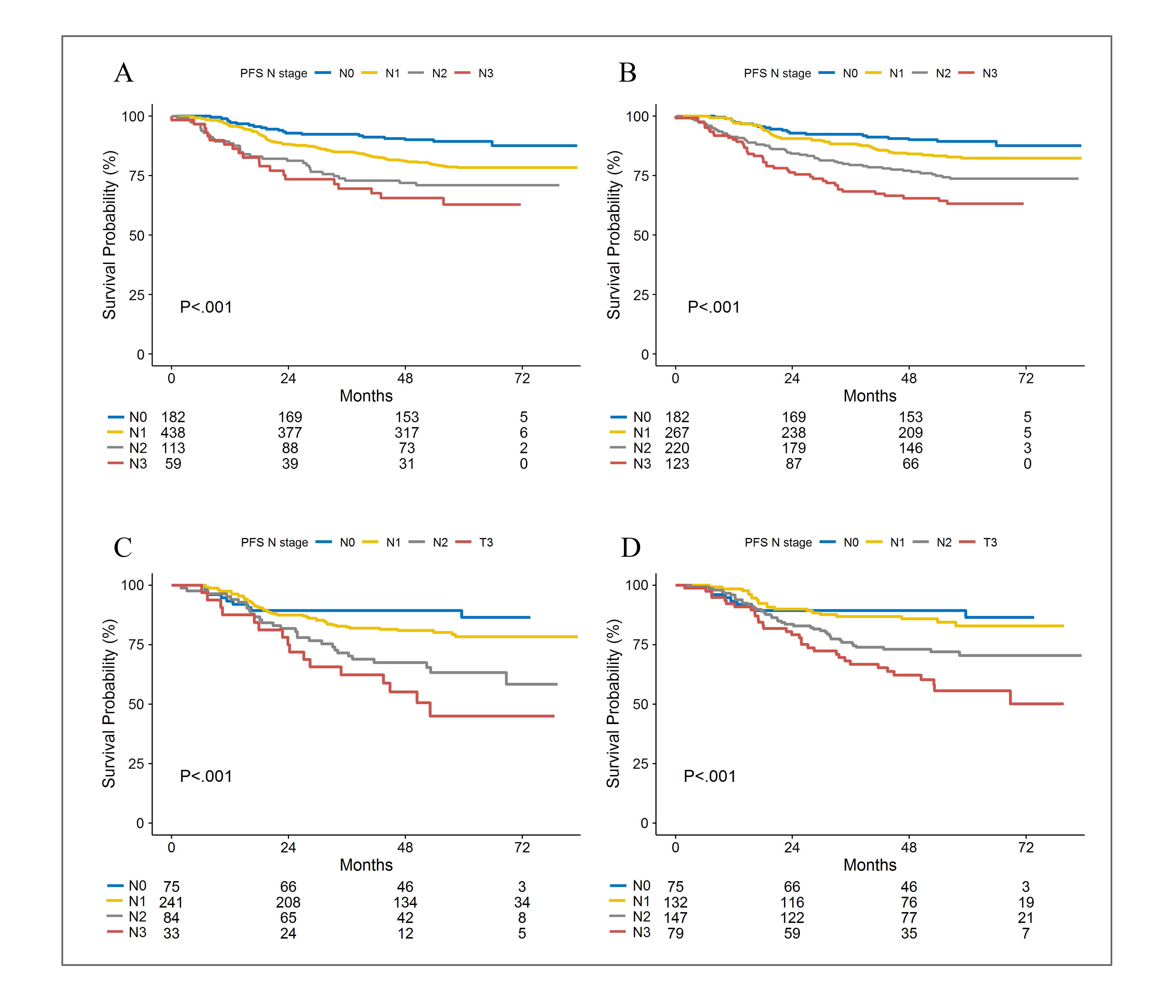
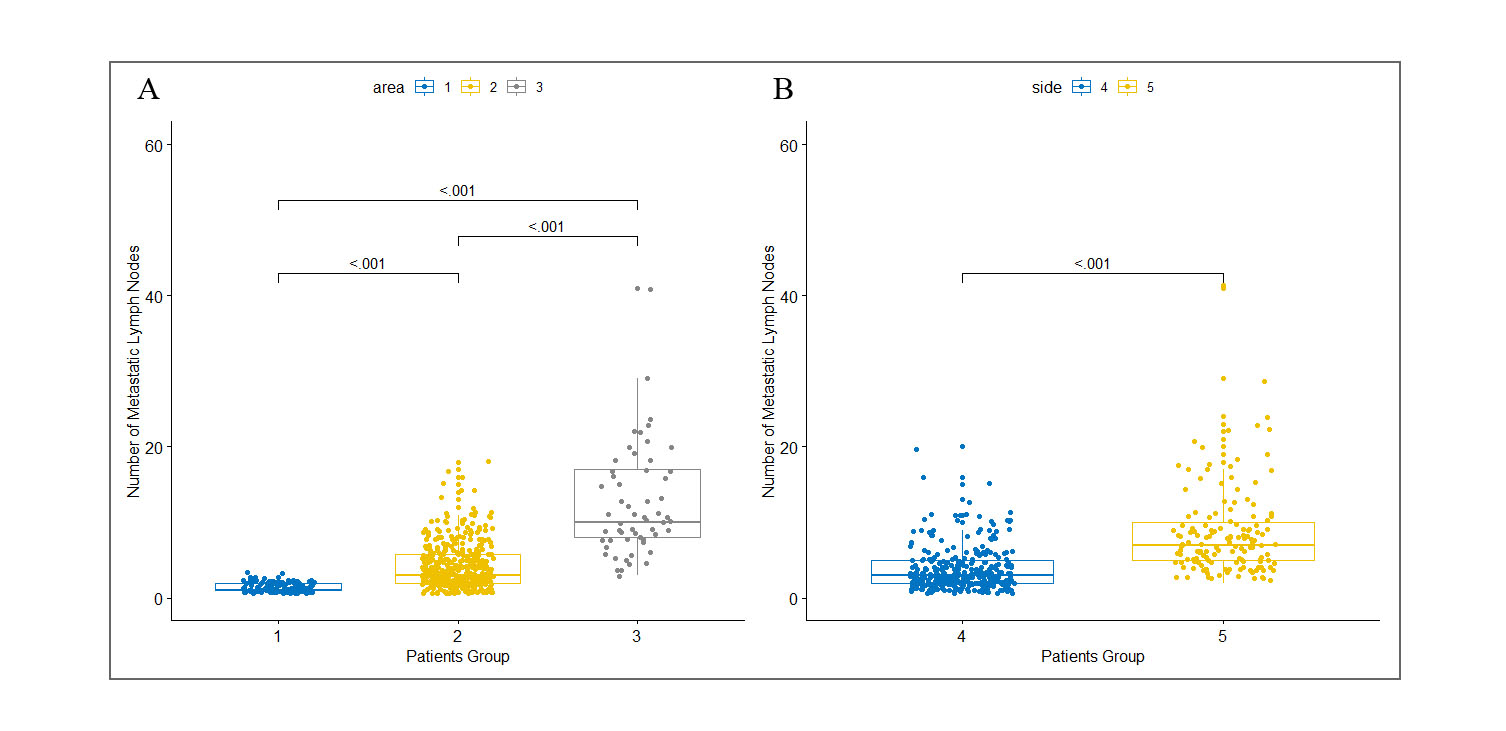
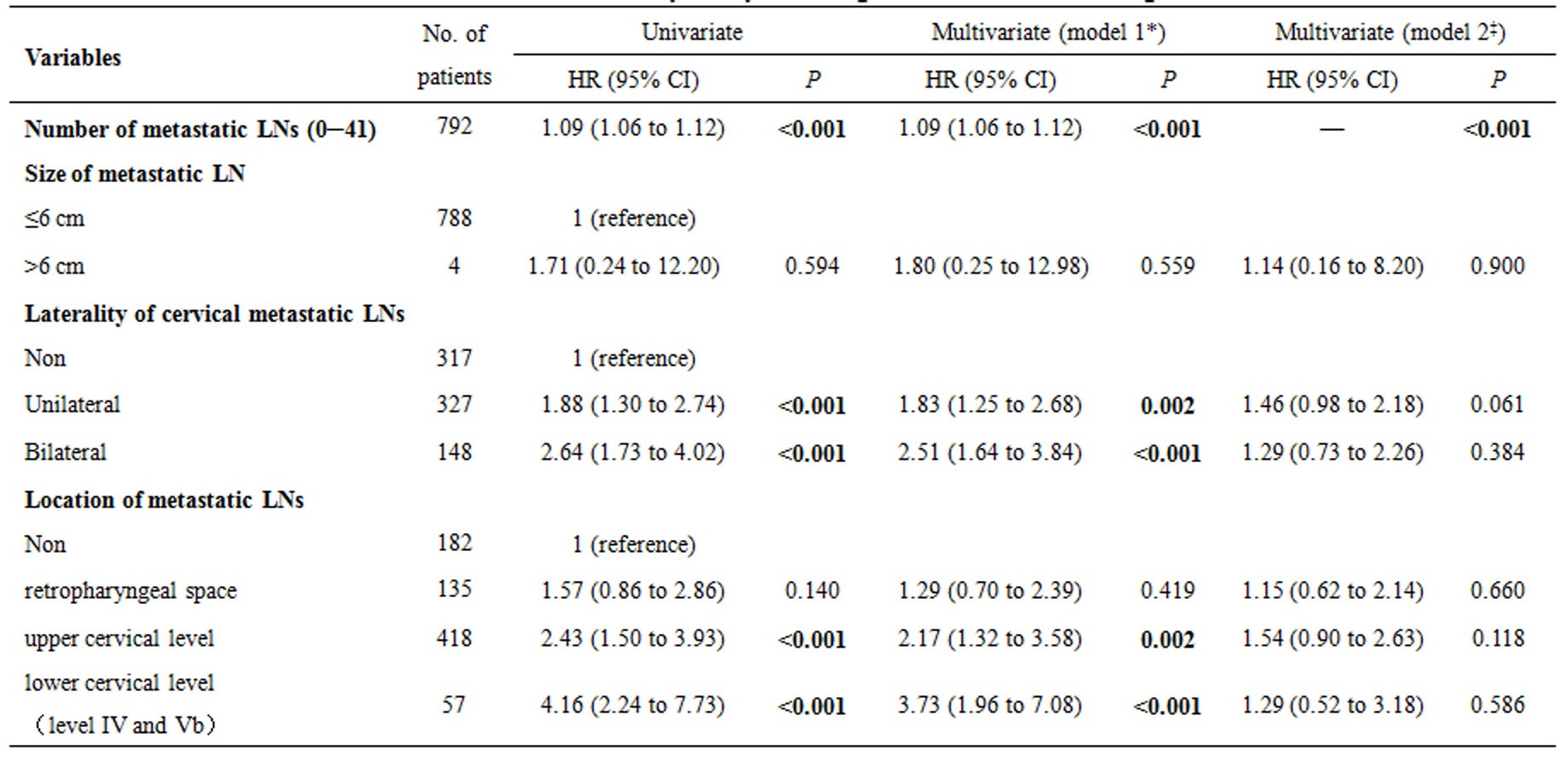
Table 1. Multivariate survival analysis by Cox regression in the training cohort
Abbreviations: LN, lymph node. HR, hazard ratio.
*Multivariable models were adjusted for age, American Joint Committee on Cancer T classification and chemotherapy.
‡Multivariable models were adjusted for age, American Joint Committee on Cancer T classification, chemotherapy and the number of metastatic LNs.