3586
Investigation of relationships between systemic inflammation and brain structure in chronic obstructive pulmonary disease (COPD)1Neurosciences Research Centre, Molecular and Clinical Research Institute, St George’s Uni, Neurosciences Research Centre, Molecular and Clinical Research Institute, St George’s, University of London, London, United Kingdom, 2Institute for Infection and Immunity, St George's University of London, London, United Kingdom, Institute for Infection and Immunity, St George's, University of London, London, United Kingdom, 3Neurosciences Research Centre, Molecular and Clinical Research Institute, St George’s, University of London, Neurosciences Research Centre, Molecular and Clinical Research Institute, St George’s, University of London, London, United Kingdom, 4St George’s, University of London, London, United Kingdom, 5Academic Respiratory Unit, School of Clinical Sciences, University of Bristol, Bristol, United Kingdom, Bristol, United Kingdom, 6Institute for Infection and Immunity, St George's, University of London, London, United Kingdom
Synopsis
COPD patients have increased systemic inflammation and increased structural brain damage. 23 COPD patients with coronary artery disease (CAD), and 24 people without COPD matched for smoking, and CAD severity (Gensini score) were studied. COPD patients had more white matter lesions and microstructural tract abnormalities compared to controls. Systemic inflammation (high sensitivity C-reactive protein and fibrinogen) was associated with microstructural brain damage in whole-group analyses. These results suggest a systemic inflammatory process in COPD, which may contribute to white matter abnormalities, consistent with those reported in small vessel disease.
Introduction
Chronic obstructive pulmonary disease (COPD) patients commonly have structural brain abnormalities 1 and are at increased risk of cardiovascular damage.2 Systemic inflammation has been implicated as a contributing factor to this increased cardiovascular damage, potentially by increasing arterial stiffness.3 It remains unclear whether systemic inflammation is related to brain damage in COPD. Here we investigate the relationship between markers of systemic inflammation and their relationship to brain damage in COPD patients and control participants who were matched for smoking history and coronary artery disease severity.Method
23 COPD patients (Age, 71 ± 8 years, 78% male, FEV1 78 ± 20), 24 people without COPD (Age, 65 ± 6, 75% male, FEV1 94 ± 20) matched for smoking, and coronary artery disease (CAD) severity (Gensini score) 4 were studied. Exclusion criteria included: chest infection within the last six weeks, known neurological disease or stroke, uncontrolled hypertension, diabetes mellitus, and obstructive sleep apnoea. The markers of systemic inflammation used were: high sensitivity C-reactive protein (hsCRP) and neutrophil/lymphocyte ratio, and we also measured fibrinogen - a component of the coagulation pathway elevated in acute inflammation. 3T magnetic resonance imaging was acquired and analysed as follows: high-resolution T1-weighted imaging provided tissue volume as % intracranial volume for grey matter, white matter, and cerebrospinal fluid 5; fluid-attenuated inversion recovery imaging enabled manual white matter lesion volume (WMLV) computation; diffusion tensor imaging (DTI) provided markers of tissue microstructure (fractional anisotropy, FA), and ultrastructure (mean diffusivity, MD) within the normal appearing white matter (NAWM) 6, and white matter tracts using tract-based spatial statistics.7 DTI was also used to calculate DSEG θ 8, a novel marker of global brain damage. Group differences were assessed using parametric (Gaussian data) and non-parametric (non-Gaussian data) models. Whole-group effects and group interactions between systemic inflammatory markers and brain damage were assessed using analysis of covariance (ANCOVA) models, which included age and sex as covariates. Whole-group non-parametric permutation based correlations between tract-based FA and MD and systemic inflammatory markers were performed on a voxel-by-voxel basis.7 These results were corrected for age, sex, and multiple comparisons.Results
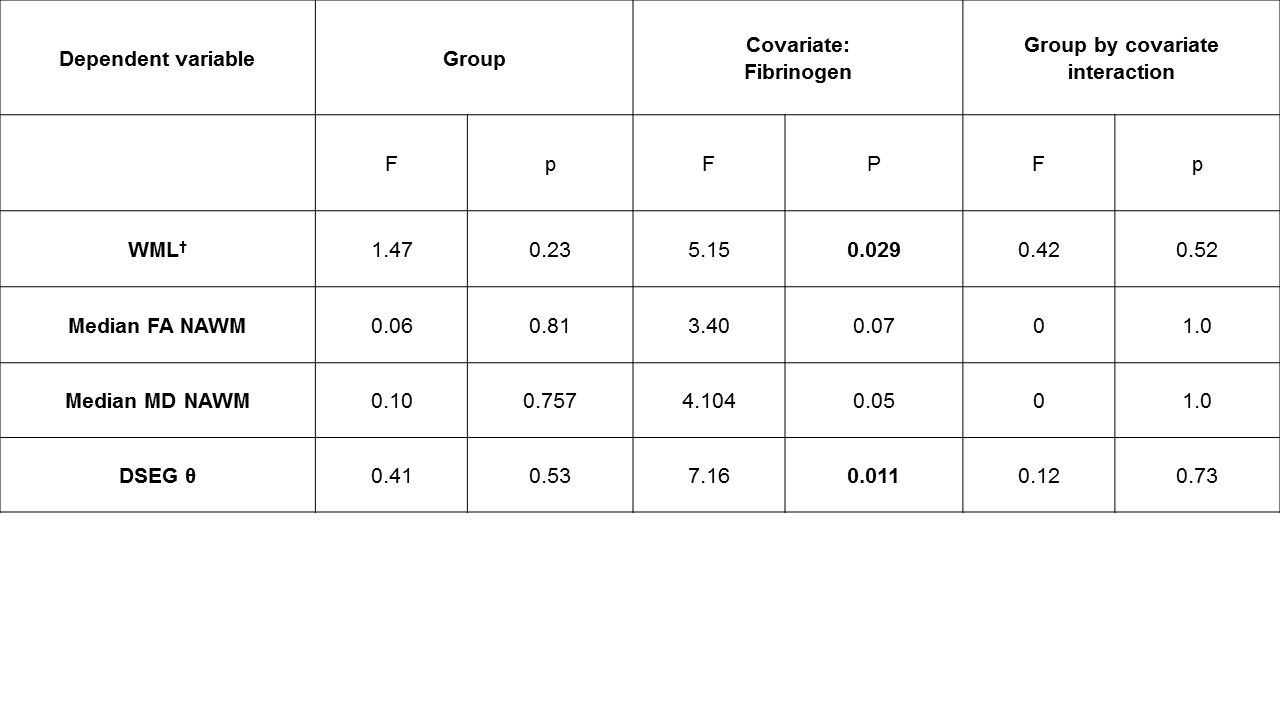
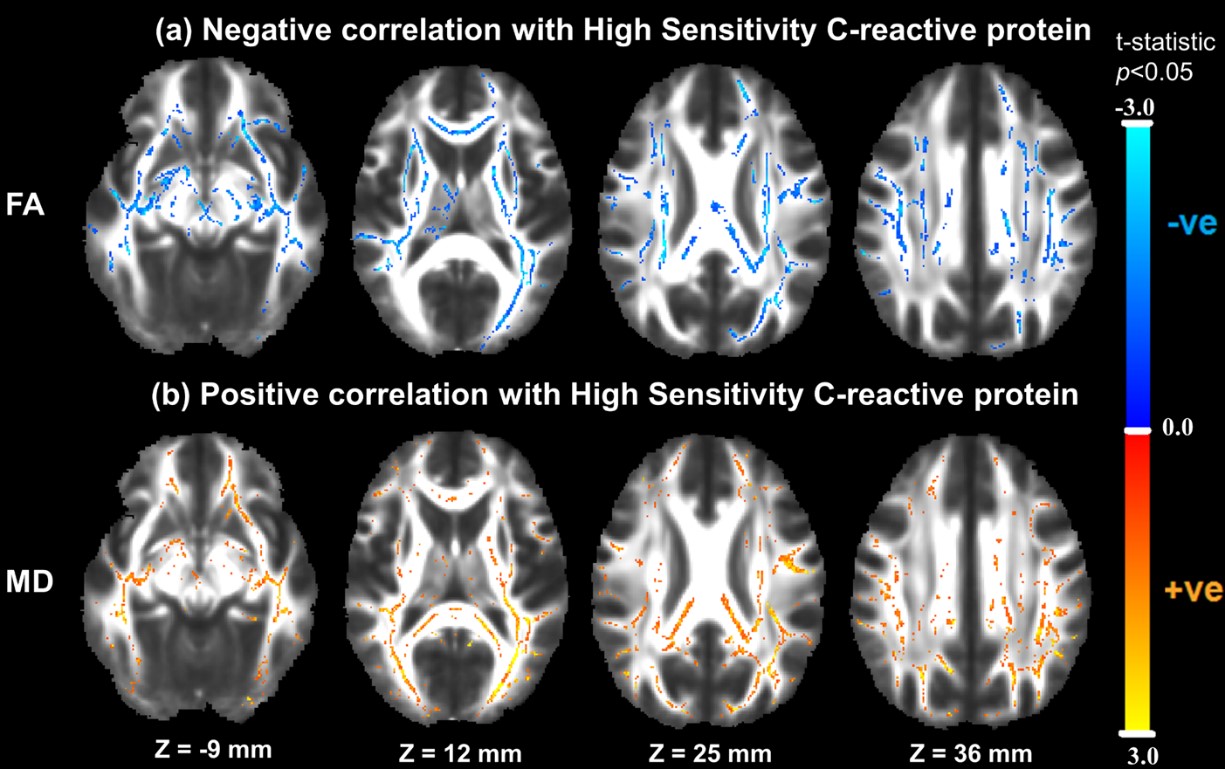
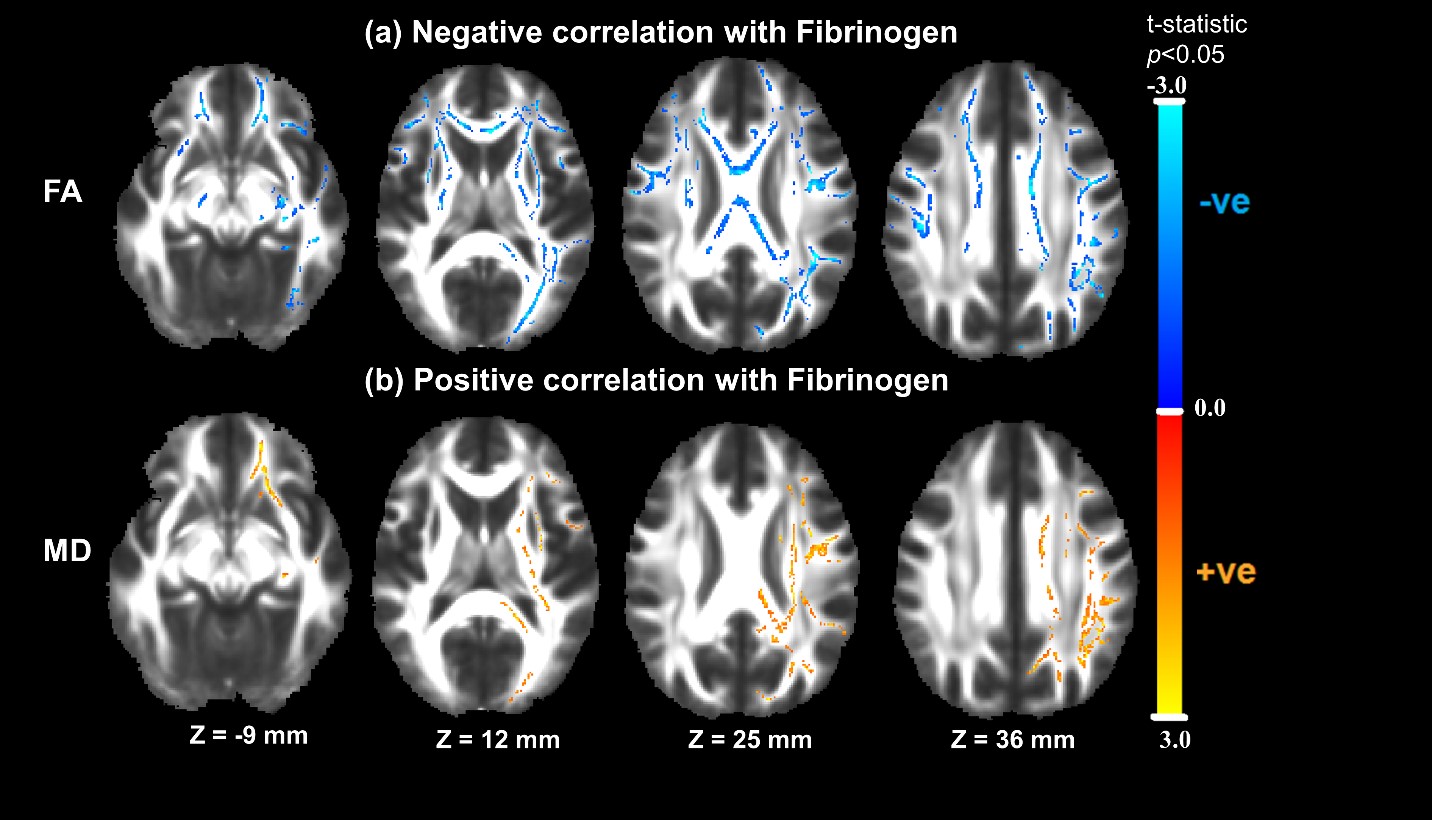
COPD patients had significantly lower lung function and greater hsCRP, neutrophil/lymphocyte ratio and WMLV compared to controls (Table 1). Brain volumes, FA and MD and DSEG θ were not significantly different between the groups. Whole-group ANCOVA analyses (Table 2) showed that hsCRP was associated with median FA (p=0.002). Fibrinogen was associated with WMLV (p=0.029) and DSEG θ (p=0.011) but not with FA or MD in NAWM (Table 3). As there were no group interactions between markers of systemic inflammation and brain damage (Table 2,3) whole-group correlations with tract-based FA and MD, were performed. COPD patients had lower tract-based FA and greater tract-based MD than controls (p<0.05). Whole-group correlations with inflammatory markers indicated that greater hsCRP (Figure 1) and greater fibrinogen (Figure 2) were negatively associated with tract-based FA and positively associated with tract-based MD (p<0.05). Neutrophil/lymphocyte ratio did not correlate with tract-based FA and MD or the aforementioned markers of brain damage.Discussion
COPD patients have increased systemic inflammation (as evidenced by hsCRP and neutrophil/lymphocyte ratio) and, greater WMLV and white matter tract abnormalities, than controls matched for smoking history and coronary artery disease severity. Our findings are consistent with previous studies in other diseases reporting that fibrinogen levels are significantly associated with WMLV in small vessel disease (SVD).9 Furthermore, associations between systemic inflammation and white matter abnormalities have been reported in SVD 10, Parkinson’s disease 11, Alzheimer’s disease 12 and Obstructive sleep apnea.13 Systemic inflammation is a cardiovascular risk factor that may link pulmonary and vascular disease.14 Cardiovascular risk factors are thought to accelerate age-related neurodegeneration, presenting as white matter lesions and microstructural damage 15 - features of SVD. Some of the possible pathophysiologic mechanisms to explain this study's findings are (1) systemic inflammatory cells, possibly originating from the lungs 16, inducing neuroinflammation 17, or (2) increased arterial stiffness, reduced vessel compliance and increased pressure pulsatility, resulting in vascular remodelling, cerebral hypoperfusion, and cell death.18,19 One of the limitations of this study is that it is not possible to determine the pathophysiology contributing to changes in FA and MD, since decreased FA and increased MD also occurs in demyelination, 20 axonal damage, 21 and inflammatory gliosis.22 It is also not clear whether these changes in diffusion parameters are reversible.Conclusion
To our knowledge, this study provides the first evidence of a link between markers of systemic inflammation and white matter abnormalities in COPD. These results suggest a systemic inflammatory process in COPD, which may contribute to white matter abnormalities consistent with those reported in small vessel disease.Acknowledgements
No acknowledgement found.References
1. Dodd JW, Chung AW, van den Broek MD, Barrick TR, Charlton RA, Jones PW. Brain structure and function in chronic obstructive pulmonary disease: a multimodal cranial magnetic resonance imaging study. Am J Respir Crit Care Med. 2012;186(3):240-245.
2. Maclay JD, McAllister DA, Mills NL, et al. Vascular dysfunction in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2009;180(6):513-520.
3. Park S, Lakatta EG. Role of inflammation in the pathogenesis of arterial stiffness. Yonsei medical journal. 2012;53(2):258-261.
4. Gensini GG. A more meaningful scoring system for determining the severity of coronary heart disease. Am J Cardiol. 1983;51(3):606.
5. Lambert C, Sam Narean J, Benjamin P, Zeestraten E, Barrick TR, Markus HS. Characterising the grey matter correlates of leukoaraiosis in cerebral small vessel disease. NeuroImage : Clinical. 2015;9:194-205.
6. Zeestraten EA, Benjamin P, Lambert C, et al. Application of Diffusion Tensor Imaging Parameters to Detect Change in Longitudinal Studies in Cerebral Small Vessel Disease. PLoS One. 2016;11(1):e0147836.
7. Smith SM, Jenkinson M, Johansen-Berg H, et al. Tract-based spatial statistics: Voxelwise analysis of multi-subject diffusion data. NeuroImage. 2006;31(4):1487-1505.
8. Williams OA, Zeestraten EA, Benjamin P, et al. Diffusion tensor image segmentation of the cerebrum provides a single measure of cerebral small vessel disease severity related to cognitive change. Neuroimage Clin. 2017;16:330-342.
9. Martí-Fàbregas J, Valencia C, Pujol J, García-Sánchez C, Martí-Vilalta JL. Fibrinogen and the Amount of Leukoaraiosis in Patients with Symptomatic Small-Vessel Disease. European Neurology. 2002;48(4):185-190.
10. Wersching H, Duning T, Lohmann H, et al. Serum C-reactive protein is linked to cerebral microstructural integrity and cognitive function. Neurology. 2010;74(13):1022-1029.
11. Chiang P-L, Chen H-L, Lu C-H, et al. White matter damage and systemic inflammation in Parkinson's disease. BMC neuroscience. 2017;18(1):48-48.
12. Swardfager W, Yu D, Ramirez J, et al. Peripheral inflammatory markers indicate microstructural damage within periventricular white matter hyperintensities in Alzheimer's disease: A preliminary report. Alzheimers Dement (Amst). 2017;7:56-60.
13. Chen HL, Lu CH, Lin HC, et al. White matter damage and systemic inflammation in obstructive sleep apnea. Sleep. 2015;38(3):361-370.
14. McAllister DA, Maclay JD, Mills NL, et al. Arterial stiffness is independently associated with emphysema severity in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2007;176(12):1208-1214.
15. Wardlaw JM, Smith EE, Biessels GJ, et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol. 2013;12(8):822-838. 16. Jiang R, Burke GL, Enright PL, et al. Inflammatory Markers and Longitudinal Lung Function Decline in the Elderly. American Journal of Epidemiology. 2008;168(6):602-610.
17. Varatharaj A, Galea I. The blood-brain barrier in systemic inflammation. Brain, Behavior, and Immunity. 2017;60:1-12.
18. Poels MM, Zaccai K, Verwoert GC, et al. Arterial stiffness and cerebral small vessel disease: the Rotterdam Scan Study. Stroke. 2012;43(10):2637-2642.
19. Dodd JW. Lung disease as a determinant of cognitive decline and dementia. Alzheimer's research & therapy. 2015;7(1):32-32.
20. Sbardella E, Petsas N, Tona F, et al. Assessing the correlation between grey and white matter damage with motor and cognitive impairment in multiple sclerosis patients. PLoS One. 2013;8(5):e63250. 21. Jang SH. Diffusion tensor imaging studies on corticospinal tract injury following traumatic brain injury: a review. NeuroRehabilitation. 2011;29(4):339-345.
22. Lu CH, Chen HL, Chang WN, et al. Assessing the chronic neuropsychologic sequelae of human immunodeficiency virus-negative cryptococcal meningitis by using diffusion tensor imaging. AJNR Am J Neuroradiol. 2011;32(7):1333-1339.
Figures
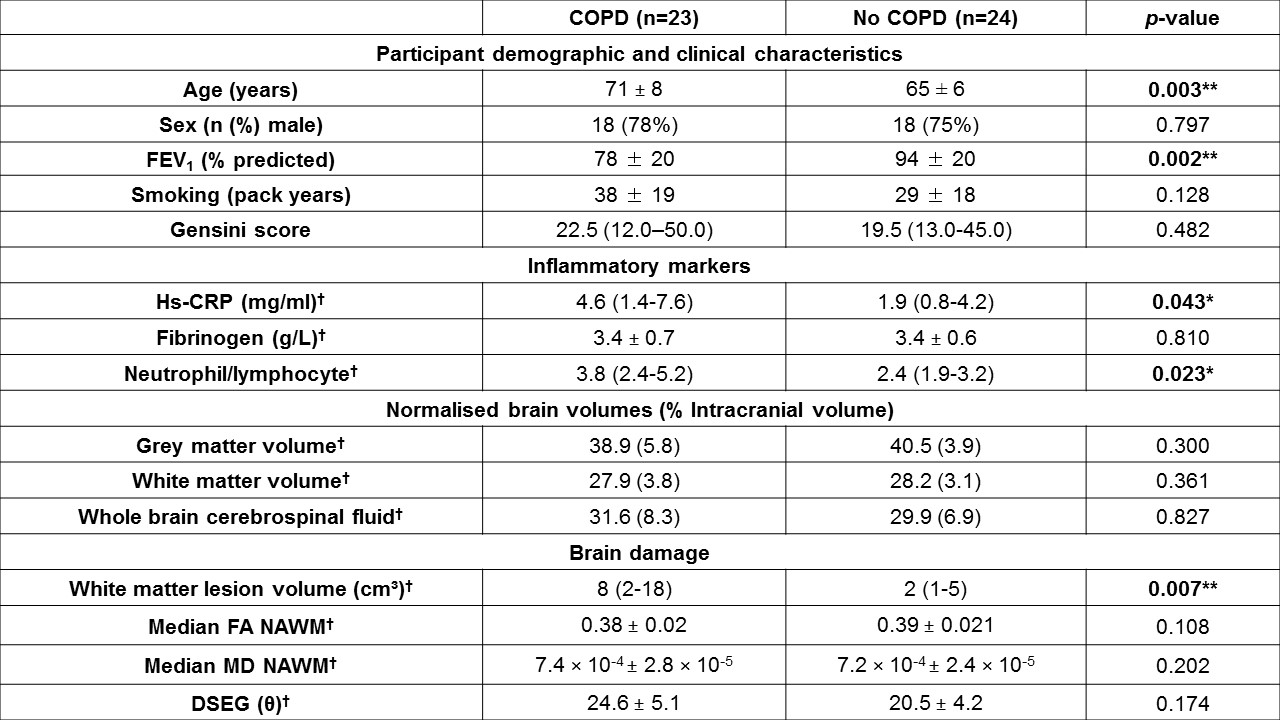
Table 1. Comparisons between people with and without COPD. Values are given as mean ± standard deviation or median (interquartile range). Statistical comparisons were made using independent t-tests, Chi-squared tests or Mann-Whitney U test as appropriate. Bold denotes significance with respect to *p<0.05, **p<0.01 and †results are corrected for age and sex. Abbreviations: FEV1 – forced expiratory volume in one second, hs-CRP – high sensitivity C-reactive protein, FA – fractional anisotropy, MD – mean diffusivity, NAWM – normal appearing white matter.
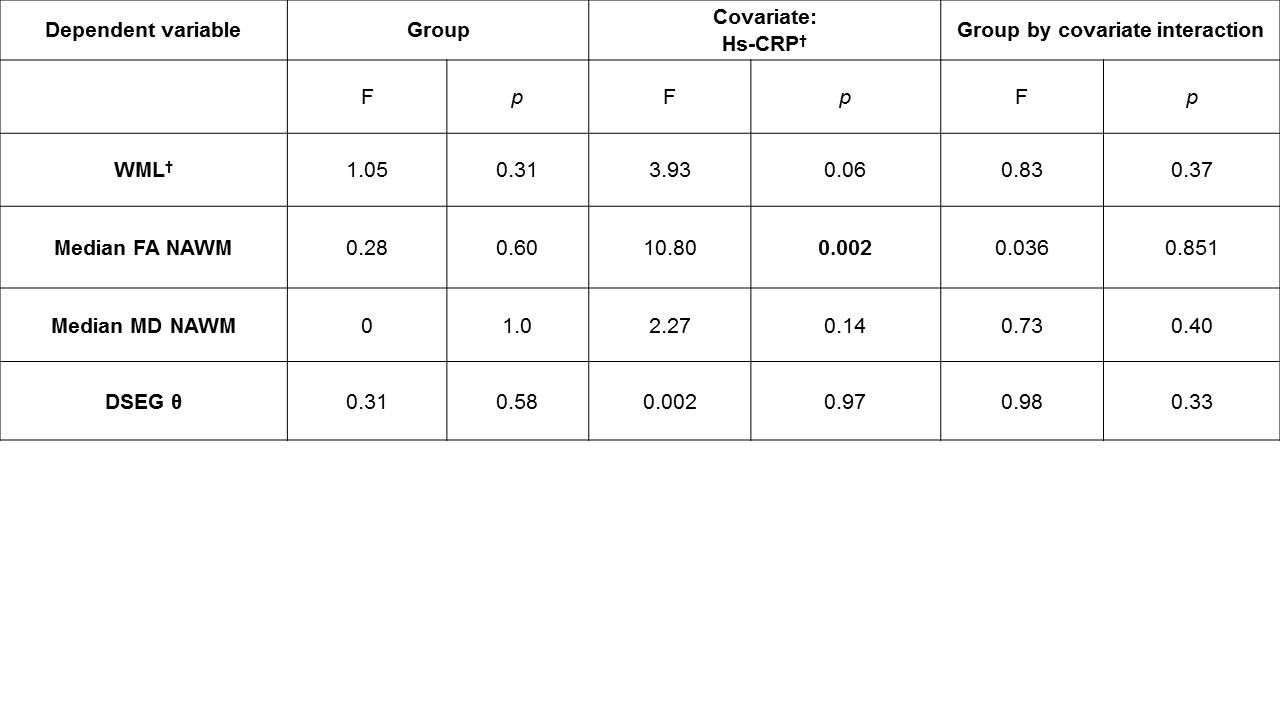
Table 2. ANCOVA model of relationships between the dependent variables and hs-CRP. Analysis of covariance (ANCOVA) testing for the following main effects of group and hs-CRP on brain damage markers. The model also tested the group by hs-CRP interactions. Age and sex were included in this model. Abbreviations: CSF – cerebrospinal fluid, WML – white matter lesion, FA – fractional anisotropy, MD – mean diffusivity, NAWM – normal appearing white matter, hs-CRP – high sensitivity C-reactive protein. †Variable was log transformed for parametric analysis.