3530
Golden-Angle Rotating Single-Shot Acquisition (GA-RoSA) for Simultaneous High-Resolution DTI and IVIM1Indiana University, School of Medicine, Indianapolis, IN, United States, 2Department of Medical Physics, Memorial Sloan-Kettering Cancer Center, New York, NY, United States, 3Siemens Shenzhen Magnetic Resonance Ltd., Shenzhen, China, 4Siemens Medical Solutions, Inc., Chicago, IL, United States
Synopsis
High-resolution DWI often relies on multi-shot acquisitions, which suffer from long acquisition time and motion-related phase variations. Although effort has been made to accelerate DWI acquisitions, acquiring b=0 images still requires multiple shots and multiple averages. In this work, in addition to accelerating DWI acquisitions, the proposed method (GA-RoSA) further rearranged the b=0 acquisitions to cover a range of lower b-values without increasing scan times, so that IVIM parameters can be obtained for free. With a golden-angle rotation scheme, GA-RoSA introduced sampling incoherence facilitating its combination with sparsity-based reconstruction approaches. We demonstrated its feasibility for simultaneous high-resolution DTI and IVIM.
Introduction
High-resolution (1×1mm2 or higher) diffusion tensor imaging (DTI) is challenging with standard single-shot echo planar imaging (SS-EPI) due to long TE and sever geometric distortion. Multi-shot techniques1-3 can be applied to partially address this issue but with prolonged acquisition times and additional corrections of between-shot phase variations. A rotating single-shot acquisition (RoSA) was previously proposed, where one blade is acquired per diffusion direction, and the q-space correlations are exploited for image reconstruction.4-5 Despite great acceleration in DWIs, acquisition of b=0s/mm2 images (b=0) with multiple averages are required for reliable tensor fitting, which is still time-consuming and is a common limitation in all existing multi-shot techniques. In this work, we proposed a new q-space design where the multiple shots of b=0 images are ‘spread out’ to cover a range of b-values (≤ 800s/mm2). Thus, DTI and IVIM can be obtained simultaneous without increasing scan times.Methods
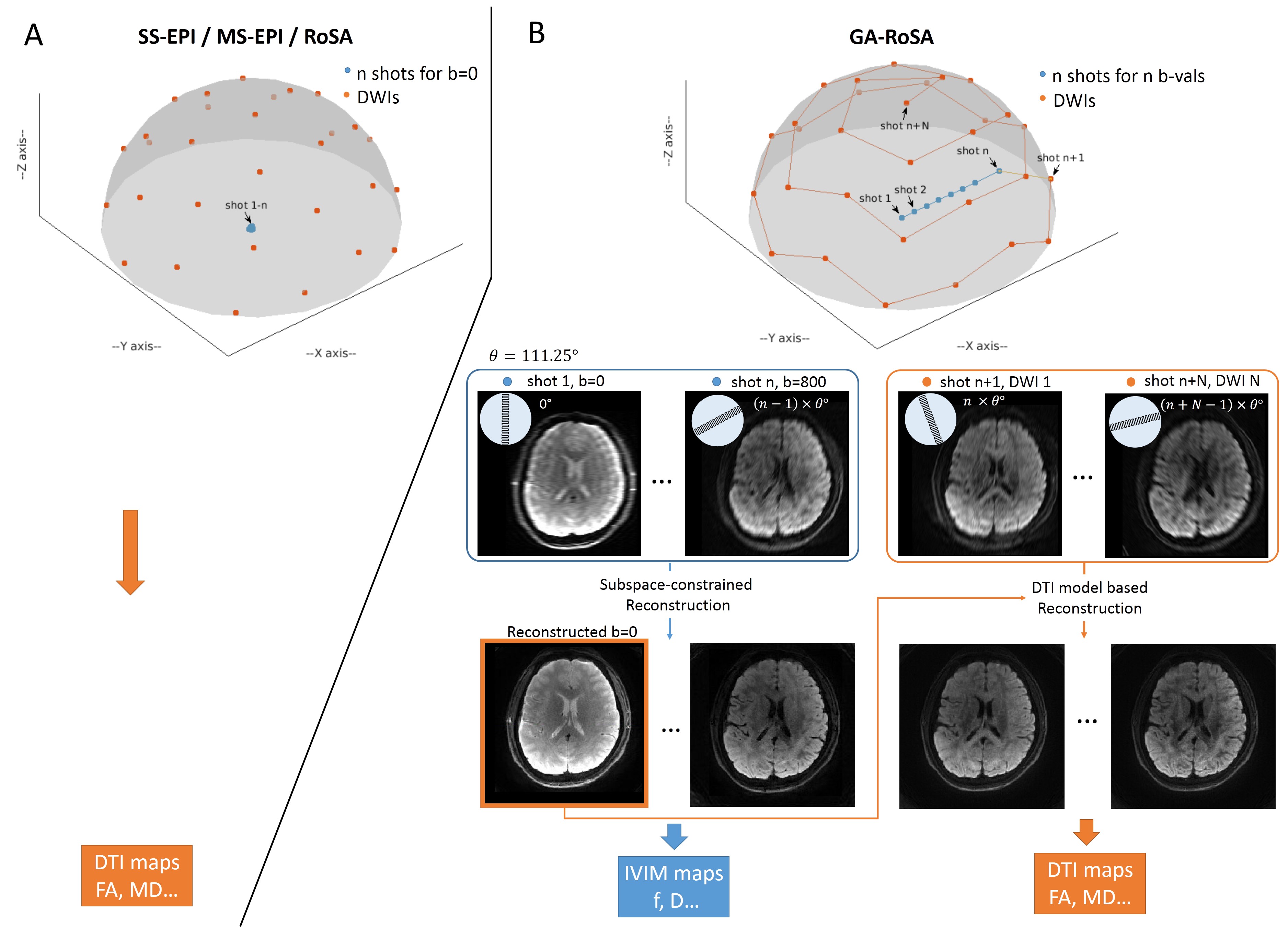
Q-space design: Contrast to conventional DTI acquisition where n shots are acquired for b=0 images (Figure 1A), we use n shots to sample n b-values (≤ 800s/mm2) in a single direction (arbitrary direction) (Figure 1B). The signals along these b-values are known to follow the bi-exponential decay, which was contributed by both blood flow and water diffusion, known as the IVIM.6 To better sensitize signals to blood flow, more shots were placed towards the lower b-values. The rest N diffusion directions for DTI were evenly distributed on one shell.
GA-RoSA trajectory: One short-axis EPI blade was acquired for each point in the design. Thus, each blade corresponds to a blurred image with full resolution in the phase-encoding direction (Figure 1B). The blade was rotating at golden-angle to introduce incoherent blurring between neighboring directions. Parallel imaging (e.g. GRAPPA) was combined to further accelerate the blade acquisition.
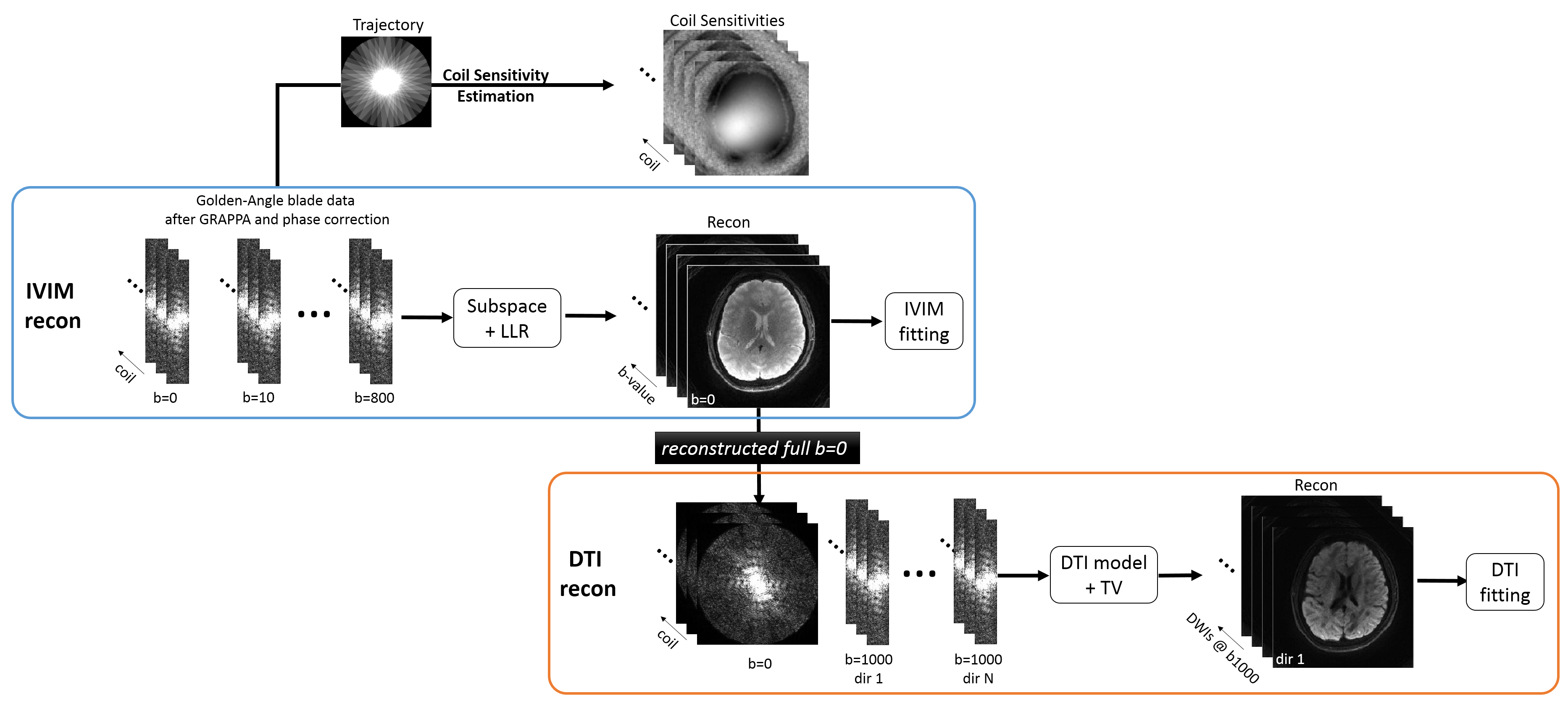
Reconstruction: Each blade was first independently processed with GRAPPA reconstruction and phase removal.4,7 Then they were fed into special IVIM and DTI reconstruction sequentially.
IVIM (Figure 2 blue window): n blades from n b-values were first reconstructed by constraining the signal evolution to a bi-exponential decay and further to a low-dimensional subspace, similar to a previous method.8-9 . After image reconstruction, IVIM model was fitted to produce the flow fraction (f) and water diffusion coefficient (D).
DTI (Figure 2 orange window): N blades from N diffusion directions, along with the reconstructed high-quality b=0 image from the IVIM were fed into a model-based reconstruction where the six maps of the diffusion tensor elements (upper triangle of 3×3 tensor matrix) were directly estimated in iterative reconstruction, similar to a previous work.10 Thereafter, DTI maps were produced.
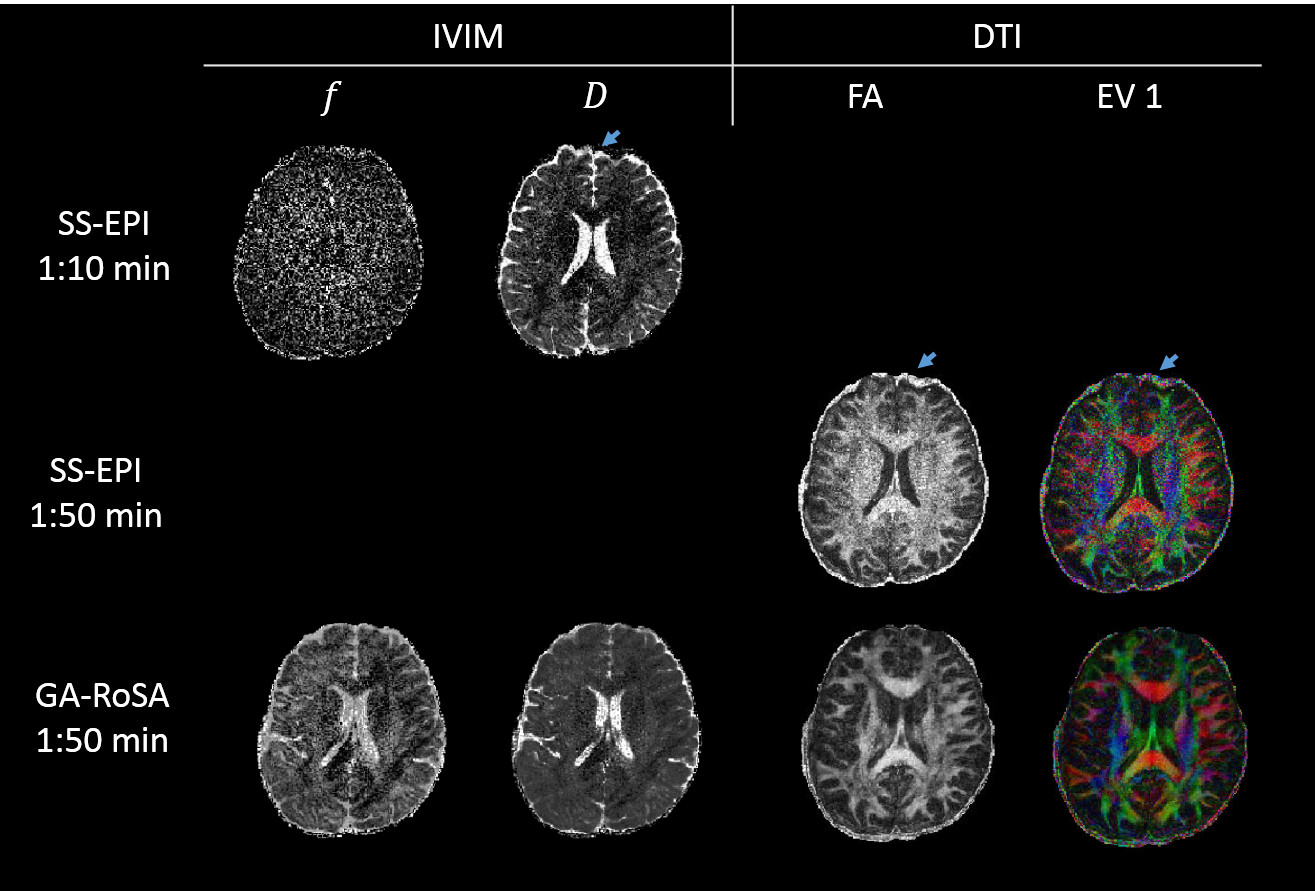
Human data: GA-RoSA was performed on a health volunteer at a 3.0T Siemens Prisma scanner with a 32-channel head coil with 1×1mm2 in-plane resolution. 18 unique b-values ranging from 0-800s/mm2 along the x-axis were sampled and the b=1000s/mm2 DWIs were acquired along 30 directions. Other parameters included: blade size=224×40, GRAPPA=3, 24 slices, TR=2000ms, acquisition time=1:50min. For comparison, SS-EPI was acquired with matching parameters, including b-values (with 2 extra b=0), diffusion directions, resolution, GRAPPA acceleration and slice coverage. TR was 3500ms and the total acquisition time was 3 min (1:50min for DTI, 1:10min for IVIM).
Results
Figure 3 shows fitted maps of f, D, FA and major eigen-value (EV1) with SS-EPI and GA-RoSA. Higher quality in all maps could be appreciated in GA-RoSA scheme, whose acquisition time was just enough for SS-EPI to get DTI. The lower SNR in SS-EPI was due to the prolonged TE (95ms as compared to 55ms in GA-RoSA). Furthermore, obvious distortion in the frontal lobe (blue arrow) could be seen in SS-EPI but not in GA-RoSA, due to significantly reduced echo spacing in GA-RoSA (0.34ms as compared to 0.95ms in SS-EPI).Discussion
GA-RoSA is an efficient and flexible high-resolution diffusion imaging technique that allows simultaneous DTI and IVIM. Instead of acquiring b=0 images in multi-shot, GA-RoSA expands this acquisition to cover a range of b-values without increasing scan times, so that IVIM can be obtained for free. A subspace-constraint reconstruction strategy and a model-based reconstruction technique are used for the IVIM and DTI reconstruction, respectively, to ensure good reconstruction performance and image quality. GA-RoSA has shown improved scan efficiency compared to conventional SS-EPI with higher SNR and less distortion, and it does not require navigator data for phase correction. With a golden-angle rotation scheme, GA-RoSA introduced sampling incoherence facilitating its combination with different sparsity-based reconstruction approaches. Although DTI results were presented, GA-RoSA can also be applied to other types of diffusion imaging, including parametric and non-parametric q-space approaches with composite reconstruction as described in the original RoSA study.4 We aim to demonstrate such versatility in both healthy subjects and different disease conditions in future work.Acknowledgements
The authors thank Peng Cao (University of Hong Kong) for the inspiring discussions and Siemens Research Support.This work was supported by Grants NIH NIA R01 AG053993.References
- Skare S, Newbould RD, Clayton DB, Bammer R. Propeller EPI in the other direction. Magn Reson Med. 2006 Jun;55(6):1298-307.
- Porter DA, Heidemann RM. High resolution diffusion-weighted imaging using readout-segmented echo-planar imaging, parallel imaging and a twodimensional navigator-based reacquisition. Magn Reson Med. 2009 Aug;62(2):468-75.
- Nan-kuei Chen, Arnaud Guidon, Hing-Chiu Chang, and Allen W. Song. A robust multi-shot scan strategy for high-resolution diffusion weighted MRI enabled by multiplexed sensitivity-encoding (MUSE). Neuroimage. 2013 May 15; 72: 41–47.
- Wen Q, Kodiweera C, Dale BM, Shivraman G, Wu YC. Rotating single-shot acquisition (RoSA) with composite reconstruction for fast high-resolution diffusion imaging. Magn Reson Med. 2018 Jan;79(1):264-275.
- Wen Q, Graham M, Drobnjak I, Zhang H, WU YC. Improving angular resolution in multi-shot turbo spin-echo diffusion imaging using rotating single-shot acquisition (RoSA). Proceedings of the 25th Annual Meeting ISMRM, Honolulu, 2017; 0179.
- Le Bihan D, Breton E, Lallemand D, Aubin ML, Vignaud J, Laval-Jeantet M. Separation of diffusion and perfusion in intravoxel incoherent motion MR imaging. Radiology. 1988 Aug;168(2):497-505.
- Pipe
JG, Farthing VG, Forbes KP. Multi-shot diusion-weighted FSE using PROPELLER
MRI. Magn Reson Med. 2002 Jan;47(1):42-52.
- Tamir J, Uecker M, Chen W, Lai P, Alley MT, Vasanawala SS, Lustig M. T2 shuffling: Sharp, multicontrast, volumetric fast spin-echo imaging. Magn Reson Med. 2017 Jan;77(1):180-195.
- Wen Q, Feng L, Zhou K, Wu Y-C. Intravoxel Incoherent Motion (IVIM) Fingerprinting. Proceedings of the 26th Annual Meeting ISMRM, Paris, 2018; 1646.
- Knoll F, Raya JG, Halloran RO, Baete S, Sigmund E, Bammer R, Block T, Otazo R, Sodickson DK. A model-based reconstruction for undersampled radial spin-echo DTI with variational penalties on the diffusion tensor. NMR Biomed. 2015 Mar;28(3):353-66.
Figures