3657
Value of patent foramen ovale in grey matter and white matter lesions of migraine: A comparative study1Department of Diagnostic Radiology, First Affiliated Hospital of Xi’an Jiaotong University, xi'an, China, 2Department of Neurology, First Affiliated Hospital of Xi’an Jiaotong University, xi'an, China
Synopsis
Migraine is a complicated neurological disability disease and still not been clarified. PFO may be a subset to cause migraine. Therefore, this study aims to analysis the value of PFO in grey matter and white matter lesions of migraine. We found that the changes mainly in frontal cortex, precentral gyrus regions of pain modulating area between patients with PFO and without PFO in migraine. However, out results do not support the relationship between PFO and white matter lesions. This findings may provide a new insight for clinical treat strategy.
Introduction
Migraine is one of the most disabling neurovascular disorders, characterized by attacks of severe headaches and autonomic nervous system dysfunction. Recent magnetic resonance imaging (MRI) data suggest that grey matter (GM) and white matter lesions (WMLs) changes are detected in migraine, but the mechanism has not been elucidated. A casual relationship has been hypothesized between patent foramen ovale (PFO) and migraine. The right-to-left shunts from PFO may increase risks to migraine [1, 2]. However, it has not been clarified whether PFO increases the risk of developing GM and white matter lesions (WMLs) in migraine patients. Therefore, we used voxel-based morphometry (VBM) to analysis the GM changes in migraine patients with or without PFO and used white matter rating scale to analysis WMLs changes, so as to evaluate the value of PFO in migraine.Methods
The Institutional Review Board approved this study and all the written informed consents were obtained from migraine patients. Patients 18 migraine patients with PFO, 18 migraine patients without PFO on MRI were included. All were undergone a PFO detection with air-contrast transcranial Doppler (cTCD). The grade of PFO:Ⅰ,no microbubble signals (MBs); Ⅱ,1-10MBs;Ⅲ, more than 10MBs, but no rain curtain; Ⅳ, rain curtain. MR Protocols. All MR examinations were performed using a 3T scanner (GE, Signa HDxt) with an 8-channel head coil. The protocols included sequences: a transverse 3D T1-weighted sequence (TR/TE, 8ms/2.5ms; matrix, 220×220; section-thickness, 1mm; FOV, 220mm; time, 6min14s) and fluid attenuated inversion recovery sequence (Flair) (TR/TE, 8600ms/132.4ms; TI, 2319ms; matrix, 256×256; section-thickness, 1mm; FOV, 220mm; time,9min05s); Data and statistical analysis 3D-T1 data was processed with the aid of the FMRIB software library (FSL, www.fmrib.ox.au.uk/fsl) and flair data was analyzed with Scheltens scale score [3]. All statistical analysis were performed by using SPSS17.0 (SPSS, Chicago, IL, USA); p < 0.05 was considered as statistically significant difference.Results
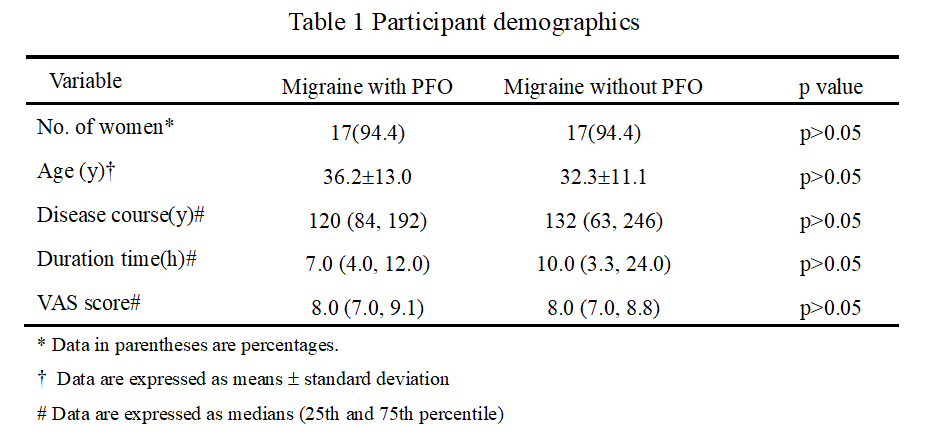
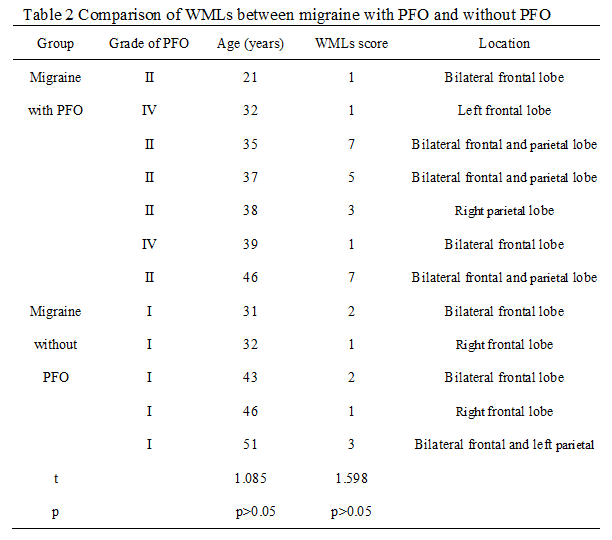
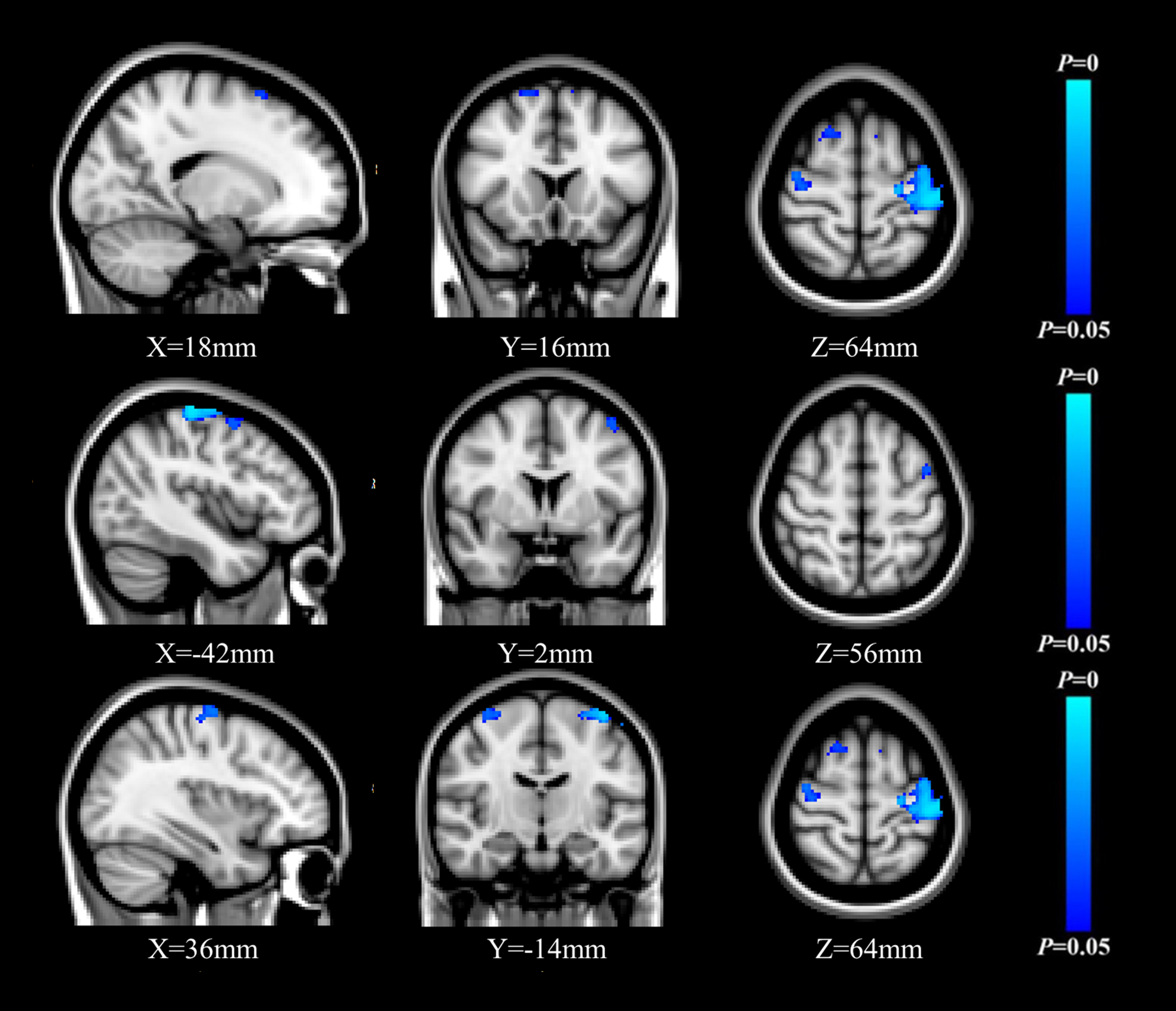
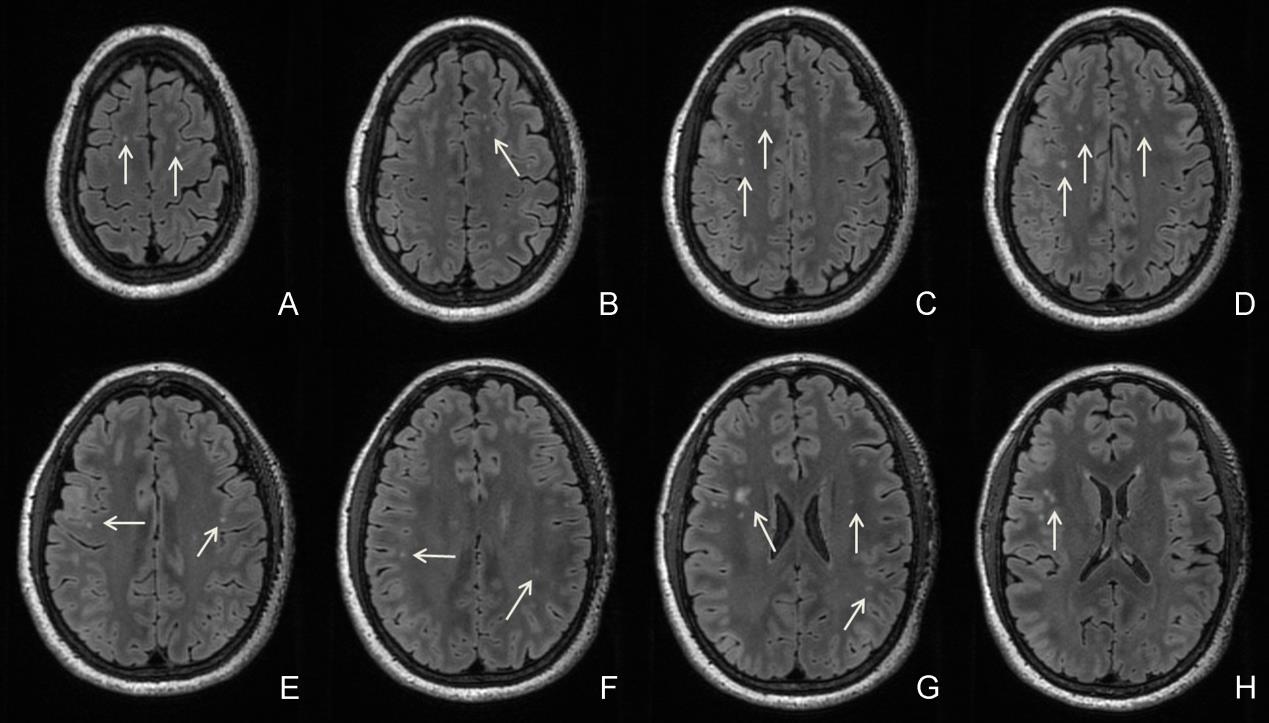
We recruited 18 migraine patients with PFO and 18 migraine patients without PFO. All migraines belong to the type of without aura according to the international classification of headache disorders, 3rd edition (ICHD-3). No differences were observed in terms of gender, year, disease course, duration time and visual analogue scale (VAS) between migraine with PFO and without PFO (Table 1). The data indicated a significant difference in GM reduction in migraine patients with PFO as compared with patients without PFO. The regions were mainly distributed in bilateral precentral gyrus, superior frontal gyrus and left postcentral gyrus and middle frontal gyrus. There was no area exhibited increased GM (Figure 1). In WMLs study, the data showed 7 cases of WMLs were distributed in the frontal lobe and parietal lobe of migraine with PFO, the score ranges were 1-7 points; 5 cases of WMLs were also distributed in the frontal lobe and parietal lobe of migraine without PFO, the score ranges were 1-3 points. The damage degree of migraine with PFO was higher than that of migraine without PFO, but there was no significant statistical difference in WMLs (Figure 2).Discussion
The present study showed that PFO in migraine patients experienced gray matter changes in specific regions, such as the superior frontal gyrus, precentral gyrus, which play an important role in pain modulating system. And changes in these certain brain function networks may be cumulative results in patients suffering long-term repeated pain stimulation [3]. The right-to-left shunts via PFO may allow some paradoxical embolism to enter circulation and stimulate trigeminal nerves, then cause migraine [4]. In addition, we found that the white matter lesions of migraine are distributed in frontal lobe and (or) parietal lobe, but our results do not support a relationship between PFO and WMLs. The reason may be that we only included migraine without aura and the studies about white matter lesions and migraine with aura were more reported in previous literatures. Moreover, most of our patients are young and have relatively few vascular risk factors, lack of micro-emboli formation conditions [5]Conclusion
PFO has a significance influence to brain gray matter abnormalities in migraine and has no clear relationship with white matter lesions. This finding may provide a new insight for clinical treat strategy.Acknowledgements
This work was Supported by the National "Twelfth Five-Year" Plan for Science and Technology Support (2014BAI04B05); the National Key Research and Development Program of China (2016YFC0100300); the National Natural Science Foundation of China (No.81171317, 81471631); the Foundation of the First Affiliated Hospital of Xi’an Jiaotong University (2016MS-02).References
1. Sathasivam, S. and S. Sathasivam, Patent foramen ovale and migraine: what is the relationship between the two? J Cardiol, 2013. 61(4): p. 256-9.
2. Kahya Eren, N., et al., To Be or Not to Be Patent: The Relationship Between Migraine and Patent Foramen Ovale. Headache, 2015. 55(7): p. 934-42.
3.Scheltens, P., et al., A Semiquantitative Rating Scale for the Assessment of Signal Hyperintensities on Magnetic Resonance Imaging. J Neurol Sci, 1993, 114: 7-12.
4. Jia, Z. and S. Yu, Grey matter alterations in migraine: A systematic review and meta-analysis. Neuroimage Clin, 2017. 14: p. 130-140.
5. Yoon, G.J., et al., Right-to-left shunts as a cause of juxtacortical spots in patients with migraine. Eur J Neurol, 2012. 19(8): p. 1086-92.
6. Kruit, M.C., et al., Infarcts in the posterior circulation territory in migraine. The population-based MRI CAMERA study. Brain, 2005. 128(Pt 9): p. 2068-77.
Figures