3652
The multi-play of diffusion tensor imaging and immunohistochemistry to unveil the longitudinal microstructural brain alterations in a closed head brain injury model.1Queensland Brain institute, Brisbane, Australia, 2Adelaide Medical School, University of Adelaide, Adelaide, Australia, 3School of Health Sciences, University of South Australia, Adelaide, Australia
Synopsis
Traumatic brain injury (TBI) is a disease burden worldwide and it is associated with axonal injury and neuroinflammation. Investigating the underlying mechanisms and the progression in the acute and sub-acute stages following TBI non-invasively would aid for early diagnosis and intervention. In this study, we used diffusion tensor imaging (DTI) to investigate the microstructural changes following TBI. Furthermore, we used immunohistochemistry to investigate the axonal injury and microglial activity following TBI. Using DTI, we detected persistent microglial activity associated with TBI which might suggest a possible use of DTI for reflecting on the microstructural changes associated with TBI in humans.
Background
Traumatic brain injury (TBI) is a leading cause of death or disability. Brain injury induces shearing force between white and grey matter initiating microstructural changes and neuroinflammatory response1–3. Several studies aimed to develop non-invasive techniques to monitor these changes following TBI for better diagnosis and possible treatment interventions. The Marmarou weight-drop rodent model of TBI resembles human closed head injury4, and it has been characterized by diffuse axonal injury, contusions, and impairment of cerebral blood flow autoregulation1–3. Furthermore, reduced mean diffusivity and radial diffusivity using diffusion tensor imaging (DTI) has been seen five days post injury5 and these changes correlated with astrogliosis5. Altered white-matter structure 7 days post-TBI has been associated with axonal damage (amyloid precursor protein (APP))6. To date, only one study investigated these changes 30 days post-TBI in female rodents and showed a correlation between FA and astrogliosis in the grey-matter post-TBI7. Interestingly, a recent study showed that females exhibit more severe white-matter damage as compared to males8. The primary objective of this study is to detect a spatiotemporal profile of microstructural alterations and identify the possibility of using DTI to detect the temporal profile of microglial activity following TBI in male rodents.Methods
Adult male Sprague Dawley rats (n = 33, 10-12 weeks old, 375 - 425gm) underwent moderate-severe closed-head TBI using the Marmarou model2. A total of 8 rats underwent MRI imaging at control (pre-TBI), 1, 7, 14, and 30 Days post-TBI. The rest of the animals were perfused for immunohistochemistry (n=5 per time-point). Anatomical, T2-weighted imaging was acquired using a rapid-relaxation-with-enhancement (RARE) sequence with TR/TE=5900/65ms, RARE-factor=8, FOV=32×25x20 mm, and matrix=256×256×40. DTI was acquired using an axial EPI sequence with TR/TE/FA=10000ms/29ms/90o, FOV =24.8 x 24.8 mm, matrix= 108 x 108 x 41, slice thickness=0.5, slice gap = 0.1, 32 directions with b-values=750, 1500 s/mm2, and 4 b0 volumes. DTI and T2 images were corrected for the field bias inhomogeneity, and skull stripped using 3D pulse-coupled neural networks9 and corrected manually. DTI were also corrected for eddy current and motion (FSL-MCFLIRT). The Diffusion Toolkit (DTIFIT) was used to fit the diffusion tensors and generate eigen values and vectors and fractional anisotropy (FA). T2 and DTI images were normalized to the Schwarz rat template non-linearly (fsl-fnirt)10. Differences between time-points post-TBI and sham were calculated using unpaired t-test performed using permutation test (fsl-randomise), with 5000 permutations, and the resulted maps were corrected for multiple comparisons using false discovery rate (p<0.05). Immunohistochemical analysis was performed at 4 different levels of the brain (-0.5, -1.5, -2.5 and -5 from Bregma) using Iba-1 staining to assess microglia number and percentage of activated cells and APP as a marker of axonal injury.Results
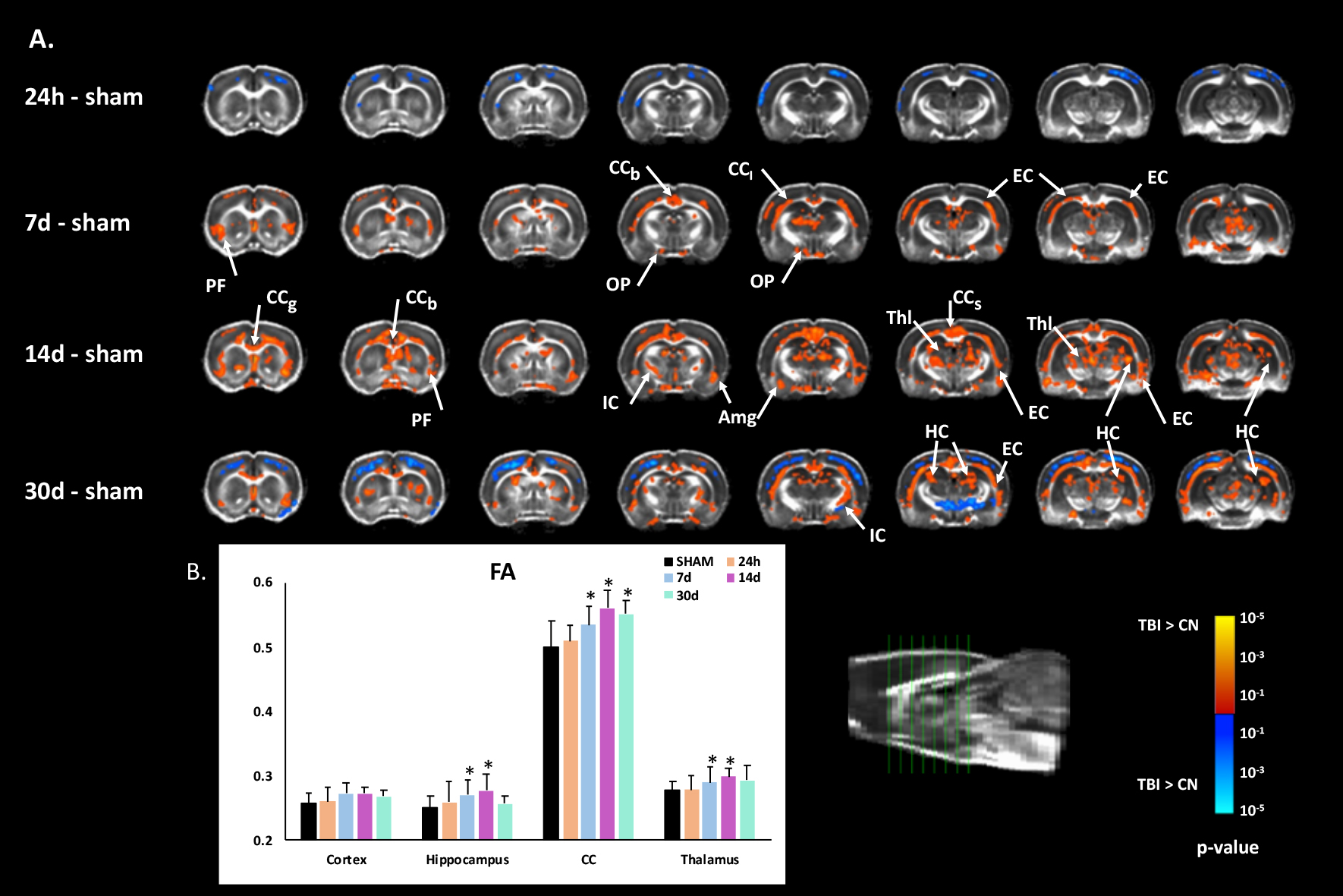
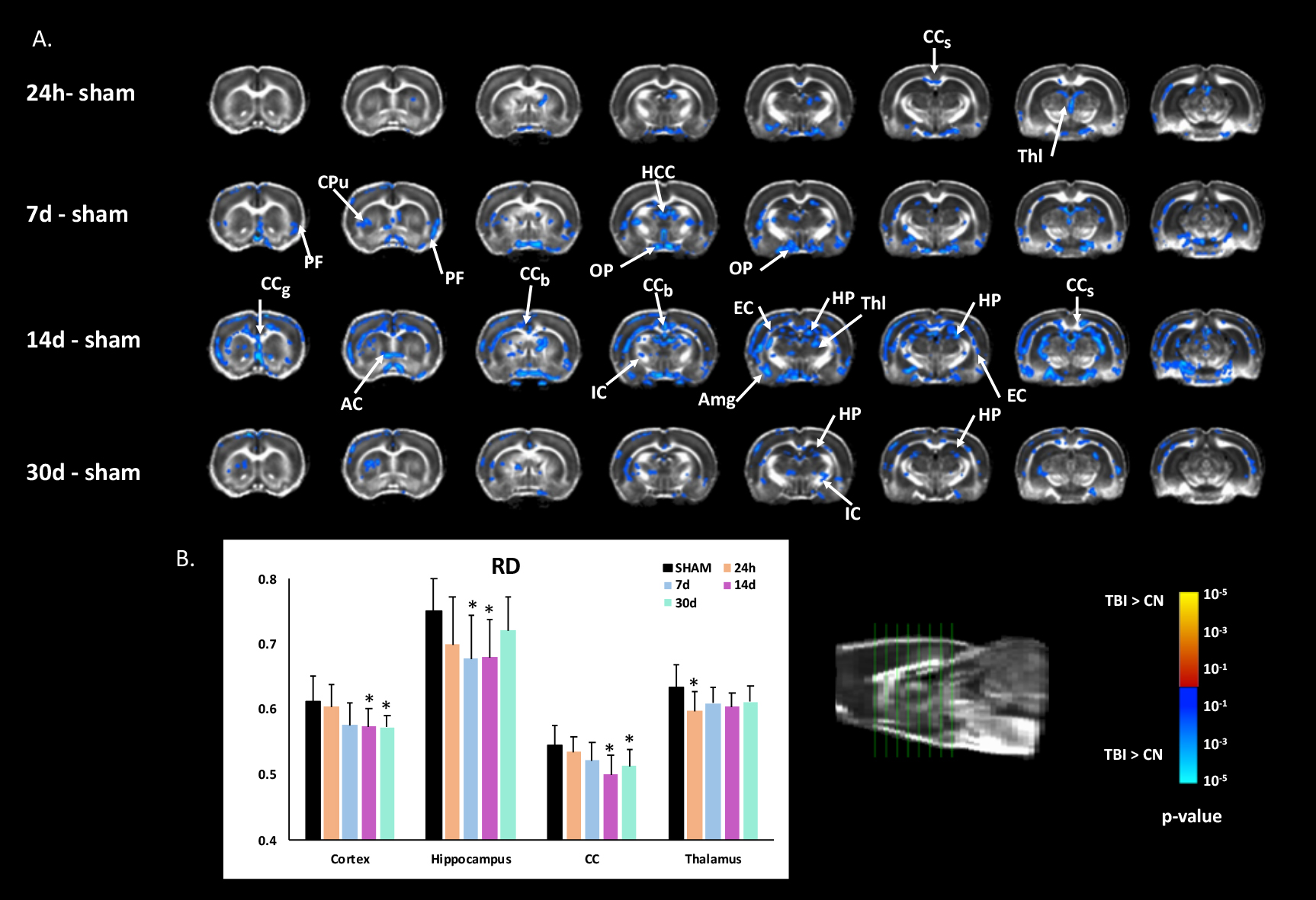
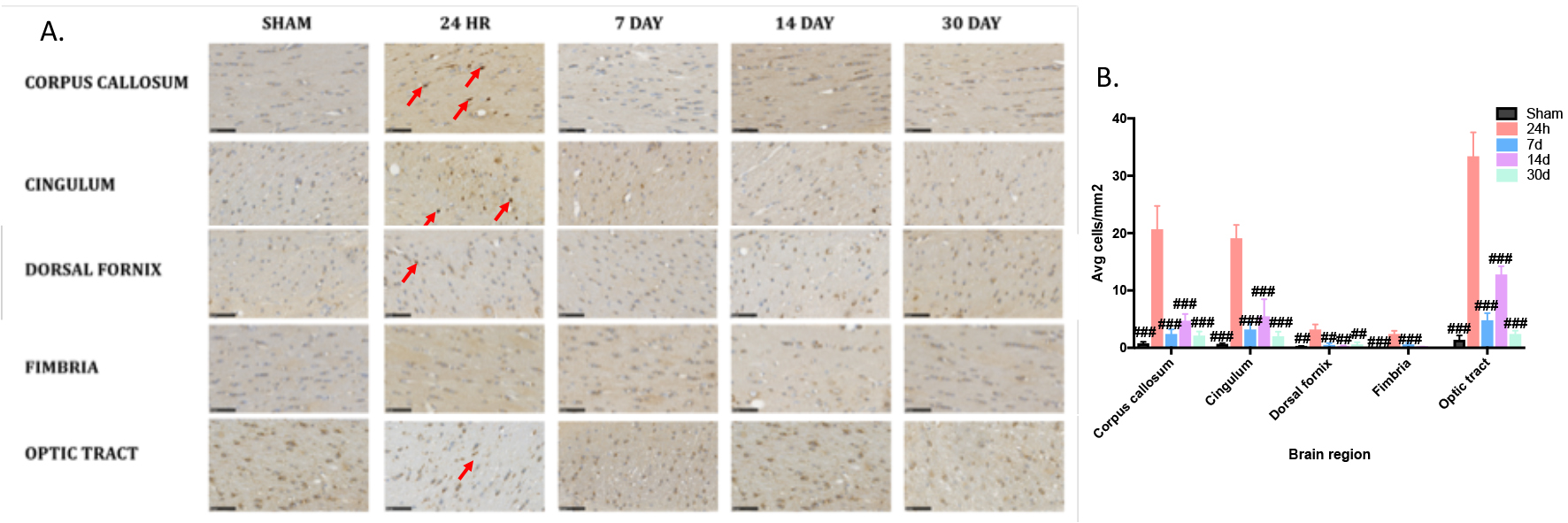
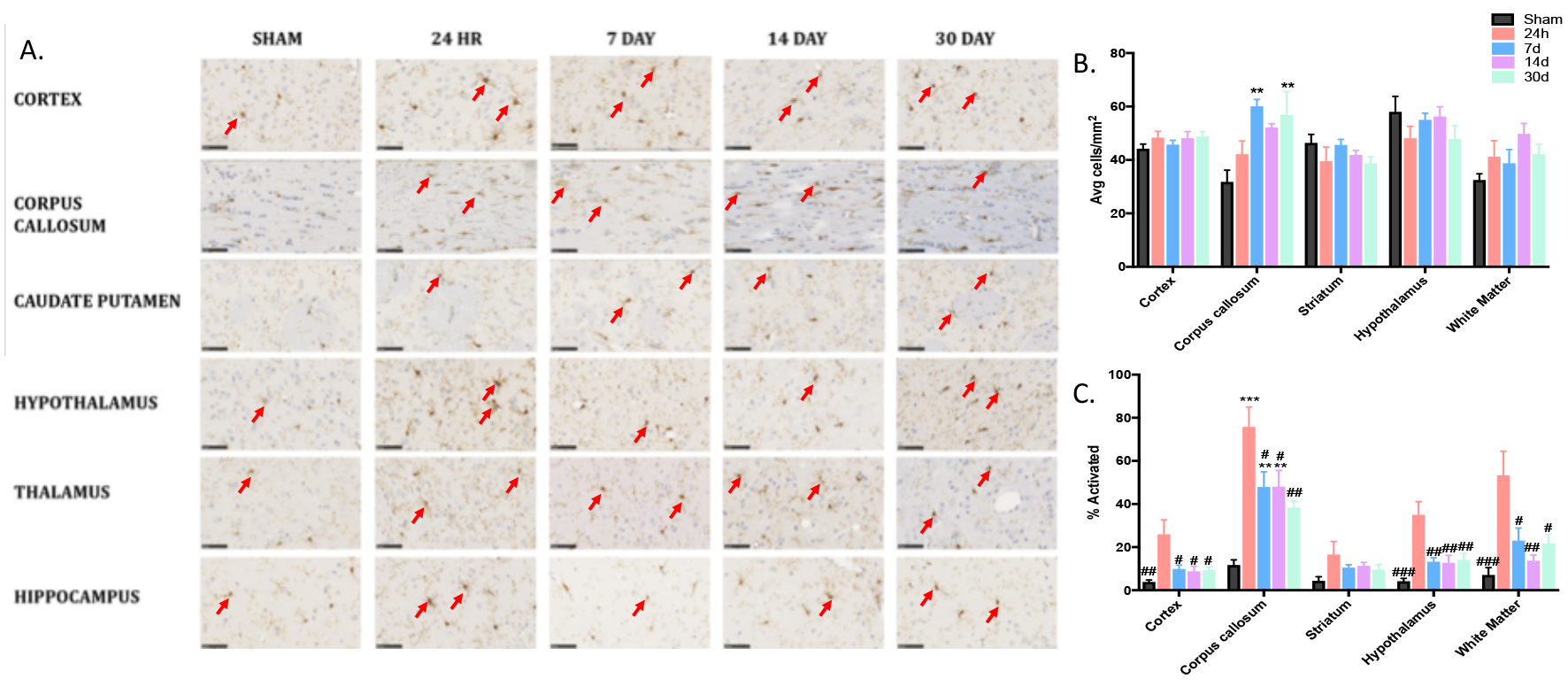
A significant increase in fractional anisotropy (FA) was seen in the white-matter including the corpus callosum (CC), internal and external capsule (IC, EC), optic tract (OP) at 7d, 14d, and 30d and grey-matter in the piriform, amygdala, thalamus, and hippocampus at 7d, 14d and 30d, but was reduced in the cortex at 7d and 30d (Fig.1). Radial diffusivity (RD) was reduced in the CC, IC, EC, OP, anterior commissure (AC), thalamus, amygdala, hippocampus and cortex with most of the changes observed at 14d (Fig.2). At 24hr, APP was significantly increased compared to sham in all ROIs indicating diffuse axonal injury, which was resolved by 7 days post-injury (Fig.3). For total number of microglia, increases were seen in the cortex, CC, and hippocampus, although this was not dependent on time post-injury (Fig.4). For activated microglia, distinct patterns were seen dependent on brain level and region analysed; however, the largest increases in microglial activation were seen at 24h post-injury with highest levels of activation in the CC, as expected given the nature of the experimental injury model.Discussion
Neuroinflammation has been reported in both human and animal studies following a TBI 5,11,12. Most studies which employed DTI to a closed-head injury model focused on the first 10 days post-TBI. Only one study investigated the injury progression over 30 days7 and showed that DTI was more reflected by a change in astrogliosis and demyelination following TBI. The present study was built upon the same concept by incorporating longitudinal imaging with immunohistochemistry showing increased microglia activation corresponding to increased FA suggesting changes in the tissue structure due to the active microglia observed from 24hrs and persistent for 30 days post-TBI. In conclusion, our results suggest the possibility to use DTI to detect microstructural changes including microglial activity post-TBI.Acknowledgements
This work as supported by Motor Accident Insurance Commission (MAIC) (Grant:2014000857), the Queensland Government, Australia for the research grant to FN. This work was also supported by grants from the NeuroSurgical Research Foundation to FC and LCP . We would like to thank the Australian Government support through NCRIS and the National Imaging Facility for the operation of 9.4T MRI at Centre of Advanced Imaging, University of Queensland, Brisbane, Australia.References
1. Mulder G, Rossem K, Reempts J, Borgers M, Verlooy J. Validation of a closed head injury model for use in long-term studies. Acta Neurochir Suppl. 2000;76:409–413.
2. Marmarou a, Foda M a, van den Brink W, Campbell J, Kita H, Demetriadou K. A new model of diffuse brain injury in rats. Part I: Pathophysiology and biomechanics. J Neurosurg. 1994;80:291–300.
3. Xiong Y, Mahmood A, Chopp M. Animal models of traumatic brain injury. Nat Rev Neurosci. 2013;14:128–142.
4. Henninger N, Sicard KM, Li Z, et al. Differential recovery of behavioral status and brain function assessed with functional magnetic resonance imaging after mild traumatic brain injury in the rat. Crit Care Med. 2007;35:2607–2614.
5. Singh K, Trivedi R, Devi MM, Tripathi RP, Khushu S. Longitudinal changes in the DTI measures, anti-GFAP expression and levels of serum inflammatory cytokines following mild traumatic brain injury. Exp Neurol. 2016;275:427–435.
6. Li J, Li X-Y, Feng D-F, Gu L. Quantitative evaluation of microscopic injury with diffusion tensor imaging in a rat model of diffuse axonal injury. Eur J Neurosci. 2011;33:933–945.
7. Tu T-W, Williams RA, Lescher JD, Jikaria N, Turtzo LC, Frank JA. Radiological-pathological correlation of diffusion tensor and magnetization transfer imaging in a closed head traumatic brain injury model. Ann Neurol. 2016;79:907–920.
8. Rubin TG, Catenaccio E, Fleysher R, et al. MRI-defined White Matter Microstructural Alteration Associated with Soccer Heading Is More Extensive in Women than Men. Radiology. 2018;289:478–486. 9. Chou N, Wu J, Bai Bingren J, Qiu A, Chuang K-H. Robust Automatic Rodent Brain Extraction Using 3-D Pulse-Coupled Neural Networks (PCNN). IEEE Trans Image Process. 2011;20:2554–2564.
10. Andersson JLR, Jenkinson M, Smith S. Non-linear registration aka Spatial normalisation. FMRIB Technial Report. In Pract. Epub 2007.
11. Arulsamy A, Teng J, Colton H, Corrigan F, Collins-Praino L. Evaluation of early chronic functional outcomes and their relationship to pre-frontal cortex and hippocampal pathology following moderate-severe traumatic brain injury. Behav Brain Res. 2018;348:127–138.
12. Woodcock T, Morganti-Kossmann MC. The role of markers of inflammation in traumatic brain injury. Front Neurol. 2013;4.
Figures