3587
Q-Space Trajectory Imaging to Untangle Sources of Microstructural White Matter Changes: Comparison of Schizophrenia Subjects and Healthy Controls1Brigham and Women's Hospital, Harvard Medical School, Boston, MA, United States, 2Lund University, Lund, Sweden, 3University Hospital Brno, Brno, Czech Republic, 4Masaryk University, Brno, Czech Republic
Synopsis
The recently proposed q-space trajectory imaging (QTI) analysis for multidimensional dMRI acquisitions with free wave forms quantifies domains of variability (size, shape, orientation) that can explain the sources of microstructural changes in the brain. These previously inaccessible domains are used here to disentangle differences observed in the white matter of schizophrenia patients compared to healthy controls. In this population microscopic anisotropy (shape variability) explains changes in fractional anisotropy, in agreement with a hypothesis of white matter degeneration. This study provides a first proof of principal for the feasibility of applying free wave form based sequences on a clinical population.
Introduction
Diffusion MRI (dMRI) continues to be important for the identification of brain changes across many disorders. While improvements in imaging hardware and software are increasing dMRI sensitivity to brain changes, specificity remains challenging, i.e., the task of associating dMRI changes with pathological or morphological tissue changes. Specificity can be improved by employing elaborated diffusion models. However, typically, fitting more complex models is ill-posed and requires additional assumptions which may not be valid in clinical data1. Alternatively, specificity can be improved by acquiring a more complex data. Recently, multidimensional dMRI acquisitions with free wave forms2 have been proposed alongside the q-space trajectory imaging (QTI) model,3 as a novel acquisition and analysis method that improves specificity by disentangling shape and size variabilities from the diffusion weighted signal.
Improving specificity is especially useful for schizophrenia imaging studies, where current dMRI studies robustly identify white matter changes (especially reduced fractional anisotropy – FA), but mapping these changes back to the biological domain is difficult.4 Moreover, recent studies in schizophrenia suggest that the disorder may involve a number of co-occurring pathologies, related to degeneration damage, developmental abnormalities, and immune system related changes5.
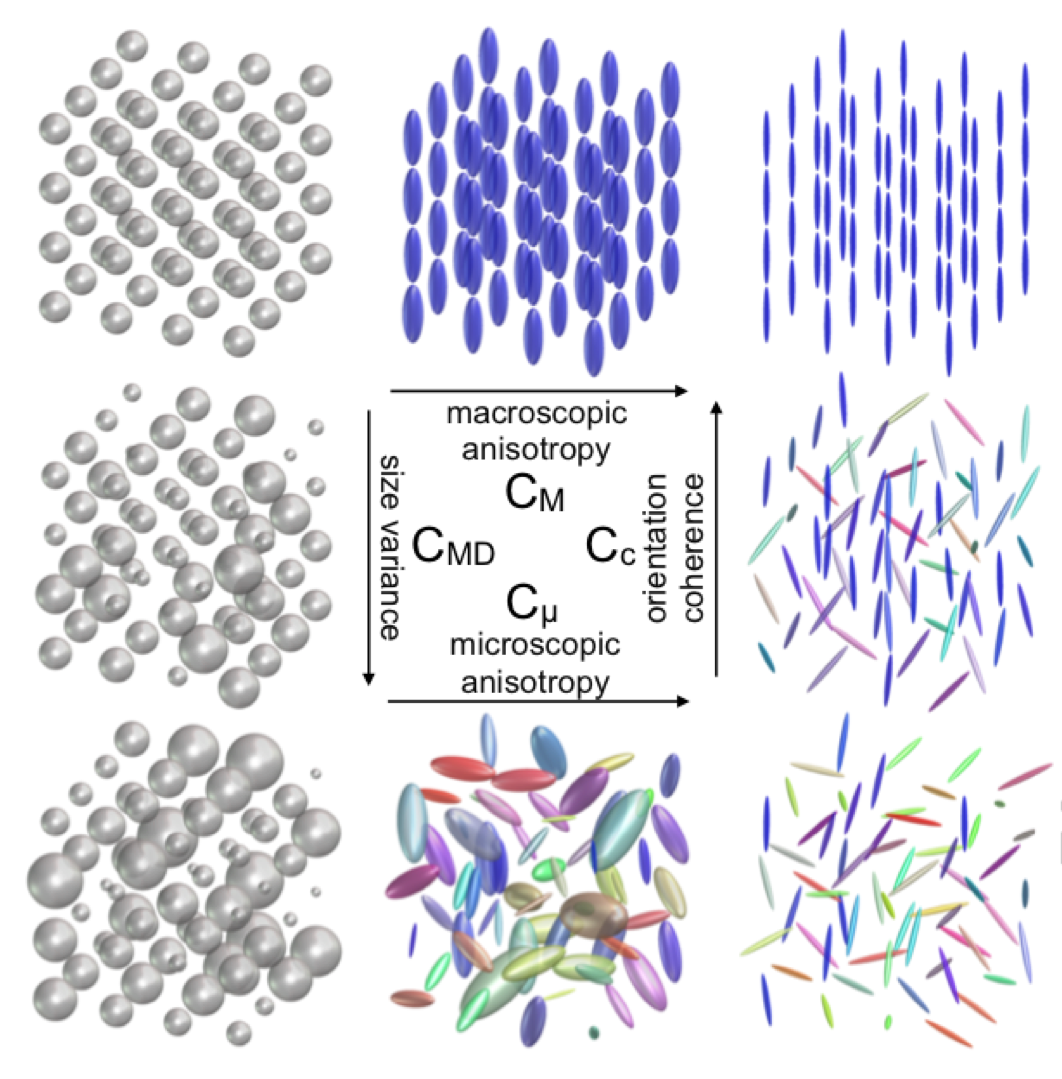
In this work we collected multidimensional dMRI acquisitions from schizophrenia patients and healthy controls, we then applied QTI in order to increase the specificity of the diffusion measures. Using QTI we were able to explore three domains of variability, which may explain dMRI changes: 1) microscopic anisotropy, Cμ. 2) orientation coherence, Cc. And 3) size variance, CMD.
Methods
QTI is estimated from a collection of free wave forms with b-tensors shaped like sticks, planes and spheres.3 The different shapes and their orientation allow the estimation of a 4th order coefficient matrix that has more degrees of freedom than the 4th order Kurtosis matrix estimated from conventional dMRI measures (i.e., just sticks).
Free wave forms were implemented and installed on a 3T Siemens Prisma scanner at the Central European Institute of Technology, Brno, Czech Republic. The wave forms included: 2-shells of sticks with b-values of 1000 s/mm2, and 2000 s/mm2, and with 30 directions in each shell; 6 planes (perpendicular to the conventional 6 direction acquisition) collected twice with b=1000 and b=2000; and 5 spheres with b-values of 50, 250, 500, 1000 and 2000, repeated 3 times. In addition seven b=0 images were acquired. The total number of volumes was 95. The data was collected with resolution of 2mmX2mmX4mm, 35 slices, TE=145ms, TR=6500ms, totaling 12:54 minutes of scan.
The sequence was applied on 21 inpatient subjects suffering from schizophrenia (4F/17M; mean age 34.9), and 18 controls (4F/14M; mean age 32.6). All subjects provided informed consent, and the study was approved by the local institutional review board.
The data was manually masked, eddy current and motion corrected. Then in each voxel the data was fitted to a second and fourth order tensors using the QTI framework as implemented in the multidimensional diffusion MRI toolbox.6 The FA image was used to construct a white matter skeleton using TBSS. Then the QTI images (Cμ , Cc and CMD) were projected onto the same skeleton. The values were averaged over the skeleton and compared between the groups using a general linear model with age and gender as covariates.
Results
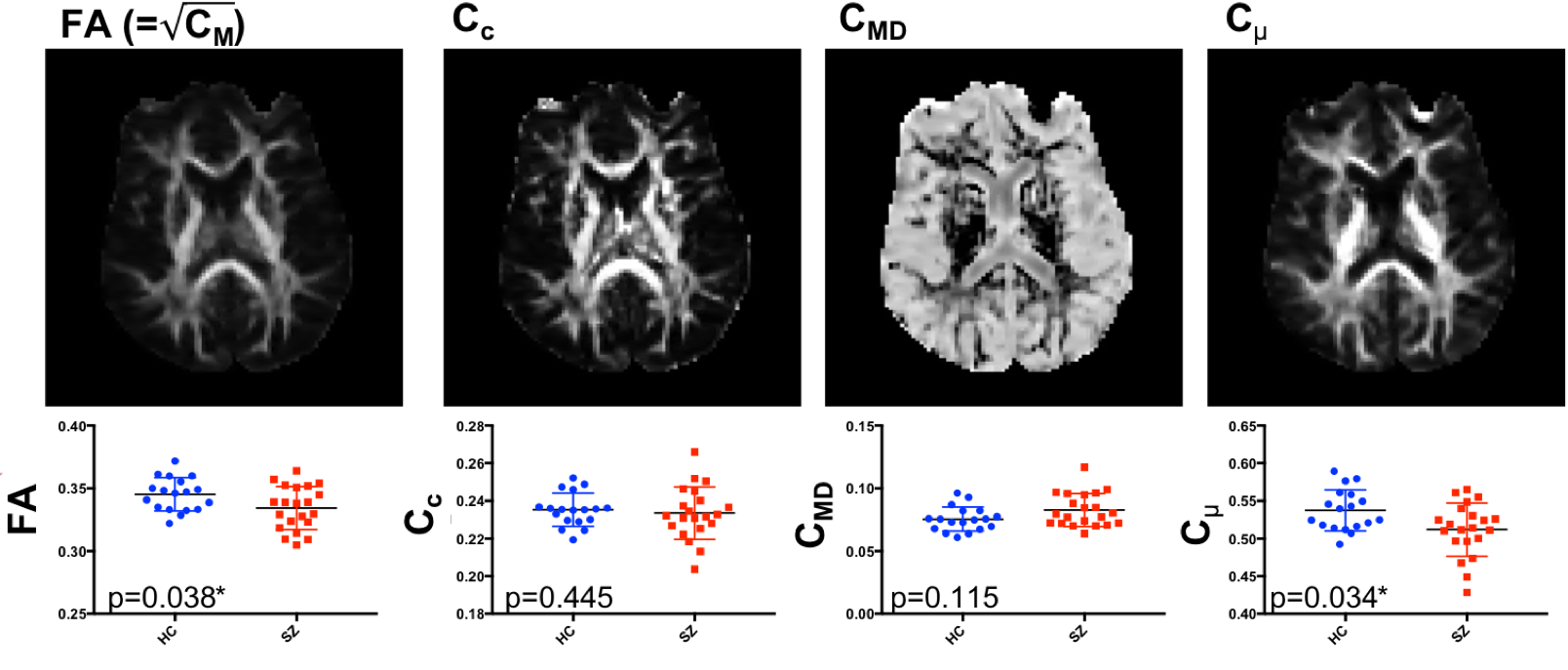
Similar to previous studies, FA in the schizophrenia subjects was significantly lower than controls (p=0.038). Applying QTI on the same data explained the group differences by a significant decrease in microscopic anisotropy, Cμ (p=0.034). Differences in orientation coherence, Cc, were not significant (p=0.445), and an increase in size variance, CMD, did not reach the significance threshold (p=0.115).Discussion
Our analysis demonstrates that the microscopic anisotropy is equivalent to FA in terms of separation between schizophrenia patients and controls. However, since QTI has three domains rather than one, we can now deduce that the FA changes were mainly driven by shape variability and to a lesser extent by size or orientation variability. Such a finding is aligned with a hypothesis that at the chronic stages of schizophrenia degenerative processes (expected to affect shape) are more dominant than developmental variability (expected to affect orientation) or immune responses (expected to affect size).Conclusions
This study provides a first proof of principal for the feasibility of applying free wave form based sequences on a clinical population. With the introduction of multi-band and more efficient wave forms the scan time could be further decreased, or alternatively the resolution increased. With regards to schizophrenia studies, additional QTI data from subjects closer to psychosis onset may shed more light on the time course and spatial extent of each expected pathological process.Acknowledgements
This study was funded in part by NIH grants R01MH074794, R01MH108574, R01MH102377,P41EB015902.References
1. Lampinen B, Szczepankiewicz F, Mårtensson J et al. Neurite density imaging versus imaging of microscopic anisotropy in diffusion MRI: A model comparison using spherical tensor encoding. Neuroimage. 2017;147:517-531.
2. Topgaard D. Multidimensional diffusion MRI. J Magn Reson 2017;275:98-113.
3. Westin CF, Knutsson H, Pasternak O. Q-space trajectory imaging for multidimensional diffusion MRI of the human brain. Neuroimage. 2016;135:345-62.
4. O'Donnell LJ,Pasternak O. Does diffusion MRI tell us anything about the white matter? An overview of methods and pitfalls. Schizophr Res. 2015;161(1):133-41
5. Pasternak O, Kelly S, Sydnor VJ, et al. Advances in microstructural diffusion neuroimaging for psychiatric disorders. Neuroimage. 2018;182:259-282.
6. https://github.com/markus-nilsson/md-dmri.git
Figures