3533
Clinical feasibility of multi-band diffusion tensor imaging (DTI) using simultaneous multi-slice acquisition for presurgical planning: Comparisons with standard DTI in patients with brain tumorMehrnaz Jenabi1, Madeleine Gene2, Nicholas s Cho1, Ricardo Otazo3, Robert Young1, Andrei I Holodny1, and Kyung Peck3
1Radiology, MSKCC, New York, NY, United States, 2MSKCC, New York, NY, United States, 3Medical physics, MSKCC, New York, NY, United States
Synopsis
Standard diffusion tensor imaging (s-DTI) is currently utilized during presurgical planning to visualize white matter tracts despite its long scanning time. Multi-band DTI (mb-DTI) utilizes simultaneous multi-slice excitation, which greatly reduces scanning time and increases coverage. In this study, 42 patients with brain tumor were analyzed using mb-DTI and s-DTI in the arcuate fasciculus and corticospinal tract, two critical white matter tracts for language and motor function, respectively. When using mb-DTI, scanning time was reduced by 40% and the image quality and quantitative parameters were preserved. This study demonstrated the clinical feasibility and potential advantages of mb-DTI during presurgical planning
Introduction
Diffusion tensor imaging (DTI) plays an important role in neurosurgical planning of brain tumor resection by visualizing the intricate structural network of white matter fibers in the surrounding brain tissue. However, limitations of standard DTI (s-DTI) using single shot EPI include its long scanning time, limited spatial resolution, and limited coverage. Simultaneous multi-slice excitation has been proposed to accelerate image acquisition times and increase slice coverage.1,2 Multi-band DTI (mb-DTI) is a new technique that utilizes simultaneous multi-slice excitation, but assessment of its clinical feasibility remains limited to a few studies involving healthy controls and a small number of clinical cases.3,4 Further research involving mb-DTI in patient populations remains critical in assessing its potential advantages in terms of scanning time and image quality for presurgical planning. The purpose of this study is to qualitatively and quantitatively compare the tractography results from s-DTI and mb-DTI in patients with brain tumor for the arcuate fasciculus (AF) and corticospinal tract (CST), which are major white tracts for language and motor function, respectively.Methods
Forty-two patients with brain tumor (mean age=56±14(SD), male/female=18/24) who underwent a presurgical planning MRI protocol involving both whole brain s-DTI and mb-DTI in the same session were analyzed. All MR images were acquired using a GE 3T (750w) clinical scanner and a GE 24 channel neurovascular head coil. The imaging parameters for s-DTI were: TR/TE=11000/74.8 ms; slice thickness=3 mm; number of slices=48; field of view (FOV)=240×240 mm2; matrix size=128×128; b=1000 s/mm2; 25 directions. The imaging parameters for mb-DTI were selected to be similar to the s-DTI: TR/TE = 6500/75.7 ms; number of multi-bands=2; slice thickness=3 mm; number of slices=60; FOV=240×240 mm2, matrix size=128×128; b=1000 s/mm2; 25 directions. The acquisition times were 5 min 25 sec for s-DTI and 3 min 2 sec for mb-DTI. In addition, 3-dimensional T1-weighted images were acquired for anatomical information. The distortion caused by eddy currents was corrected using FSL. Data was corrected for image distortion induced by local field inhomogeneity in sinuses near the orbital frontal cortex and area near the ear canals. DSIstudio was used for tensor analysis and tractography analysis. Tract-specific analysis to determine the fractional anisotropy (FA), tract volume, and tract length was applied into the AF and CST. Seed ROIs were set at the superior temporal gyrus and inferior frontal gyrus for the AF and at the pons and foot motor area for the CST tract. Two-tailed, paired t-tests were used to assess the differences in parameters between s-DTI and mb-DTI.Results
Scan time was reduced by approximately 40% when using mb-DTI instead of s-DTI. Moreover, mb-DTI was able to generate images with very similar appearance to s-DTI for whole-brain FA maps (Fig 1), whole-brain tractography (Fig 2), AF tractography (Fig 3), and CST tractography (Fig 4), which was qualitatively validated by a neuroradiologist. When comparing the quantitative diffusion parameters of fiber length, fiber volume, and FA between mb-DTI and s-DTI in the whole-brain, AF, and CST, these parameters were slightly higher for mb-DTI than in s-DTI for nearly all subjects. Moreover, these small differences at the individual level resulted in a statistically significant difference in FA values between mb-DTI and s-DTI for the whole-brain (mb-DTI/s-DTI=0.48±0.02/0.47±0.02), AF (0.55±0.04/0.53±0.04), and CST (0.60±0.03/0.58±0.03) as well as in fiber length (72±14/58±13) and fiber volume (2760±1280/2080±970) in the AF (p<0.0001 for all).Discussion
Our data shows that s-DTI using a single shot EPI and mb-DTI using simultaneous multi-slice acquisition with 2 multi-bands produced very similar results for the fiber tractography of the AF and CST, two white matter tracts of critical importance during presurgical planning. These results suggest that mb-DTI would be beneficial for clinical implementation because of its considerable scan time reduction compared to s-DTI. Moreover, the significant increase in quantitative parameters in mb-DTI may be the result of higher signal-to-noise ratio compared to s-DTI, which may suggest that mb-DTI can allow for more accurate and sensitive presurgical planning for white matter tracts compared to s-DTI.Conclusion
As a result, this study demonstrated the clinical feasibility of utilizing mb-DTI for presurgical planning in patients with brain tumor. The reduced scan time of mb-DTI along with its similar image quality and quantitative diffusion parameters to s-DTI for analyzing two white matter tracts particularly important during presurgical planning suggest clinical advantages for utilizing mb-DTI over current techniques.Acknowledgements
No acknowledgement found.References
1) Maudsley AA. Multiple‐line‐scanning spin‐density imaging. J Magn Reson 1980; 41:112–126. 2) Müller S. Multifrequency Selective RF Pulses for Multislice MR Imaging. Magn Reson Med 1988; 6:364–371. 3) Mitsuda et al., Feasibility of Diffusion Tensor Imaging at 1.5T Using Multi-Band Echo Planar Acquisition. Magn Reson Med Sci. 2017; 16(2): 169–175. 4) Wen Q et al., Clinically feasible NODDI characterization of glioma using multiband EPI at 7 T. Neuroimage Clin. 2015 Sep 3;9:291-9Figures
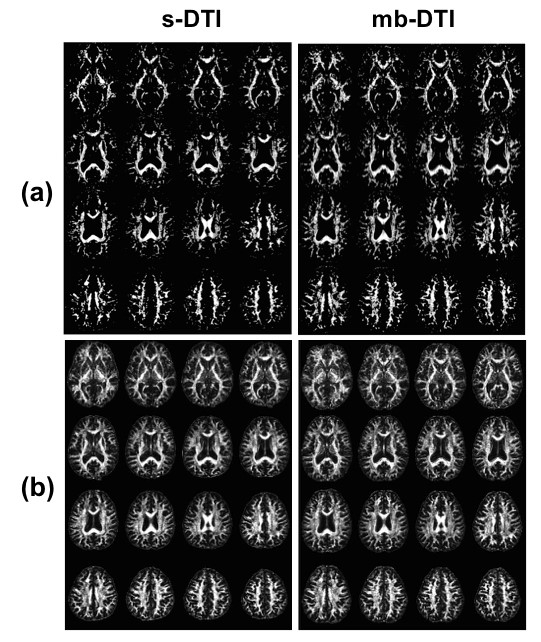
Figure 1 shows the
fractional anisotropy (FA) maps obtained using standard diffusion tensor
imaging (s-DTI) and multi-band DTI (mb-DTI) at a minimum threshold of 0.2 (a)
and 0.5 (b) for the same patient. The maps obtained using mb-DTI show slightly
greater sensitivity and elucidation of white matter tracts than s-DTI at both
thresholds.
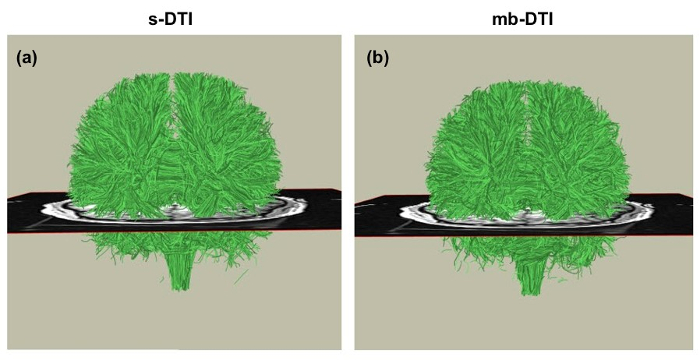
Figure 2 shows whole-brain
tractography analysis using standard diffusion tensor imaging (s-DTI) (a) and
multi-band DTI (mb-DTI) (b). Qualitative inspection shows that mb-DTI produced
very similar images to s-DTI.
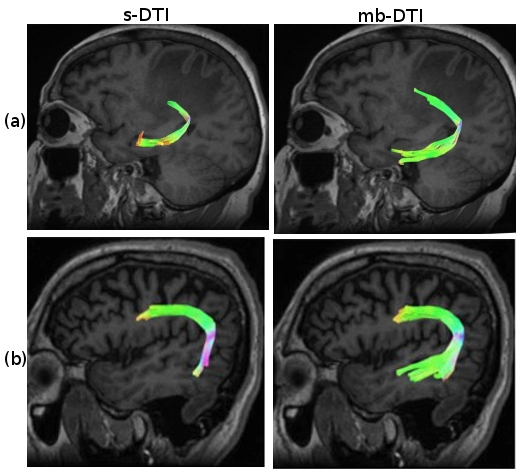
Figure
3 compares tractography analysis of the arcuate fasciculus using standard
diffusion tensor imaging (s-DTI) and multi-band DTI (mb-DTI) in two patients.
There was greater elucidation of the arcuate fasciculus using mb-DTI compared
to s-DTI in both patients.
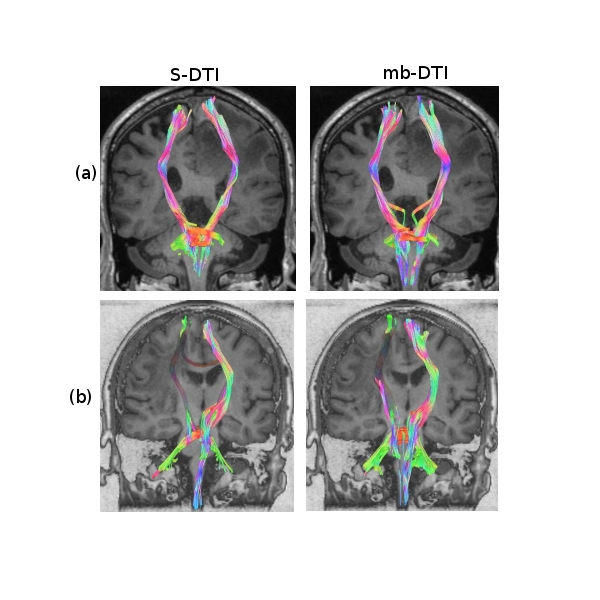
Figure 4 compares the
tractography analysis of the corticospinal tract using standard diffusion
tensor imaging (s-DTI) (a) and multi-band diffusion tensor imaging (mb-DTI)
(b). Qualitative inspection shows that mb-DTI produces very similar images to
s-DTI.
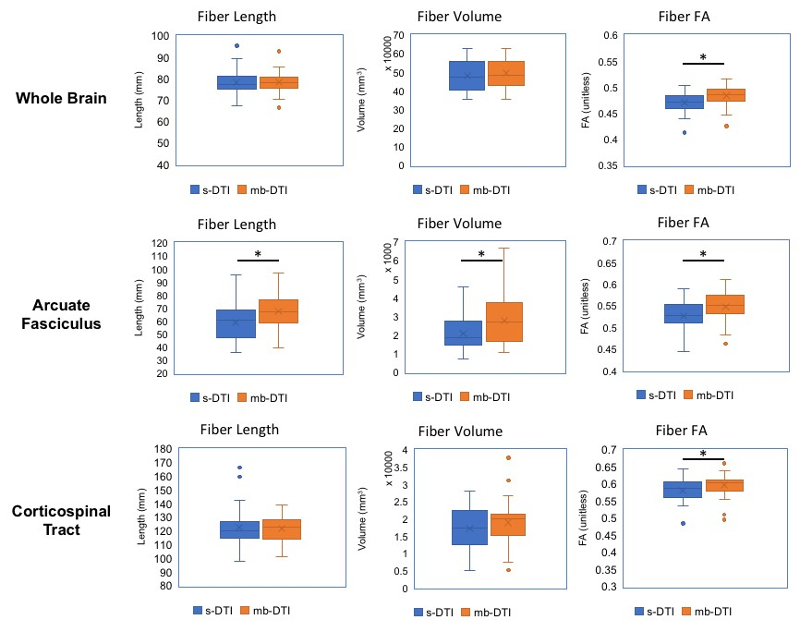
Figure
5 shows the box-and-whisker plot analysis for the quantitative diffusion
parameters of fiber length, volume, and fractional anisotropy (FA) using
standard diffusion tensor imaging (s-DTI) and multi-band DTI (mb-DTI). The
parameters were slightly higher for mb-DTI than in s-DTI for nearly all
subjects. An asterisk (*) denotes a statistically significant difference of
p<0.0001.